Abstract
Objectives
To assess the pharmacological treatment and the control of major modifiable cardiovascular risk factors in everyday practice according to the patients’ cardiovascular risk level.
Methods
In a cross-sectional study general practitioners (GPs) had to identify a random sample of their patients with cardiovascular risk factors or diseases and collect essential data on the pharmacological treatment and control of hypertension, hyperlipidemia, and diabetes according to the patients’ cardiovascular risk level and history of cardiovascular disease. Participants were subjects of both sexes, aged 40–80 years, with at least one known cardiovascular risk factor or a history of cardiovascular diseases.
Results
From June to December 2000, 162 Italian GPs enrolled 3120 of their patients (2470 hypertensives, 1373 hyperlipidemics, and 604 diabetics). Despite the positive association between the perceived level of global cardiovascular risk and lipid-lowering drug prescriptions in hyperlipidemic subjects (from 26% for lowest risk to 56% for highest risk p < 0.0001) or the prescription of combination therapy in hypertensives (from 41% to 70%, p < 0.0001) and diabetics (from 24% to 43%, p = 0.057), control was still inadequate in 48% of diabetics, 77% of hypertensives, and 85% of hyperlipidemics, with no increase in patients at highest risk. Trends for treatment and control were similar in patients with cardiovascular diseases.
Conclusions
Even in high-risk patients, despite a tendency towards more intensive treatment, pharmacological therapy is still under used and the degree of control of blood pressure, cholesterol level and diabetes is largely unsatisfactory.
Introduction
Epidemiological surveys consistently report under-utilization of evidence-based preventive treatments and inadequate control of modifiable risk factors in the overall population at cardiovascular risk (CitationDunn and Bough 1996; CitationAvanzini et al 1998; CitationBouma M et al 1999; CitationPrimatesta and Poulter 2000; CitationEUROASPIRE II Study Group 2001; CitationHippisley-Cox and Pringles 2001; CitationPrimatesta et al 2001; CitationGianpaoli and Vanuzzo 2003; CitationPilotto et al 2004; CitationBhatt et al 2006). As the absolute benefits of treatments for the prevention of cardiovascular diseases are directly proportional to patients’ global cardiovascular risk, priority should clearly be given to patients at high risk (CitationWood et al 1998; CitationAnsell et al 1999; CitationEuropean Diabetes Policy Group 1999; 1999 WHO/ISH 1999). However, little information is available, to our knowledge, on the degree of treatment and control of cardiovascular risk factors in relation to patients’ absolute risk (CitationAmar et al 2002; CitationCamisasca et al 2002; CitationLloyd-Jones et al 2002). General practitioners (GPs) identify subjects at high cardiovascular risk properly (CitationRoncaglioni et al 2004), but it is not known whether this perception leads to more intensive treatment and better control of their risk factors.
As part of the feasibility phase of a large intervention study on the optimization of cardiovascular prevention in high-risk patients (Risk & Prevention Study, Clinical Trial.gov number, NCT00317707 [ClinicalTrial.gov]), we ran a pilot epidemiological study to assess the level of treatment and control of the three major modifiable cardiovascular risk factors—arterial hypertension, hyperlipidemia and diabetes—in everyday practice, according to patients’ absolute levels of cardiovascular risk.
Methods
A network of GPs from all over Italy was invited to enter a cross-sectional study on the cardiovascular preventive strategies adopted in everyday practice. General practitioners were members of research working parties who have participated in previous collaborative studies with our Institute. Among all subjects coming to the surgery for any reasons from June to December 2000 each GP identified a random sample of patients aged 40–80 perceived as being at cardiovascular risk because of at least one risk factor or atherosclerotic disease. All patients who met these criteria were consecutively entered in a register in which a random sequence picked out one in ten for inclusion in the study for up to 20 patients. We estimate that a sample of at least 100 general practitioners (GPs) recruiting a total of 2000 patients would have been enough to detect the percentage of control of major risk factors in the four pre-specified risk level categories, with sufficient accuracy.
GPs had to collect data on cardiovascular risk factors (history of hypertension, diabetes, hyperlipidemia, if patients were obese, current smokers, or had a family history of premature myocardial infarction) and on the history of cardiovascular diseases (CVD) including myocardial infarction (MI), angina pectoris, arterial revascularization procedures (CABG or PTCA), stroke, transient ischemic attack (TIA), peripheral arterial occlusive disease (PAOD), GPs were also asked to do a physical examination (including measuring blood pressure [BP], height, and weight) and record the results of recent laboratory tests (plasma lipids and glucose in all patients and HbA1c in diabetics). On the basis of all the data, GPs were asked to subjectively estimate for each patient the overall level of cardiovascular risk, rating it as mild, moderate, high, or very high (CitationRoncaglioni et al 2004). Patients’ risk was also classified according to whether they already had a history of CVD.
Hypertensives were considered well-controlled when BP was <140/90 mmHg if not diabetics, and <130/80 mmHg if diabetics; hyperlipidemics when total plasma cholesterol was <190 mg/dL and diabetics when blood HbA1c was ≤7.5 mg% (CitationWood 1998).
In interpreting the use of lipid-lowering drugs we must bear in mind the restrictions on their prescription imposed by the Italian National Health Service in patients at low-moderate cardiovascular risk.
Statistical analysis
Descriptive results are expressed as numbers and percentages. The proportions of subjects treated and controlled, with or without CVD, were compared using the χ2 test. The same analysis according to the level of risk was done using the χ2 test for trend. Tests were two-sided and a value of p < 0.05 was considered significant. Statistical analyses were done using the statistical package SAS® (SAS Institute, Cary, NC).
Results
A total of 162 GPs took part in this study and recruited 3120 patients between June and December 2000. As a whole, 41% of this population had a history of CVD; 40% had 3 or more risk factors, 15% had 2, and 4% had just 1 risk factor.
A BP measure was available in all 2470 hypertensives, a recent measure of total plasma cholesterol was available in 1373 out of 1627 hyperlipidemics (84%) and blood HbA1c in 604 out of 635 diabetics (95%). Only patients with complete data (2914) were included in the present analysis and their characteristics are shown in . shows the distribution of hypertensive, hyperlipidemic, and diabetic patients according to the level of global cardiovascular risk perceived by their GP and the presence of CVD.
Table 1 Main characteristics of the populationTable Footnotea
Table 2 Distribution of hypertensive, hyperlipidaemic and diabetic patients according to the level of global cardiovascular risk perceived by GPs and the history of cardiovascular disease
Preventive treatment of risk factors
shows the rate of specific pharmacological treatments of patients with risk factors; 96% of hypertensives were pharmacologically treated, 78% of diabetics, and 46% of hyperlipidemics.
Figure 1 Treatment and control of hypertension, hyperlipidemia, and diabetes
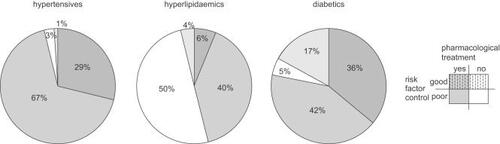
ACE-inhibitors, diuretics, and calcium antagonists were the drugs most frequently used in hypertensive patients, respectively in 53%, 47%, and 39%; 62% of hypertensive patients were treated with 2 or more drugs. In hyperlipidemic patients, statins were the drugs most used (87%); 1% received a combination of 2 drugs. Among diabetic patients 40% were treated with monotherapy (22% with sulphonylureas, 6% biguanides, 11% insulin, and 1% acarbose); 38% received a combination.
shows the relation between the prescription of preventive drug therapy and GPs’ risk perception. In hyperlipidemic subjects, there was a significant pattern in the treatment rate, rising from 27% of patients perceived to be at low risk to 61% of subjects at very high cardiovascular risk (p < 0.0001). In hypertensive and diabetic patients there was a trend between the number of drugs prescribed and GPs’ risk perception (p < 0.0001 for hypertensives; p = 0.057 for diabetics).
Figure 2 Drug therapy in hypertension, hyperlipidemia, and diabetics according to level of global cardiovascular risk perceived by GPs (A) and the history of cardiovascular disease (CVD) (B)
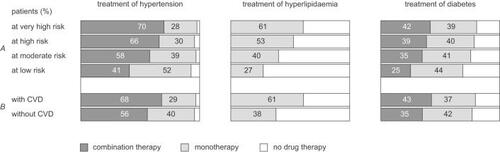
A similar pattern was found on analyzing the drug prescriptions according to the presence of CVD (B). The numbers of hyperlipidemics given drugs and of hypertensive and diabetics treated with a combination therapy were higher in patients with CVD: from 38% up to 61% in hyperlipidemics (p < 0.0001), from 56% up to 68% in hypertensives (p < 0.0001), and from 35% up to 43% in diabetics (p = 0.0633).
The presence and intensity of treatment of each risk factor was not influenced by the concomitant use of drugs for the other two risk factors: two or more drugs were used in 59% of cases when hypertension was the only risk factor, in 58% of patients also using statins or antidiabetic drugs and in 64% of those taking both. Findings were similar in diabetic patients and hyperlypidemics.
Control of risk factors
Overall, control was adequate in 55% of diabetics, 29% of hypertensives, and 10% of hyperlipidemics. shows the levels of control according to GPs’ subjective risk grading. Control was not better in hypertensive and hyperlipidemic patients perceived at higher risk, and in diabetics, control was significantly worse in patients at higher cardiovascular risk (p < 0.0001).
Figure 3 Control of hypertension, hyperlipidemia, and diabetes according to level of global cardiovascular risk perceived by GPs and the history of cardiovascular disease (CVD)
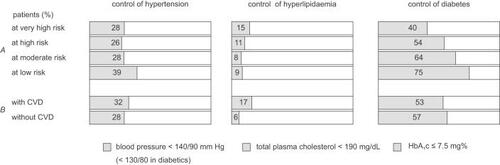
Analyzing data according to the history of CVD, no significant differences in the rate of control of hypertensive and diabetic patients were observed; a higher rate of control was found in hyperlipidemic patients with CVD in respect to those without (17% vs 6%, p < 0.001).
Pharmacological therapy to control hyperlipidemia was more frequently required in patients at high or very high cardiovascular risk (72%) than in patients at low or moderate risk (48%). Analagously, to control hypertension and diabetes, combination therapies were more frequently required in patients at high or very high cardiovascular risk (66% and 32%, respectively) than in patients at low or moderate risk (55% and 25%, respectively). Similar results were found on analyzing the pharmacological therapy required to control the three risk factors according to the presence of CVD.
Among subjects at high or very high cardiovascular risk, 48% with uncontrolled hyperlipidemia were not receiving drug therapy, and 33% and 52%, respectively, with uncontrolled hypertension and diabetes were receiving no drugs or monotherapy. Similar results were found on analyzing subjects with established CVD and uncontrolled risk factors Being under chronic therapy for other cardio-vascular risk factors at the same time did not significantly change the rate of control of the risk factor considered.
Discussion
This study clearly shows how in daily practice many effective strategies to prevent cardiovascular diseases are still under used even in patients at high cardiovascular risk.
In fact, despite the proportion of hyperlipidemics treated with lipid-lowering agents and of diabetics and hypertensives using combination therapies was higher in patients at higher risk or with previous CVD, this is still inadequate to reach the therapeutic goals in the majority of patients.
Besides confirming other findings on the overall low rate of control of hypertension, hyperlipidemia and diabetes in current practice (CitationBouma M et al 1999; CitationDunn and Bough 1996; CitationAvanzini et al 1998; CitationPrimatesta and Poulter 2000; CitationEUROASPIRE II Study Group 2001; CitationHippisley-Cox and Pringles 2001; CitationPrimatesta et al 2001; CitationGianpaoli and Vanuzzo 2003; CitationPilotto et al 2004; CitationBhatt et al 2006), the lack of control even in patients at higher risk of developing CVD in a short time proves that the global level of risk has not yet become a fundamental tool for the implementation of preventive strategies in everyday practice. The consequences are epidemiologically important considering the prevalence of patients at high cardiovascular risk: in our population half of hypertensives and hyperlipidemics and two out of three diabetics were considered by their GP to be at high or very high risk of CVD in the next few years, while over a quarter of patients with hypertension and over a third of those with diabetes and hyperlipidemia had already suffered a CVD. The fact that some of them are likely to have more severe forms of hypertension, hyperlipidemia, and diabetes, often with target organ damage or concomitant diseases, means they need much more aggressive treatment to obtain all the possible benefits. The large margin for improvement is documented by the fact that one out of three uncontrolled hypertensives and half the uncontrolled diabetics at higher cardiovascular risk were given monotherapy or no drugs at all, and that half the uncontrolled hyperlipidemics at higher risk were not treated. Although we did not collect data on non-pharmacological treatments, it is likely that a closer life style management could significantly improve the control of hypertension, hyperlipidemia and diabetes. There have been many reports that aggressive treatment of risk factors can lead to an optimal level of control in the majority of patients at high cardiovascular risk (CitationUK Prospective Diabetes Study (UKPDS) Group 1998a, Citation1998b; CitationPROGRESS Collaborative Group 2001; CitationHeart Protection Study Collaborative Group 2002; CitationPepine et al 2003; CitationCannon et al 2004); however, these data come from clinical trials, where compliance is expected to be better than in routine practice. We collected no data on this point in our survey, but the far-from-optimal level of control of modifiable risk factors might actually reflect not only the GPs’ attitude to prescribing preventive treatments but also the patients’ resistance to taking numerous pills for asymptomatic conditions or poor compliance anyway in the long term. Compliance with preventive treatments would probably increase if people were more aware of their risks (CitationFerrario et al 2004), and more information from GPs on the long-term benefits of preventive drugs could reduce the fear of lifelong therapies.
The absence of any negative interaction in our patients among the drugs used for hypertension, diabetes and hyperlipidemia should make it possible to optimise these therapies even in patients at high cardiovascular risk because of several simultaneous risk factors. The possibility of using poly-pills, which combine in the same pill different drugs to control several risk factors simultaneously, may help make the treatment of multiple risk factors easier and more acceptable (CitationWald and Law 2003; CitationSleight et al 2006). In addition, the imminent arrival of generic statins might mitigate the current Italian restriction and could favour their use also in patients with a lower level of risk (CitationMoon 2006).
Apart from GPs’ and patients’ roles, the presence of specific contraindications and the appearance of side effects may affect the use of preventive drug treatments. However, the large selection of different pharmacological approaches available to control hypertension, hyperlipidemia and diabetes means that only a tiny minority are due to these reasons.
One limitation of this study was the selection of the population at cardiovascular risk among people coming to their family doctor for any reason. This could have favored the inclusion of subjects with uncontrolled risk factors. Otherwise, these subjects are expected to be more willing to take drugs and to follow GPs’ advice, too. Anyway this is the population that would receive immediate benefit if GPs took a more “aggressive” preventive attitude.
Another possible limit is the unusual way of defining the level of cardiovascular risk. We preferred to classify the patients’ risk according to the GPs’ perception because in a previous analysis we had found these estimates were not only associated with the patients’ level of risk but were also independent of the levels of single risk factors, such as BP or blood cholesterol (CitationRoncaglioni et al 2004). The use of algorithms or charts would have favored the inclusion of uncontrolled hypertensive and hyperlipidemic patients in the high or very high risk categories. In order to overcome this possible bias, we also classified our population according to their clinical history of CVD, a recognized way to identify people at higher risk, obtaining similar results.
A third limit of the study is that participating GPs do not necessarily represent all Italian GPs. However, it is likely that GPs who participated voluntarily and without any financial incentive were those who managed risk factors better and were more used to complying with recommendations. Thus our results probably provide an optimistic estimate of the real behavior.
In conclusion, the central finding of this study is that in current practice even in high-risk patients, despite a tendency towards more intensive treatment, pharmacological therapy is still under used and the degree of control of blood pressure, cholesterol level and diabetes is largely unsatisfactory. This leads to the paradox that despite the number of effective treatments available, subjects at higher risk of CVD in the short term get little benefit from them. To identify the main reasons for this and how best to solve it would greatly improve the effectiveness of cardiovascular preventive treatments and the prognosis of a large number of people. These are the aims of a prospective trial on the optimisation of cardiovascular prevention in patients at high cardiovascular risk that is currently going on after this epidemiological feasibility phase.
Acknowledgements
We thank F Clerici, G Sgaroni, and A Palumbo for careful secretarial assistance in the management of the study and help in preparing the paper and J Baggott for editorial assistance.
Disclosures
The authors have no conflicts of interest to disclose. An educational grant was provided by Pharmacia Upjohn and Società Prodotti Antibiotici (SPA) for the co-ordination expenses.
References
- AmarJVaurLPerretMon behalf of the PRATIK Study investigatorsHypertension in high-risk patients: beware of the underuse of effective combination therapy (results of the PRATIK Study)J Hypertens2002207798411910316
- AnsellBJWatsonKEFogelmanAMAn evidence-based assessment of the NCEP adult treatment panel II guidelinesJAMA199928220515710591388
- AvanziniFAlliCColomboPon behalf of the Physicians taking part in STAPControl of hypertension in Italy: results of the “Study on Antihypertensive Treatment in General Practice (STAP)”G Ital Cardiol19982876069773300
- BhattDLStegPGOhmanEMInternational prevalence, recognition, and treatment of cardiovascular risk factors in outpatients with atherothrombosisJAMA2006295180916403930
- BoumaMDekkerJHvan EiikJThMMetabolic control and morbidity of type 2 diabetic patients in a general practice networkFam Pract199916402610493712
- CamisascaPAvanziniFAlliCon behalf of the “Studio sul Trattamento Antipertensivo nella Pratica ambulatoriale (STAP)” participantsOverall cardiovascular risk still ignored in general practice care of hypertensionJ Cardiovasc Risk200291475212202837
- CannonPCBraunwaldEMcCabeCHIntensive versus moderate lipid lowering with statins after acute coronary sindromesN Engl J Med2004350149550415007110
- DunnNRBoughPStandards of care of diabetic patients in a typical English communityBr J Gen Pract19964640158776910
- EUROASPIRE II Study GroupLifestyle and risk factor management and use of drug therapies in coronary patients from 15 countries; principal results from EUROASPIRE II Euro Heart Survey ProgrammeEur Heart J2001225547211259143
- European Diabetes Policy GroupA desktop guide to type 2 diabetes mellitusDiabetic Med1999167163010510947
- FerrarioGAlkhimovitchOAvanziniFPeoples’ perception of their overall coronary risk: an Italian experienceItal Heart J20045162115080576
- GianpaoliSVanuzzoDItalian Atlas of Cardiovascular DiseasesItal Heart J200341st edSuppl 41S121S
- Heart Protection Study Collaborative GroupMRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20536 high-risk individuals: a randomised placebo-controlled trialLancet200236072212114036
- Hippisley-CoxPringle MGeneral practice workload implications of the national service framework for coronary heart disease: cross sectional surveyBMJ20013232697011485958
- Lloyd-JonesDMEvansJCLarsonMGTreatment and control of hypertension in the community. A prospective analysisHypertension200240640612411456
- MoonJCSwitching statins. Using generic simvastatin as first line could save £2bn over five years in EnglandBMJ20063321344516763226
- PepineCJHandbergEMCooper-DeHoffRMA calcium antagonist vs a non-calcium antagonist hypertension treatment strategy for patients with coronary artery disease. The International Verapamil-Trandolapril Study (INVEST): a randomized controlled trialJAMA200329028051614657064
- PilottoLGiaggioliALo NoceCIl diabete in Italia: un problema di sanità pubblicaItal Heart J Suppl20045480615471153
- PrimatestaPBrookesMPoulterNRImproved hypertension management and control: results from the heath survey for England 1998Hypertension2001388273211641294
- PrimatestaPPoulterNRLipid concentrations and the use of lipid-lowering drugs: evidence from a national cross-sectional surveyBMJ20003211322511090516
- PROGRESS Collaborative GroupRandomised trial of a perindopril-based blood-pressure-lowering regimen among 6105 individuals with previous stroke or transient ischaemic attackLancet200135810334111589932
- RoncaglioniMCAvanziniFRoccatagliataDHow general practitioners perceive and grade the cardiovascular risk of their patientsEur J Cardiovasc Prev Rehabil200411233815179106
- SleightPPouleurHZannadFBenefits, challenges, and registerability of the polypillEur Heart J2006271651–616603580
- UK Prospective Diabetes Study (UKPDS) GroupIntensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33)Lancet1998352837539742976
- UK Prospective Diabetes Study (UKPDS) GroupEffect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34)Lancet1998352854659742977
- WaldNJLawMRA strategy to reduce cardiovascular disease by more than 80%BMJ200332616
- WoodDDe BackerGFaergemanOtogether with members of the Task ForcePrevention of coronary heart disease in clinical practice. Recommendations of the Second Joint Task Force of European and other Societies on Coronary PreventionEur Heart J199819143415039820987
- 1999 World Health Organization/International Society of Hypertension Guidelines for management of hypertensionJ Hypertens1999171518310067786
Appendix
General practitioners
Adinolfi D. (Pozzuoli); Agneta A. (Montalbano Jonico); Alberino S. (Chiusdino); Alexanian A. (Milano); Anglano B. (Parona-Verona); Aronica A. (Milano); Bagagli F. (Torino); Balzan C. (Trichiana); Barba G. (Talsano); Baron P. (Palmanova); Barone A. (Albano di Lucania); Bedon R. (Casale Monferrato); Benetti R. (Casale sul Sile); Berton G. (Castelfranco Veneto); Besozzi E. (Castelletto sopra Ticino); Bevilacqua S. (Viterbo); Bizzarri G. (Cannara); Boldini L. (Torbole Casaglia); Bonzi G. (Ostiano); Bosisio Pioltelli M. (Monza); Bozzetto R.M. (Breganze); Brocchi A. (Cortona); Brizzi A. (Terlizzi); Bruno B. (Montereale); Burbi M. (Cortona); Buzzatti A. (Sedico); Cadioli T. (Carpi); Caimi V. (Monza); Calciano F.P. (Grassano); Calienno S. (Monza); Caltagirone P. (Castelnuovo di Isola Vic.); Capelli O. (Montefiorino); Casella M. (Caserta); Casella P. (Caserta); Caso C. (Mercato San Severino); Cassanelli M. (Castelfranco Emilia); Catalano A. (San Leucio del Sannio); Ciociano C. (Sarno); Coazzoli E. (Milano); Colecchia G. (Massa); Colombo I. (Boffalora sul Ticino); Conti M. (Castiglion Fiorentino); Corti N. (Scandiano); Corvino P. (Caserta); Cotroneo S. (Villa San Giovanni); Cozzani L. (Ponte di Arcola); Cuffari A. (Marino); Cuozzo E. (Napoli); Cusmai L. (Foggia); D’Anna M.A. (Milano); Danti G. (Buttapietra); De Cesare G. (Caserta); De Maria E. (Napoli); De Maria R. (Milano); De Matteis D. (Belvedere Spinello); Del Carlo A. (Viareggio); Dell’Aquila A.M. (Caserta); De Sire G. (Caserta); Di Giovambattista E. (Magnano in Riviera); Di Giuseppe M. (Carnate); Dionette M.G. (Scano di Montiferro); Ermacora T. (Maiano); Fastidio M. (Milano); Ferrari V. (Parabita); Ferreri A. (Cigoli San Miniato Basso); Filippi S. (Pontremoli); Fortunato S. (Montoro Inferiore); Fossati B. (Monza); Fumagalli M.A. (Senago); Galimberti G. (Como); Galli G. (Licciana Nardi); Galopin T. (Verona); Gambarelli L. (Scandiano); Gangi F. (Pasian di Prato); Gardinale E. (Milano); Gasparin A. (Pordenone); Gasparri R. (Mansue’); Gelardi M. (Urbino); Gentile M. (Terni); Germano S. (Avola); Germini F. (Perugia); Giugliano R. (Pozzuoli); Guerra C. (Aprilia); Guerrini A. (Piangipane); Idone A. (Catona); Lattuada G. (Uboldo); Lippa L. (Avezzano); Lombardi P. (Milano); Longoni P. (Milano); Lorello M. (Napoli); Maggioni A. (Ala); Malavasi P. (Carpi); Manni A. (Scandiano); Mao M. (Torino); Marazzi M. (Mirandola); Mariangeloni A. (Terontola); Maruzzi G. (Cantù); Masperi M. (Abbiategrasso); Massa E. (Cittadella); Mastella M. (Foza); Mezzacapo G. (Veroli); Mingarelli C. (Aprilia); Mingione F. (Puccianiello); Minotta F. (Pozzuoli); Misiani V. (Reggio Calabria); Montecchio G. (Abbiategrasso); Moretti S. (Caserta); Morini M. (Cotignola); Moro A. (Preganziol); Nasorri R. (Terontola); Nicoli S. (Borgo di Terzo); Nicolosi M. (Torino); Orlando V. (Caserta); Paci C. (Gioia del Colle); Palatella A. (Foggia); Panigada M. (Bergamo); Panza E.G. (Bollate); Parini P.C. (Vittuone); Paroli G. (Galleno); Patafio M. (Scilla); Pedroni M. (Scandiano); Perone V. (Caserta); Perugini I. (Capranica); Petrera L. (Castellaneta); Piazza G. (Santorso); Piccolo F. (Bisceglie); Pignatti M. (S. Giovanni in Persiceto); Pinto D. (Monopoli); Pirovano E. (Milano); Pirrotta D. (Scilla); Pulcino Lupo G. (Caserta); Rafanelli P. (Firenze); Ramunni A. (Conversano); Recusani A. (Parma); Ribetto Bruno M. (Villar Perosa); Ricciarini P. (Lucignano); Rinchi F. (Cortona); Riva M.G. (Monza); Rossi C. (Casagiove); Rossi R. (Urbino); Rossitto A. (Taranto); Russo V. (Pozzuoli); Sagnelli C. (Maddaloni); Savignano L.C. (Casagiove); Scattolari G. (Urbino); Sissa F. (Virgilio); Sizzano E. (Trivero); Sproviero A.M. (Pozzuoli); Sproviero S. (Pozzuoli); Stranges M. (Caserta); Talia R. (Villa San Giovanni); Tedesco A. (Guradavalle); Titta G. (Torino); Tomba A. (Valdagno); Tosetti C. (Porretta Terme); Uberti M. (Torino); Vece R. (Eboli); Vincenti G. (Sarzana); Visentini E. (Sant’Angelo di Piove di Sacco); Vitali F. (Castiglione del Lago); Vitaloni E. (Abbiategrasso); Zannier P. (San Giuliano Milanese); Zappone P. (Palmi); Ziccardi F. (San Clemente); Zitiello V. (San Marco Evangelista); Zizzo F. (Lissone); Zorzi C. (Ziano di Fiemme).
Data management and statistics: Clerici F.1, Colombo F.1, Barlera S.1, Palumbo A.1, Sgaroni G.1
Scientific Committee: Aronica A.3, Avanzini F.1, Caimi V.4, Lauri D.1, Longoni P.3, Marchioli R.2, Monesi L.1, Roccatagliata D.1, Roncaglioni MC.1, Tognoni G.1, Tombesi M.4, Visconti M.3
1Istituto di Ricerche Farmacologiche “Mario Negri”, Milano; 2Consorzio “Mario Negri Sud”, Santa Maria Imbaro; 3CoS, Milano; 4CSeRMEG, Monza.