Abstract
Hypertension is a major risk factor for the development of cardiovascular and renal disease. The incidence of hypertension is increasing globally and the rate of blood pressure control remains inadequate. Renin-angiotensin-aldosterone system (RAAS) plays a crucial role in volume regulation and maintenance of blood pressure. Pathological activation of RAAS results in chronic hypertension and consequent end organ damage. Most patients with hypertension require combination therapy using agents with complimentary mechanisms of action. Hydrochlorothiazide (HCTZ) together with an agent blocking the RAAS such as an angiotensin converting enzyme (ACE) inhibitor or angiotensin receptor blocker (ARB) are widely used effective anti-hypertensive therapy. Aliskiren is an orally effective direct renin inhibitor that blocks the generation of angiotensin I from angiotensinogen, the rate limiting step of RAAS activation. Studies have shown equivalent antihypertensive efficacy of aliskiren when compared to existing medications such as HCTZ, ACE inhibitors and ARBs. Aliskiren has also been tested in combination therapies. The current review aims to look at the efficacy of aliskiren therapy in hypertension and the evidence for using aliskiren in combination with HCTZ.
Introduction
Elevated blood pressure (BP) is a major risk factor for the development of myocardial infarction, heart failure, stroke and renal failure. Greater than 25% of the global population was hypertensive in 2000 with a 60% projected increase in incidence by the year 2025 (CitationKearney et al 2005). Approximately 30% of the US population is hypertensive (CitationOng et al 2007). According to the 7th Joint National Committee on the prevention, detection, evaluation and treatment of high blood pressure (JNC-7), only about a third of treated US adult patients have their BP adequately controlled (CitationChobanian et al 2003). An epidemiology study of hypertension treatment and control in five European countries, Canada and the US showed lower treatment and control rates in Europe when compared to North America (CitationWolf-Maier et al 2004).
Hypertension is a treatable disease and effective medical therapies have been available for nearly 5 decades. Socio-economic conditions, treatment non-compliance and inadequate prevention strategies have all been implicated as barriers to adequate BP control. The major pharmacological strategies currently utilized for hypertension management include volume control with diuretics, suppression of central and peripheral sympathetic nervous system activity, vasodilation with ion channel manipulation and blockade of renin-angiotensin-aldosterone system (RAAS). Monotherapy results in adequate control of BP only in fewer that 50% of patients (CitationMaterson et al 1993; CitationCushman et al 2002; CitationChobanian et al 2003). Most patients require combination therapy using agents with complimentary mechanisms of action. Life style modification should also be an integral part of the treatment plan. Combination therapy may enable the utilization of sub-maximal doses of component drugs thus minimizing adverse events without significantly affecting potency. Several combination agents are currently available. The most widely used combinations involve a thiazide diuretic like hydrochlorothiazide (HCTZ) together with a drug blocking the RAAS such as angiotensin converting enzyme (ACE) inhibitor or angiotensin receptor blocker (ARB). RAAS has long been known to play a crucial role in both the regulation of BP as well as atherogenesis and vascular damage (CitationOparil and Haber 1974; CitationDzau 2001). Thiazide diuretics block the uptake of Na+ in the distal convoluted tubule of the nephron resulting in salt and water depletion. While this can lower the BP, the resulting activation of the RAAS may limit the antihypertensive benefits of diuretics. Thus drugs that inhibit the RAAS such as ACE inhibitors and ARBs are considered attractive for combination with thiazide diuretics (CitationSkolnik et al 2000; CitationWaeber B 2003). Recently, a direct renin inhibitor namely aliskiren was approved by the US Food and Drug Administration and the European regulatory agency for the treatment of hypertension. The antihypertensive efficacy of aliskiren has been studied both as monotherapy and in combination with other agents including HCTZ. The current review includes an overview of RAAS and the clinical experience of renin blockade with aliskiren in hypertension with particular focus on the evidence for using aliskiren/HCTZ combination. Articles published in English language pertaining to aliskiren were reviewed.
Renin-angiotensin-aldosterone system and its blockade
A schematic of the RAAS is depicted in . Renin is an aspartic protease generated and released from the juxtaglomerular cells in the kidney. The renin molecule has two homologous lobes and the cleft between the lobes contain the active site (CitationDanser and Deinum 2005). Under the influence of renin, angiotensinogen, the only know substrate of renin is cleaved to generate the decapeptide angiotensin I (Ang I). This is the rate-limiting step of RAAS activation. In the presence of angiotensin converting enzyme (ACE), Ang I is converted into the octapeptide hormone angiotensin II (Ang II), a powerful vasoconstrictor that mediates its activity through the type-1 angiotensin II (AT1) receptor. Binding of Ang II to AT1 receptor increases BP, and promotes aldosterone secretion from adrenal cortex, sodium reabsorption in renal proximal tubules, and catecholamine release from pre-synaptic nerve endings and adrenal medulla (CitationKim and Iwao 2000). Pathological activation of RAAS can result in hypertension with consequent end-organ damage.
Figure 1 Renin-angiotensin-aldosterone system and the sites of blockade. Thick arrows indicate main pathways, thin arrows denote alternative pathways and dashed arrows show sites of blockade.
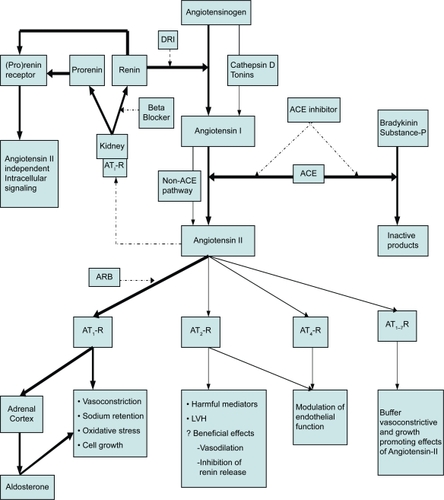
Several medications can interrupt the RAAS cascade but redundant pathways limit drug effects. Beta blockers inhibit renin secretion from the juxtaglomerular cells. ACE inhibitors block the conversion of Ang I to Ang II but non-ACE pathways of Ang II generation such as chymase and dipeptidases present in end organs including heart, kidney and blood vessels get activated under conditions of ACE inhibition (CitationHollenberg et al 1998; CitationUrata et al 1990). ACE inhibitors are not specific for RAAS and can prevent ACE-induced inactivation of bradykinin and substance P that are thought to be responsible for ACE-inhibitor related side effects such as cough and angioedema. ARBs exert their effect by blocking AT1 receptors activation by Ang II. This may lead to unopposed stimulation of other types of receptors such as type-2 and type-4 Ang II receptors (AT2 and AT4 receptors). Physiological role of these receptors are not clear but may be important for endothelial function (CitationWantanabe et al 2005). Over stimulation of AT2 receptors can generate deleterious agents such as oxygen free radicals, pro-inflammatory cytokines and pro-fibrotic mediators and may promote left ventricular hypertrophy (CitationWilliams 2001; CitationAzizi et al 2006). On the other hand, beneficial effects such as inhibition of renin synthesis and Ang II formation are also reported following AT2 receptor activation (CitationSiragy et al 2005). Both ACE inhibitors and ARBs stimulate renal renin production by disrupting the inhibitory feed back of Ang II on juxtaglomerular cells. The resulting increase in renin eventually restores Ang II level.
As mentioned before, the rate limiting step in RAAS is the conversion of angiotensinogen to Ang I under the influence of renin. There is a steep step down in concentration from angiotensinogen to Ang I which makes renin inhibition an attractive option for effective RAAS blockade. Animal studies using gene-dosing strategies showed increase in BP in the presence of increased copies of angiotensinogen gene but not with ACE gene, underscoring the rationale for blocking the conversion of angiotensinogen to Ang I (CitationSmithies 1997). Even though renin was discovered more than a century ago, a successful direct renin inhibitor has been available for clinical use only recently. Investigational renin inhibitors such as remikiren, enalkiren, ditekiren and zanikern developed in the past were limited by short half-life, high costs, and poor bioavailability (CitationFisher and Hollenberg 2001). Aliskiren is the first direct renin inhibitor with sufficient bioavailability (2.5%), safety and efficacy that was tested in human studies.
Pro-renin is an inactive precursor of renin that is constitutively released from the kidney. Pro-renin is rendered inactive by a 43-amino acid N-terminus that covers the enzymatic cleft. The circulating level of pro-renin is approximately 10-fold higher than renin levels and the proportion is increased in diabetics (CitationLuetscher et al 1985; CitationDanser et al 1998). Increased pro-renin levels may predict the onset of microalbuminuria in patients with diabetes (CitationChiarelli et al 2001). Pro-renin can undergo proteolytic and nonproteolytic activation. Proteolytic activation occurs predominantly in the juxtaglomerular cells. Nonproteolytic activation can be induced by exposure to low temperature and low pH as well as through binding to the recently discovered (pro)renin receptor (CitationNguyen et al 2002). (Pro)renin receptors have been localized to mesangial cells, distal collecting tubular cells of kidney, vascular smooth muscle cells, human heart and brain. These receptors bind both renin and pro-renin. Once bound to (pro)renin receptors, activated pro-renin and renin facilitate circulation independent Ang I production locally. The binding also promote intracellular signaling pathways in an angiotensin independent manner through mitogen-activated protein kinases leading to upregulation of pro-fibrotic mediators with harmful end-organ consequences that are inhibited by neither ACE inhibitors nor ARBs. (Pro)renin receptor blockade inhibited progression of nephropathy and reversed glomerulosclerosis in rats with streptozotozin- induced diabetes with proteinuria and glomerulosclerosis (CitationTakahashi et al 2007).
Aliskiren: pharmacokinetic and pharmacodynamic properties
Aliskiren is a small-molecular-weight, orally active, non-peptide direct renin inhibitor with very high affinity and specificity for human renin (CitationWood et al 2003). It blinds to the S1/S3 pocket at the active site of renin molecule thus preventing the conversion of angiotensinogen to Ang I. Aliskiren is a potent inhibitor of renin with an IC50 (concentration inhibiting 50% of activity) of 0.6 nmol/L. Renin is measured as plasma renin concentration (PRC) and plasma renin activity (PRA). PRC measures the actual amount of renin in plasma regardless of its enzymatic activity and is expressed as either μU/mL or pg/mL. PRA denotes the enzymatic activity of renin and is measured as the rate of angiotensin I production after adding serum to angiotensinogen. PRA is expressed as ng/ml/hour.
Effects of various medications on RAAS pathway are shown in . With the exception of beta blockers, all other agents blocking RAAS and diuretics including HCTZ increase PRC. Aliskiren and ACE inhibitors achieve this by decreasing Ang II levels and ARBs by blocking inhibitory effects of Ang II on AT 1 receptors on juxtaglomerular cells. Diuretics increase PRC by inducing volume depletion. The magnitude of PRC elevation is more pronounced when aliskiren is combined with HCTZ. PRA is increased by ACE inhibitors, ARBs and HCTZ while aliskiren use alone and in combination with HCTZ is associated with a decrease in PRA. Other agents that can decrease PRA include beta blockers and centralα-2 receptor agonists.
Table 1 Medication effects on RAAS pathway
Pharmacokinetic properties
Pharmacokinetic properties of aliskiren have been reported before (CitationAzizi et al 2006; CitationNovartis Pharmaceuticals Corporation 2007; CitationWaldmeier et al 2007). After an oral dose, the bioavailability of aliskiren is 2.5%. High aqueous solubility and affinity for renin compensates for the low absolute bioavailability of aliskiren. Peak plasma concentration is achieved within one to three hours following a single oral dose. Plasma concentration increased in a dose dependent manner at dose ranges of 40 to 640 mg/day. Steady state blood levels are reached in about 7 to 8 days. A terminal half-life of 23 to 36 hours makes the drug suitable for once daily administration (CitationAzizi et al 2006). A dose-dependent increase in trough plasma concentration of aliskiren from 2.6 to 30.0 ng/mL was seen with aliskiren doses ranging from 37.5 to 300 mg/day in one study (CitationStanton et al 2003). Mean trough plasma concentrations of aliskiren were 10.7 ± 6.7, 13.1 ± 8.3, 9.5 ± 5.9 and 7.6 ± 3.2 ng/mL respectively in hypertensive patients taking aliskiren 150 mg, aliskiren/HCTZ 150/25 mg, ramipril/aliskiren 5/150 mg and irbesartan aliskiren 150/150 mg daily in another study (CitationO’Brien et al 2006).
Aliskiren has a large volume of distribution and a plasma protein binding of 49.5%. Mean area under the curve (AUC) and Cmax of aliskiren decreased by 71% and 85% respectively when taken with a high fat meal (CitationNovartis Pharmaceuticals Corporation 2007). Patients should take aliskiren on an empty stomach and establish a routine pattern with regard to meals. A 32% to 70% inter-subject variability in AUC and Cmax was noted for a 40 to 1800 mg dose range of oral aliskiren (CitationNussberger et al 2002). AUC and Cmax were higher by 28% and 57% respectively in subjects over 65 years compared to those 18 to 45 years old (CitationVaidyanathan et al 2007). Following the administration of 300 mg aliskiren in healthy subjects, 90.9% drug elimination was via the fecal route and only 0.6% was recovered from urine (CitationWaldmeier et al 2007). Hepatic first-pass effect is minimal for aliskiren and modification of starting dose is not recommended in patients with hepatic and renal impairment. Pharmacokinetics of aliskiren are similar among Japanese, Blacks and Caucasians.
Aliskiren is not metabolized by cytochrome P450 system and has a low potential for drug interactions. The pharmaco-kinetics of amlodipine, valsartan, HCTZ and ramipril were not influenced by co-administration with aliskiren in healthy volunteers (CitationVaidyanathan et al 2006). Co-administration of lovastatin, atenolol, celecoxib and cimetidine did not significantly change AUC and therapeutic half-life of aliskiren (CitationDieterle et al 2005). Aliskiren did not exert detectable effects on the pharmacokinetics and pharmacodynamics of warfarin (CitationDieterle et al 2004). There were no clinically significant interactions between aliskiren and digoxin in health volunteers (CitationDieterich et al 2006). Co-administration of aliskiren with furosemide reduced the AUC and Cmax of furosemide by 30% and 50% respectively (CitationNovartis Pharmaceuticals Corporation 2007).
Pharmacodynamic properties
Since renin is very species specific, animal testing of human renin inhibitors are limited to marmosets and guinea pigs. Aliskiren doses of 1 and 3 mg/kg completely suppressed PRA for 6 and 12 hours respectively in sodium depleted marmosets (CitationWood et al 2005). BP lowering effects of aliskiren were similar to valsartan and benzapril. Aliskiren decreased PRA, Ang I and Ang II levels in normotensive volunteers in a dose dependent manner but caused a 10-fold increase in PRC (CitationNussberger et al 2002). A decrease in plasma and urine aldosterone levels were also noted with daily aliskiren doses of 80 mg and above. Aliskiren 160 mg and enalapril 20 mg doses were comparable in terms of their inhibitory effects on Ang II levels (CitationNussberger et al 2002).
A small randomized four-period cross-over study looked at the effects of single doses of aliskiren 300 mg, valsartan 160 mg and aliskiren/valsartan 150/80 mg combination in 12 mildly sodium-depleted volunteers (CitationAzizi et al 2004). Aliskiren lowered PRA, and plasma levels of Ang I and Ang II for 48 hours, stimulated active renin release more strongly than valsartan 160 mg and decreased urinary aldosterone excretion for longer duration than valsartan 160 mg. The effects of aliskiren/valsartan 150/80 mg were similar to aliskiren 300 mg but greater than those of valsartan 160 mg. Aliskiren blunted the valsartan-induced rise in PRA and plasma levels of Ang I and Ang II. Similar findings were also reported in sodium-replete normotensive individuals (CitationAzizi et al 2007).
Preclinical target organ protection studies of aliskiren
Since renin is highly species specific and aliskiren inhibits only primate renin, usual animal models of hypertension studies can not be used to test the end organ effects of aliskiren. Double transgenic rats (dTGR) which carries human genes for both renin and angiotensin were developed to circumvent this issue (CitationGanten et al 1992; Fukamizu et al 1993). These dTGR can generate large amounts of Ang II and untreated animals die by 8 weeks from cardiac dysfunction and renal failure. This feature makes dTGR an excellent model to test the effects of human renin inhibitors.
The target organ protection by aliskiren and valsartan were compared in dTGR (CitationPilz et al 2005). Matched dTGR received no treatment, aliskiren (0.3 or 3 mg/kg/day) or valsartan (1 or 10 mg/kg/day) from weeks 6 to 9. All groups had hypertension at week 6. Untreated dTGR developed worsening hypertension, increased creatinine and albuminuria by week 7 with 100% mortality by week 9. Both aliskiren treated groups and high-dose valsartan treated group had lower BP and albuminuria and normal serum creatinine levels by weeks 9 with 100% survival. Mortality was 26% in low-dose valsartan group and this group also had ventricular hypertrophy and diastolic dysfunction. In this model, renin inhibition had more favorable effect on end organ damage compared to angiotensin receptor blockade. In another study of dTGR model, both aliskiren and losartan reduced albuminuria and renal expression of inflammatory markers (CitationShagdarsuren et al 2005). Similar findings with reduction of albuminuria and reduced gene expression of TGF-beta and collagen III and IV were observed with aliskiren use in dTGR with diabetic nephropathy (CitationKelly et al 2007).
The role of renin inhibition and AT1-receptor blockade in attenuating cardiac oxidative stress and cellular remodeling was evaluated in the transgenic TG(mRen2)27 rat, a rodent model of chronically elevated tissue Ang II levels with consequent hypertension, insulin resistance and cardiovascular damage (CitationWhaley-Connell et al 2008). Administration of aliskiren and irbesartan were both associated with significant attenuation of cardiac functional and structural alterations in TG (mRen2)27 rats but irbesartan caused greater reductions in BP and markers of oxidative stress. In another study, aliskiren use lowered BP, prevented albuminuria and suppressed renal expressions of TGF-beta and collagen I in streptozotozin-diabetic TG (mRen2)27 rats (CitationFeldman et al 2008). Aliskiren also reduced renal expression of (pro)renin receptor.
Clinical efficacy of aliskiren in hypertension
Aliskiren has been evaluated as both monotherapy and in combination therapy in the treatment of hypertension. outlines the studies of aliskiren in hypertension.
Table 2 Studies of aliskiren therapy in hypertension
Aliskiren monotherapy in hypertension
Clinical trials have compared the antihypertensive efficacy of aliskiren with placebo, HCTZ, ARBs, ACE inhibitors and calcium channel blockers. The antihypertensive effect of aliskiren was evaluated in 455 Japanese patients with a mean sitting diastolic BP (msDBP) of 95 to 110 mmHg (CitationKushiro et al 2006). Patients were assigned to aliskiren 75 mg, 150 mg or 300 mg or placebo for 8 weeks in a double-blind randomized manner. Aliskiren produced a dose dependent-reduction in both msDBP (p < 0.0005 vs placebo for each dose) and mean sitting systolic BP (msSBP) (p < 0.001 vs placebo for each dose). Placebo corrected reductions in msSBP/msDBP were 5.7/4.0, 5.9/4.5 and 11.2/7.5 mmHg for aliskiren doses of 75, 150 and 300 mg respectively. At the study end, 27.8%, 47.8%, 48.2% and 63.7% of patients in the placebo and aliskiren 75, 150 and 300 mg groups, respectively had a successful response (defined as a DBP < 90 mmHg and/or <10 mmHg reduction from baseline, p < 0.005 vs placebo for each aliskiren dose). However it should be noted that only about 36% of patients showed adequate response to 300 mg aliskiren monotherapy when corrected for the placebo effect. Aliskiren demonstrated placebo-like tolerability. In another study, 672 patients with msDBP of 95 to 109 mmHg were randomized to aliskiren doses of 150 mg, 300 mg, 600 mg or placebo for 8 weeks (CitationOh et al 2007). Compared to a reduction in msSBP/msDBP of 3.8/4.9 mmHg with placebo, aliskiren doses of 150 mg, 300 mg and 600 mg resulted in 13.0/10.3, 14.7/11.1 and 15.8/12.5 mmHg reductions respectively (p < 0.0001). Aliskiren doses of 150 mg, 300 mg and 600 mg resulted in PRA reductions of 79.5%, 81.1% and 75.0% from baseline but PRC increased by 51.5%, 101.6% and 228.5% from the baseline. Patients taking 600 mg of aliskiren reported increased incidence of diarrhea.
In a multi-center double-blind trial, 652 patients with mild to moderate hypertension were randomized to once-daily doses of aliskiren (150 mg, 300 mg or 600 mg) irbesartan 150 mg or placebo for 8 weeks (CitationGradman et al 2005). Compared to placebo, all doses of aliskiren significantly lowered trough msSBP and msDBP (p < 0.001) (). The dose-response curve for aliskiren showed a plateau at 300 mg and antihypertensive efficacy was similar between aliskiren 150 mg and irbesartan 150 mg. BP control (defined as a BP < 140/90 mmHg) was achieved in 37.8%, 50% and 20.8% of patients on aliskiren 150 mg, 300 mg and placebo. Aliskiren was well tolerated.
Another double-blind trial randomized 226 patients with mild to moderate hypertension to four doses of aliskiren (37.5 mg, 75 mg, 150 mg, 300 mg) or losartan 100 mg daily for 4 weeks (CitationStanton et al 2003). The mean ± SD changes in daytime ambulatory systolic BP were −0.4 ± 11.7, −5.3 ± 11.3, −8.0 ± 11.0 and −11.0 ± 11.0 mmHg respectively in patients receiving 37.5 mg, 75 mg, 150 mg and 300 mg doses of aliskiren (p = 0.0002). The changes in PRA (median change as percentage with inter- quartile range) for the same doses of aliskiren were −55 (−64, −11), −60 (−82, −46), −77 (−86, −72) and −83 (−92, −71) respectively (p = 0.0008). Losartan 100 mg increased the PRA by 110%. The change in day time systolic pressure with 100 mg losartan (−10.9 ± 13.8 mmHg) was not significantly different from the changes seen with 75, 150 and 300 mg aliskiren. All doses of aliskiren were well tolerated.
A multicenter 8-week trial randomized 1123 patients with mild to moderate hypertension (msDBP ≥ 95 mmHg) to once daily doses of aliskiren (75 mg, 150 mg or 300 mg), valsartan (80 mg, 160 mg or 320 mg), aliskiren/valsartan combinations (75/80 mg 150/160 mg or 300/320 mg), valsartan/HCTZ (160/12.5 mg) or placebo (CitationPool et al 2007). Compared with placebo, there were significant reductions in both msSBP and msDBP with aliskiren 300 mg (10.0/8.6 vs 15.0/12.3 mmHg, p < 0.001). Valsartan 160 mg and 320 mg doses lowered msSBP and msDBP significantly compared to aliskiren 150 mg (p < 0.05 for both valsartan doses) (). Placebo effect was prominent. A pooled analysis involving 8481 patients involved in double-blind trials with aliskiren and placebo arms for a period of 8 to 12 weeks revealed reductions in msSBP/msDBP of 12.5/10.1 and 15.2/11.8 mmHg respectively from baseline with aliskiren 150 and 300 mg doses compared to 6.2/5.9 mmHg with placebo (p < 0.0001) (CitationDahlof et al 2007).
The efficacy, safety and tolerability of aliskiren were evaluated in patients ≥ 65 years of age (CitationVerdecchia et al 2007). In this study, 355 elderly patients with msSBP 145–179 mmHg and mean 24-hour ambulatory SBP of ≥ 135 mmHg underwent double-blind randomization to 8-week treatment with once daily aliskiren (75, 150 or 300 mg) or lisinopril 10 mg. At study end, mean 24-hour ambulatory SBP/DBP decreased by 8.4/4.5, 7.1/3.6, 8.7/3.9 and 10.2/6.3 mmHg respectively with aliskiren 75, 150 and 300 mg and lisinopril 10 mg doses. A higher proportion of patients on aliskiren 300 mg vs 75 mg achieved BP < 140/90 mmHg (36.2% vs 24.2%, p = 0.033). All doses of aliskiren were well tolerated. Another study randomized 842 patients (msDBP 95–109 mmHg) to aliskiren 150 mg or ramipril 5 mg with subsequent doubling of the drug doses and addition of HCTZ (12.5–25 mg) for inadequate BP control (CitationAndersen et al 2008). At 26-week follow-up, aliskiren-based therapy significantly lowered msSBP (17.9 vs 15.2 mmHg, p = 0.0036), msDBP (13.2 vs 12.0 mmHg, p = 0.025) and resulted in higher rates of BP control (61.4% vs 53.0%, p = 0.0205) compared to ramipril based therapy. During drug withdrawal, BP increased more rapidly after stopping ramipril than aliskiren based therapy, median BP reached 140/90 mmHg after 1 and 4 weeks of drug withdrawal respectively. The incidence of serum potassium levels > 5.5 mmol/L was 1.9% in the aliskiren group and 1% in the ramipril group.
A double-blind multi-center 8-week trial randomized 183 patients with severe hypertension (msDBP 105–119 mmHg) in a 2:1 ratio, to aliskiren 150 mg or lisinopril 20 mg with dose-doubling and subsequent addition of HCTZ for additional BP control (CitationStrasser et al 2007). Reductions in msSBP and msDBP as well as responder rates (81.55 vs 87.9%) were similar between aliskiren and lisinopril groups (). Half of patients in each group needed HCTZ for adequate BP control.
In summary, monotherapy with aliskiren was well tolerated with antihypertensive effects comparable to losartan, irbesartan, lisinopril and ramipril. Dose-response curve seems to plateau at 300 mg of aliskiren. Aliskiren consistently lowered PRA. Prominent placebo effects seen in most studies were attributed to factors such as regression to the mean, residual effects from previous therapy and limitations of cuff BP measurements.
Aliskiren combination therapy in hypertension
Antihypertensive efficacy, safety and tolerability of aliskiren in combination with HCTZ, ACE inhibitors, ARBs and calcium channel blockers were tested in patients with hypertension.
Combination with an ACE inhibitor, ARB or calcium channel blocker
Dual blockade of the RAAS can be achieved by utilizing combination of aliskiren with either an ACE inhibitor or an ARB. The additional antihypertensive effects of adding 6 weeks of aliskiren therapy (75 mg in the first 3 weeks and 150 mg in the last 3 weeks) in patients with mild to moderate hypertension on monotherapy with ramipril (n = 21) or irbesartan (n = 23) was assessed in an open-label design using ambulatory blood pressure monitoring (ABPM) (CitationO’Brien et al 2007). The addition of aliskiren to 5 mg of ramipril further lowered both day time and night time BP compared to ramipril monotherapy while the addition of aliskiren to 150 mg of irbesartan resulted in significant reduction in night time BP (). Ramipril and irbesartan monotherapy caused 90% and 175% increase in PRA respectively. By contrast, when aliskiren was co-administered with ramipril or irbesartan, PRA levels were similar to or less than baseline values. Treatment compliance assessed from pill counts averaged > 95%. The maximum individual serum potassium levels recorded when aliskiren was co-administered with ramipril or irbesartan were 5.3 and 5.5 mmol/L respectively.
A double-blind study randomized 1797 patients with hypertension (msDBP 95–109 mmHg and 8-hour daytime ambulatory diastolic BP ≥ 90 mmHg) to receive once-daily aliskiren 150 mg (n = 437), valsartan 160 mg (n = 455), a combination of aliskiren 150 mg and valsartan 160 mg (n = 446), or placebo (n = 459) for 4 weeks, followed by force titration to double the dose for another 4 weeks (CitationOparil et al 2007). Before the study end, 11% of patients discontinued treatment mainly due to lack of therapeutic effect. An intention-to-treat analysis at 8-week endpoint showed a significant reduction in msSBP/msDBP from baseline with the combination of aliskiren and valsartan when compared to aliskiren (p < 0.0001) or valsartan (p < 0.0001) monotherapy or placebo (p < 0.0001) (). ABPM in a subset of patients also showed similar observation. Both aliskiren and valsartan monotherapy significantly decreased msSBP/msDBP compared to placebo (p < 0.0001). Combination therapy provide additional reductions of 4.2/3.2 mmHg over aliskiren monotherapy and 4.4/2.5 mmHg over valsartan monotherapy. PRC was highest in the combination therapy group (912%) compared to patients who received aliskiren (468%) or valsartan (138%). While aliskiren 300 mg monotherapy and aliskiren/valsartan combination therapy decreased PRA (73% and 44% respectively), valsartan 320 mg monotherapy increased PRA by 160%. A serum potassium of > 5.5 mmol/L was observed more frequently during combination therapy (4%) than during aliskiren or valsartan monotherapy (2% each) or with placebo (3%).
The 6-month interim analysis of a long-term, open-label study looking at the safety, tolerability and efficacy of aliskiren/valsartan 300/320-mg combination in patients with hypertension (msDBP 90–109 mmHg) was reported recently (CitationChrysant et al 2008). A total of 601 patients received aliskiren/valsartan (150/160 mg) combination for 2 weeks followed by forced titration to aliskiren/valsartan 300/320 mg once daily for a targeted duration of 52 weeks. Optional HCTZ addition was allowed starting from week 8 if BP control was inadequate (>140/90 mmHg). At the 6-month point, 512 patients were still ongoing with the study and 192 patients received at least once dose of HCTZ-add on therapy. Reductions in msSBP/msDBP of 22.3/14.4 mmHg were observed at 6-month endpoint and 73.4% of patients achieved BP of < 140/90 mmHg. Ten patients (2.5%) receiving aliskiren/valsartan and 2 patients (1%) receiving aliskiren/valsartan/HCTZ developed serum potassium >5.5 mmol/L.
A double-blind multi-center trial, randomized 837 patients with diabetes mellitus and hypertension (msDBP 96–109 mmHg) to once daily aliskiren (150 mg, titrated to 300 mg after 4 weeks; n = 282), ramipril (5 mg titrated to 10 mg; n = 278) or the combination for 8 weeks (CitationUresin et al 2007). When compared to ramipril or aliskiren monotherapy, aliskiren/ramipril combination provided superior reductions in msDBP (p = 0.004 and 0.043 respectively) (). An additional reduction in mean BP of 4.6/2.1 mmHg was achieved by the addition of aliskiren to ramipril. PRC increased in all groups but there was a 66% reduction in PRA from baseline in the aliskiren group (p < 0.0001) and a 48% reduction in the combination group (p < 0.0001). The randomized trial by Pool et al discussed earlier noted similar reductions in msSBP/msDBP with aliskiren/valsartan 150/160 mg and 300/320 mg doses when compared to valsartan/HCTZ 160/12.5 mg dose.
In a double-blind study, 545 patients whose msDBP remained at 90–109 mmHg despite 4 weeks of therapy with amlodipine 5 mg daily were randomized to 3 arms for 6 weeks: continue amlodipine 5 mg, amlodipine 10 mg or amlodipine 5 mg with aliskiren 150 mg (CitationDrummond et al 2007). At study end, reduction in msSBP/msDBP with aliskiren/amlodipine 150/5 mg was significantly more compared to amlodipine 5 mg monotherapy (11.0/8.5 vs 5.0/4.8 mmHg, p < 0.001) but was similar to amlodipine 10 mg monotherapy (9.6/8.0 mmHg). Peripheral edema developed more frequently in the amlodipine 10 mg group (11.2%) compared to the combination therapy (2.1%) and amlodipine 5 mg (3.4%).
Combination with HCTZ
Antihypertensive efficacy of aliskiren has been studied both in comparison to and in combination with HCTZ. A 12-month randomized study compared the antihypertensive efficacy of once-daily doses of aliskiren 300 mg and HCTZ 25 mg in1124 patients with mild to moderate hypertension (CitationSchmieder et al 2007). Add on therapy with amlodipine 5 to 10 mg was used as needed to achieve a target BP of 140/90 mmHg. Starting at 12 weeks, aliskiren 300 mg significantly lowered BP from baseline compared to HCTZ ().
An 8-week multi-center double-blind trial randomized 2776 patients with msDBP of 95 to 109 mmHg to different doses of aliskiren (75 mg, 150 mg or 300 mg), HCTZ (6.25 mg, 12.5 mg or 25 mg), aliskiren/HCTZ combinations (75/6.25, 75/12.5, 75/25, 150/6.25, 150/12.5, 150/25, 300/12.5, 300/25 mg) or placebo (CitationVillamil et al 2007). Aliskiren monotherapy with all 3 doses significantly lowered msDBP compared to placebo with a linear dose relationship (p = 0.0002) (). HCTZ monotherapy with all 3 doses also significantly reduced msDBP compared to placebo but with a non-linear dose relationship (p < 0.01). All doses of HCTZ and aliskiren doses of 150 and 300 mg significantly lowered msSBP compared to placebo. All combinations were superior to placebo (p < 0.0001) and most were superior to both monotherapies (p < 0.05) in lowering msDBP (exceptions were aliskiren/HCTZ 150/6.25 mg vs either monotherapy and aliskiren/HCTZ 75/12.5 mg vs HCTZ monotherapy). Reductions in msDBP from baseline to endpoint with combination therapy ranged from 10.4 ± 0.59 to 14.3 ± 0.61 mmHg. All combinations were superior to component monotherapies in reducing msSBP from baseline (p < 0.05), with the exception of aliskiren/HCTZ 75/12.5 mg vs HCTZ monotherapy. Reductions in msSBP from baseline to end point with combination therapy ranged from 14.3 ± 0.93 to 21.2 ± 0.97 mmHg. Greatest reduction in BP was seen in patients on aliskiren/HCTZ 300/25 mg (msSBP/msDBP reduction of 21.5/14.3 mmHg). Responder rate (msDBP < 90 mmHg and/or ≥10 mmHg reduction from baseline) was 63.9% for aliskiren 300 mg (p = 0.0005), 60.6% for HCTZ 12.5 mg (p < 0.02), 59.0% for HCTZ 25 mg (p < 0.02) and 58.4% to 80.6% for all combination doses (all p < 0.05) compared to 45.8% for placebo. Responder rates for all combinations of aliskiren (75–300 mg) with HCTZ 25 mg and aliskiren/HCTZ 300/12.5 mg were superior to both monotherapies (p < 0.05), where as aliskiren/HCTZ 75/12.5 mg and 150/12.5 mg were superior to their respective aliskiren monotherapies (p < 0.05). There was a trend towards higher control rare (defined as msSBP/msDBP < 140/90 mmHg at study end) with combination therapy (37.4%–59.5%) when compared to either aliskiren (29.0%–46.7%) or HCTZ (32.5%–37.7%) monotherapies. Among the monotherapy groups, only aliskiren 300 mg significantly improved control rate compared to placebo (46.7 vs 28.1%, p = 0.0001). Control rate were superior with all aliskiren/HCTZ combinations (except 75/6.25 mg group) when compared to placebo (p < 0.02). The antihypertensive effects of aliskiren and HCTZ were comparable but it should be noted that the study was powered to compare the antihypertensive effects of the combination therapies with component monotherapies but not to compare the monotherapies with each other. PRA decreased by 54.2, 65.1 and 57.6% from baseline in patients taking aliskiren 75, 150 and 300 mg doses where as PRA increased by 3.5, 44.7 and 71.9% with HCTZ doses of 6.25, 12.5 and 25 mg. A net reduction in PRA of 46.1% to 63.5% was observed in patients on aliskiren/HCTZ combinations. Placebo increased PRA only by 0.7% from baseline. PRC increased to a greater degree with aliskiren (164, 192 and 348% with aliskiren 75, 150 and 300 mg doses) compared to HCTZ (10, 26 and 108% with HCTZ 6.25, 12.5 and 25 mg doses). The highest PRC increase was seen with aliskiren/HCTZ 300/25 mg combination (1211% from baseline). Hypokalemia (serum potassium <3.5 mmol/L) developed in 3.9% and 5.9% of patients on HCTZ 12.5 mg and 25 mg doses respectively. The frequency of hypokalemia dropped to 0.7% to 2.0% and 2.2% to 3.4% respectively with drug combinations containing 12.5 mg and 25 mg HCTZ.
A 12-month open label study randomized patients with msDBP of 90–109 mmHg to aliskiren 150 mg (n = 1178) or 300 mg (n = 773) once daily after washout and a 2–4 week drug-free period (CitationSica et al 2006). If BP remained ≥140/90 mmHg after month 2, doubling of aliskiren dose from 150 to 300 mg or addition of HCTZ (12.5–25 mg) to aliskiren 300 mg was permitted. A subgroup of patients remaining on aliskiren monotherapy at month 11 were randomized to continue aliskiren (n = 132) or placebo (n = 129) for 4 weeks as double-blind withdrawal phase. A total of 1625 (83%) completed the study. Reductions in msSBP/msDBP at the endpoint were 17.5/12.4 and 18.8/13.3 mmHg in aliskiren 150 and 300 mg groups respectively. Addition of HCTZ was required in 868 patients (45%) and BP reduction at the study end in this group (18.7/12.1 mmHg) was comparable to aliskiren monotherapy group (17.4/13.3 mmHg). During the withdrawal period, mean sitting BP gradually increased in the placebo group where as BP reduction was maintained in patients remaining on aliskiren with a statistically significant difference between the groups at the end of withdrawal period (5.99/3.87 mmHg p = 0.0001). This difference was also seen in a subgroup of patients who underwent ABPM (4.14/3.87 mmHg p < 0.0001).
The additional antihypertensive benefit of aliskiren was analyzed in obese hypertensive (msDBP 95–109 mmHg) patients unresponsive to 25 mg of HCTZ (CitationJordan et al 2007). After a 2- to 4-week washout period, 560 patients received single-blind HCTZ 25 mg for 4 weeks; 490 non-responders underwent double-blind randomization to aliskiren 150 mg, irbesartan 150 mg, amlodipine 5 mg or placebo for 4 weeks while continuing HCTZ. This was followed by doubling the initial doses of aliskiren, irbesartan and amlodipine for 8 weeks. After 8 weeks of double-blind treatment (4 weeks on higher doses), BP reduction was significantly more with aliskiren/HCTZ compared to placebo/HCTZ (15.8/11.9 vs 8.6/7.9 mmHg, p < 0.0001) and the significance persisted at study end (p < 0.005 for msDBP and p < 0.0001 for msSBP). BP reductions with irbesartan/HCTZ (15.4/11.3 mmHg) and amlodipine/HCTZ (13.6/10.3 mmHg) were similar to aliskiren/HCTZ (). The BP control rate (a BP < 140/90 mmHg) was significantly higher with aliskiren/HCTZ compared to placebo/HCTZ at week 8 end point (p = 0.0005) and at week 12 end point (58.4% vs 33.3%, p = 0.0001). The BP control rate among amlodipine/HCTZ and irbesartan/HCTZ were not significantly different from those observed with aliskiren/HCTZ at week 8 and 12 end points but the BP control rate with aliskiren/HCTZ at week 8 end point was numerically higher compared to that observed with amlodipine/HCTZ (56.6 vs 45.1%, p = 0.052). Compared with pretreatment baseline, PRA increased with HCTZ monotherapy (p < 0.05) but when combined with aliskiren, there was a significant reduction in PRA (p < 0.05). Combination of HCTZ with irbesartan and amlodipine resulted in further significant increase in PRA. The open-label study by O’Brien et al also looked at the benefits of adding 25 mg of HCTZ (n = 23) to 150 mg of aliskiren daily for 3 weeks (CitationO’Brien et al 2007). Compared to aliskiren monotherapy, there was significant reduction in day time BP with combination therapy ().
Potential advantages of aliskiren/HCTZ combination in hypertension
Aliskiren monotherapy in large part demonstrated antihypertensive efficacy comparable to equivalent doses of HCTZ, losartan, irbesartan, lisinopril and ramipril. Fore effective BP control, majority of patients will require combination therapy. Both ACE inhibitors and ARBs are used extensively in combination with HCTZ. Aliskiren/HCTZ combination has several advantages. HCTZ has been clinically available for decades and costs less. It is considered the preferred first line antihypertensive agent in all comers (CitationChobanian et al 2003). While exerting its antihypertensive effects, HCTZ activates RAAS which can limit its efficacy. Agents blocking the RAAS such as aliskiren, ACE inhibitors and ARBs can augment the potency of HCTZ in addition to their own antihypertensive effects. At higher doses of aliskiren/HCTZ combination, reduction in BP was closer to the sum of BP reductions obtained with each monotherapy after excluding the placebo effects from all treatment groups. For instance, the placebo-corrected reduction in msSBP/msDBP were 8.2/3.4, 6.9/2.5 and 13.7/7.4 mmHg respectively with aliskiren 300 mg, HCTZ 25 mg and aliskiren/HCTZ 300/25 mg respectively in a large study (CitationVillamil et al 2007). On the other hand, placebo-corrected reductions in msSBP/msDBP with aliskiren 300 mg, valsartan 320 mg and aliskiren/valsartan 300/320 mg were 5.0/3.7, 6.5/2.7 and 8.0/4.3 mmHg respectively in one study (CitationPool et al 2007) and 8.4/4.9, 8.2/5.2 and 12.6/8.1 mmHg respectively in another study (CitationOparil et al 2007).
In addition to its antihypertensive effects, HCTZ is also a week diuretic which helps to correct any underlying hypervolemia/sodium excess. Ability of aliskiren to lower angiotensin1–7 (Ang1–7) levels may have a potential negative impact on BP lowering effects of aliskiren/ACE inhibitor and aliskiren/ARB combinations. Ang1–7 is a heptapeptide fragment of Ang II that can buffer the vasoconstrictive and growth promoting effects of Ang II. Ang1–7 can block AT1 receptor and stimulate release of nitric oxide and vasodilating prostaglandins (CitationDellipizzi et al 1994; CitationMahon et al 1994; CitationFreeman et al 1996; CitationLi et al 1997). Both ACE inhibitors and ARBs increase the level of Ang1–7, the former by inhibiting the ACE-induced degradation of Ang1–7 and the latter by increasing Ang II level (substrate for Ang1–7) through AT1 receptor blockade. Elevated levels of Ang1–7 are thought to be contributing to the antihypertensive effects of both ACE inhibitors and ARBs (CitationLuque et al 1996; CitationIyer et al 1998). Since direct renin inhibition can decrease Ang1–7 levels, it is intuitive to think that aliskiren might hamper antihypertensive effects of both ACE inhibitors and ARBs to some extent.
HCTZ monotherapy can cause hypokalemia and combination with aliskiren can mitigate this effect due to the potassium retaining effects of the latter. Dual inhibition of the RAAS can increase the risk of hyperkalemia. Fortunately hyperkalemia was not a frequent occurrence in studies of aliskiren combination therapy with ACE inhibitors and ARBs. The risk will be clearly increased in patients with underlying renal dysfunction.
Safety and tolerability
Aliskiren was well tolerated with adverse events and discontinuation rates similar to placebo in most clinical trials. An increased incidence of diarrhea was reported with 600 mg dose of aliskiren. The adverse effects of aliskiren monotherapy were similar to placebo (39.8% vs 40.2%) in a pooled analysis of over 2000 patients (CitationWeir et al 2007). Most common adverse effects reported with aliskiren vs placebo were head ache (5.75 vs 8.7%), nasopharyngitis (4.4% vs 5.8%) and diarrhea (2.6% vs 1.2%). Diarrhea was not associated with increased discontinuation rates. Serious adverse effects with aliskiren were low at 0.5% compared to 0.6% with placebo. Over 95% of the adverse effects were mild to moderate in severity thought to be unrelated to aliskiren.
Unlike ACE inhibitors, aliskiren does not affect the metabolism of bradykinin and substance P. Hence cough and angioedema are extremely rare with its use. Hyperkalemia is a concern when aliskiren is used in combination with ACE inhibitors or ARBs especially in patients with impaired renal function. Hypokalemia developed in 3.9 and 5.9% of patients who took 12.5 and 25 mg HCTZ monotherapy which decreased to 0.7%–2.0% and 2.2%–3.4% respectively after the addition of aliskiren (CitationVillamil et al 2007). Increased adverse effects may develop if aliskiren is used in volume depleted patients and those with severe renal artery stenosis. Aliskiren is contraindicated in pregnancy.
Perspectives on direct renin inhibition with aliskiren
RAAS plays a crucial role in chronic hypertension and end-organ damage. There is evidence that both ACE inhibitors and ARBs lower BP and confer end-organ protection in heart, kidney and blood vessels. Their efficacy is limited by redundant pathways in RAAS and counter regulatory mechanisms. Renin has been a therapeutic target for long time but a direct renin inhibitor has been available for clinical use only recently. Aliskiren may provide more complete and more effective blockade of RAAS. Cathepsin D and tonin pathways of Ang I generation are not blocked by renin inhibitors. But these pathways are not thought to be of significant physiological importance (CitationPhilips et al 1993). Compared to ACE inhibitors and ARBs, aliskiren induced more pronounced renal vasodilation in healthy normotensive human subjects (CitationFisher et al 2008). Studies thus far have shown similar antihypertensive effects at best with aliskiren when compared to equivalent doses of ACE- inhibitors, ARBs and diuretics. Aliskiren in combination therapies lowered BP more effectively than monotherapy and aliskiren/HCTZ combination appear to have more synergy. There is evidence from animal studies that aliskiren can confer end-organ protection in kidney and heart (CitationPilz et al 2005; CitationShagdarsuren et al 2005). Animal studies have also shown evidence for atherosclerotic plaque stabilization with aliskiren (CitationNussberger et al 2008). End organ protective effects of aliskiren in human studies are beginning to emerge. The recently published AVOID (Aliskiren in eValuation of prOteinuria in Diabetes) study has shown reduction in proteinuria independent of BP control in patients with diabetic nephropathy on background therapy with losartan 100 mg/day (CitationParving et al 2008).
The recently discovered (pro)renin receptor can bind and activate both pro-renin and renin with consequent intracellular signaling of second messenger pathways through an Ang II independent mechanism. (Pro)renin receptor blockade has shown to confer end organ protection in animal studies (CitationTakahashi et al 2007). Even though aliskiren could possibly modify pro-renin molecule and prevents its conversion to active renin, preliminary evidence indicate that aliskiren does not inhibit the renin-induced or pro-renin induced activation of the (pro)renin receptor (CitationSchmieder 2007; CitationSchefe et al 2008).
The reactive increase in PRC seen with aliskiren is more pronounced compared to other antihypertensive agents and is dose dependent. PRC increased even further with aliskiren/HCTZ combination. It was suggested that the elevated PRC might be sufficient to overwhelm the renin inhibitory capacity of aliskiren and may even cause paradoxical elevation of BP in patients with hyperreactive RAAS such as those with renovascular and malignant hypertension (CitationSealey and Laragh 2007). Others have discounted this theory pointing to the properties of aliskiren including long half-life and lack of rebound hypertension after withdrawal (CitationMenard and Azizi 2007). Another concern is the possibility that elevated PRC might cause harmful effects through the (pro)renin receptor. Available evidence indicate that aliskiren does not inhibit Ang II-independent intracellular signaling mediated through (pro)renin receptor but needs further clarification (CitationSarris et al 2006). Unlike other agents such as ACE inhibitors, ARBs and diuretics, aliskiren consistently decreased PRA as monotherapy and in combination therapy. Pretreatment PRA has shown a direct association with cardiovascular risk in hypertensive patients (CitationAldeman et al 1997). However, no study has yet reported such an association with drug induced elevations in PRA.
Conclusions
Aliskiren is the first direct renin inhibitor available for clinical use. The long half-life and absence of rebound phenomenon makes aliskiren suitable for once daily administration. Favorable side-effect profiles and high trough-to peak ratios are other features of aliskiren. The antihypertensive efficacy of monotherapy with aliskiren is dose-dependent up to 300 mg daily doses and is comparable to ACE inhibitors such as lisinopril and ramipril, ARBs such as losartan and irbesartan as well as HCTZ. Combination therapy with ACE inhibitors, ARBs, amlodipine and HCTZ were also well tolerated. Because of the complimentary pharmacological action of aliskiren and HCTZ, their combination seems favorable in hypertension. Aliskiren 150 to 300 mg with HCTZ 12.5 to 25 mg are the most effective of these single daily combinations. Since reactive increase in PRC could be a potential limiting factor with aliskiren in terms of its antihypertensive efficacy and beta blockers can blunt this response, combining aliskiren with a beta blocker looks attractive. Such a study using aliskiren-atenolol combination was completed recently and results are awaited. One has to be cautious about the risk of hyperkalemia with strategies utilizing dual blockade of RAAS. Studies are underway looking at the long-term efficacy, safety and tolerability of combination therapy of aliskiren with HCTZ or with agents blocking RAAS. In addition, outcome studies looking at the beneficial effects of aliskiren on left ventricular mass in obese hypertensive patients as well as its effect on post-myocardial infarction LV remodeling are ongoing.
Disclosures
The author has no conflicts of interest to disclose.
References
- AldemanMHOoiWICohenH1997Plasma renin activity: a risk factor for myocardial infarction in hypertensive patientsAm J hypertens101189008242
- AndersenKWeinbergerMHEganB2008Comparative efficacy and safety of aliskiren, an oral direct renin inhibitor, and ramipril in hypertension: a 6-month, randomized, double-blind trialJ Hypertens265899918300872
- AziziMMenradJBisseryA2004Pharmacologic demonstration of the synergistic effects of a combination of the renin inhibitor aliskiren and the AT1-receptor antagonist valsartan on the angiotensin II-renin feedback interruptionJ Am Soc Nephrol1531263315579516
- AziziMWebbRNussbergerJ2006Renin inhibition with aliskiren: where are we now and where are we going?J Hypertens242435616508564
- AziziMMenradJBisseryA2007Hormonal and hemodynamic effects of aliskiren and valsartan and their combination in sodium-replete normotensive individualsClin J Am Soc Nephrol29475517702736
- ChiarelliFPomilioMDe LucaFA2001Plasma prorenin levels may predict persistent microalbuminuria in children with diabetesPediatr Nephrol161162011261677
- ChobanianAVBakrisGLBlackHR2003Seventh report of the Joint National Committee on Prevention, Detection, Evaluation and Treatment of High Blood PressureHypertension4212065214656957
- ChrysantSGMurrayAVHoppeUC2008Long-term safety, tolerability and efficacy of aliskiren in combination with valsartan in patients with hypertension: a 6-month interim analysisCurr Med Res Opin2410394718307835
- CushmanWCFordCECutlerJA2002Success and predictors of blood pressure control in diverse North American settings: The Antihypertensive and Lipid Lowering Treatment to Prevent Heart Attack Trial (ALLHAT)J Clin Hyertens4393404
- DahlofBAndersonDRAroraV2007Aliskiren, a direct renin inhibitor, provides antihypertensive efficacy and excellent tolerability independent of age or gender in patients with hypertensionJ Clin Hypertens9Suppl AA157
- DanserAHDerkxFHSchalekampMA1998Determinant so finterindividual variation of renin and pro-renin concentrations: evidence for a sexual dimorphism of (pro)renin levels in humansJ Hypertens16853629663926
- DanserAHJDeinumJ2005Renin, pro-renin and the putative (pro)renin receptorHypertension4610697616186442
- DellipizziAMHilcheySDBell-QuilleyCP1994Natriuretic action of angiotensin (1–7)Br J Pharmacol111138012686
- DieterleWCorynenSMannJ2004Effect of the oral renin inhibitor aliskiren on the pharmacokinetics and pharmacodynamics of a single dose of warfarin in health subjectsBr J Clin Pharmacol58433615373937
- DieterichHKempCVaidyanathanS2006Aliskiren, the first in a new class of orally effective renin inhibitors, has no clinically significant interactions with digoxin in healthy volunteersClin Pharmacol Ther7911124
- DieterleWCorynenSVaidyanathanS2005Pharmacokinetic interactions of the oral renin inhibitor aliskiren with lovastatin, atenolol, celecoxib and cimetidineInt J Clin Pharmacol Ther435273516300168
- DrummondWMungerMAEssopMR2007Antihypertensive efficacy of the oral direct renin inhibitor aliskiren as add-on therapy in patients not responding to amlodipine monotherapyJ Clin Hypertens974250
- DzauVJ2001Tissue angiotensin and pathophysiology of vascuklar disease, a unifying hypothesisHypertension3710475211304501
- FeldmanDLJinLXuanH2008Effect of aliskiren on blood pressure, albuminuria, and(pro)renin receptor expression in diabetic TG(mRen-2) ratsHypertension52130618490518
- FisherNDHollenbergNK2001Is there a future for renin inhibitors?Exp Opin Invest Drugs1041726
- FisherNDJan DanserAHNussbergerJ2008Renal and hormonal responses to direct renin inhibition with aliskiren in healthy humansCirculation117319920518559696
- FreemanEJChisolmGMFerrarioCM1996Angiotensin (1–7) inhibits vascular smooth muscle growthHypertension2810488675248
- GantenDWagnerJZehK1992Species specificity of renin kinetics in transgenic rats harboring the human renin and angiotensin genesProc Natl Acad Sci U S A897806101502199
- GradmanAHSchmiederRELinsRL2005Aliksiren, a novel orally effective renin inhibitir, provides dose-dependent antihypertensive efficacy and placebo-like tolerability in hypertensive patientsCirculation1111028
- HollenbergNKFisherNDPriceDA1998Pathways of angiotensin II generation in intact human tissue: Evidence from comparative pharmacological interruption of the renin systemHypertension32387929740600
- IyerSNChappellMCAverillDB1998Vasodepressor actions of angiotensin (1–7) unmasked during combine treatment with lisinopril and losartanHypertension316997059461243
- JordanJEngeliSBoyeSW2007Direct renin inhibition with aliskiren in obese patients with arterial hypertensionHypertension4910475517353513
- KearneyPMWheltonMReynoldsK2005Global burden of hypertension: analysis of worldwide dataLancet3652172315652604
- KellyDJZhangYMoeG2007Aliskiren, a novel renin inhibitor, is renoprotective in a model of advanced diabetic nephropathy in ratsDiabetologia50239840417828524
- KimSIwaoH2000Molecular and cellular mechanisms of angiotensin II-mediated cardiovascular and renal diseasesPharmacol Rev52113410699153
- KushiroTItakuraHAboY2006Aliskiren, a novel oral renin inhibitor, provides dose-dependent efficacy and placebo-like tolerability in Japanese patients with hypertensionHypertens Res29997100517378372
- LiPChappellMCFerrarioCM1997Angiotensin (1–7) augments bradykinin-induced vasodilation by competing with ACE and releasing nitric oxideHypertension293944009039133
- LuetscherJAKraemerFBWilsonDM1985Increased plasma inactive renin in diabetes mellitus a marker of microvascular complicationsN Engl J Med3121412173887168
- LuqueMMartinPMartellN1996Effects of captopril related to increased levels of prostacyclin and angiotensin-(1–7) in essential hypertensionJ Hypertens147998058793704
- MahonJMCarrRDNicolAK1994Angiotensin (1–7) is an antagonist at the type 1 angiotensin II receptorJ Hypertens121377817706697
- MatersonBJRedaDJCushmanWC1993Single drug therapy for hypertension in men. A comparison of six antihypertensive agents with placebo. The department of Veterans Affairs Cooperative Study Group on Antihypertensive agentsN Engl J Med328914218446138
- MenardJAzizM2007The difficult conception, birth and delivery of renin inhibitor: controversies around aliskirenJ Hypertens2517758217762637
- Novartis Pharmaceuticals Corporation2007Tecturna® (aliskiren tablets): US prescribing informationEast Hanover, NJ
- NguyenGDelarueFBurckleC2002Pivotal role of the renin/pro-renin receptor in angiotensin II production and cellular responses to reninJ Clin Invest10914172712045255
- NussbegerJWuerznerGJensenC2002Angiotensin II suppression in humans by the orally active renin inhibitor aliskiren (SPP100); Comparison with enalaprilHypertension39E1811799102
- NussbergerJAubertJFBouzoureneK2008Renin inhibition by aliskiren prevents atherosclerosis progression: comparison with irbesartan, atenolol, and amlodipineHypertension5113061118391092
- O’BrienEBartonJNussbergerJ2007Aliskiren reduced blood pressure and suppress plasma renin activity in combination with a thiazide diuretic, an angiotensin converting enzyme inhibitor, or an angiotensin receptor blockerHypertension492768417159081
- OhBHMitchellJHerronJR2007Aliskiren, an oral renin inhibitor, provides dose-dependent efficacy and sustained 24-hour blood pressure control in patients with hypertensionJ Am Coll Cardiol4911576317367658
- OngKLCheungBMManYB2007Prevalence, awareness, treatment and control of hypertension among United States adults 1999–2004Hypertension49697517159087
- OparilSHaberE1974The renin angiotensin systemN Engl J Med2913814014211170
- OparilSYarowsSAPatelS2007Efficacy and safety of combined use of aliskiren and valsartan in patients with hypertension: a randomized, double-blind trialLancet370221917658393
- ParvingHHPerssonFLewisJB2008Aliskiren combined with losartan in type 2 diabetes and nephropathyN Engl J Med35824334618525041
- PhilipsMISpeakmanEAKimuraB1993Levels of angiotensin and molecular biology of the tissue angiotensin systemsRegul Pept431208426906
- PilzBShagdarsurenEWellnerM2005Aliskiren, a human renin inhibitor, ameliorates cardiac and renal damage in double-transgenic ratsHypertension465697616103264
- PoolJLSchmiederREAziziM2007Aliskiren, an orally effective renin inhibitor, provides antihypertensive efficacy alone and in combination with valsartanAm J Hypertens20112017198906
- SarrisJJ‘t HoenPACGarreldsIM2006Pro-renin induces intracellular signaling in cardiomyocytes independently of angiotensin IIHypertension485647116940215
- ShagdarsurenEWellnerMBraesenJH2005Compliment activation in angiotensin II induced organdamgeCirc Res977162416109917
- SchefeJHNeumannCGoebelM2008Prorenin engages the (pro)renin receptor like renin and both ligand activities are unopposed by aliskirenJ Hypertens2617879418698213
- SchmiederRE2007The potential role of pro-renin in diabetic nephropathyJ Hypertens251323617563548
- SchmiederREPhilippTGuerediagaJ2007Aliskiren-based therapy lowers blood pressure more effectively than hydrochlorothiazide-based therapy in patients with hypertensionJ Clin Hypertens9Suppl AA182
- SealeyJELaraghJH2007Aliskiren, the first renin inhibitor for treating hypertension: reactive renin secretion may limit its effectivenessAm J Hypertens205879717485026
- SicaDGradmanALederballeO2006Aliskiren, a novel renin inhibitor, is well tolerated and has sustained BP-lowering effects alone or in combination with HCTZ during long-term (52 weeks) treatment of hypertensionEur Heart J27SupplA797
- SiragyHMXueCAbadirP2005Angiotensin subtype-2 receptors inhibit renin biosynthesis and angiotensin II formationHypertension45133715534073
- SkolnikNSBeckJDClarkM2000Combination antihypertensive drugs: recommendations for useAm Fam Physician6130495610839554
- SmithiesO1997Theodore Cooper Memorial Lecture. A mouse view of hypertensionHypertension301318249403547
- StantonAJensenCNussbergerJO’BrienE2003Blood pressure lowering in essential hypertension with an oral renin inhibitor, aliskirenHypertension4211374314597641
- StrasserRHPuigJGFarsangC2007A comparison of the tolerability of the direct renin inhibitor aliskiren and lisinopril in patients with severe hypertensionJ Hum Hypertens21780717541390
- TakahashiHIchiharaAKaneshiroY2007Regression of nephropathy developed in diabetes by (pro)renin receptor blockadeJ Am Soc Nephrol1819899217596635
- UrataHKinoshitaAMisonoKS1990Identification of a highly specific chymase as the major angiotensin II forming enzyme in the human heartJ Biol Chem26522348572266130
- UresinYTaylorAAKiloC2007Efficacy and safety of the direct renin inhibitor aliskiren and ramipril alone or in combination in patients with diabetes and hypertensionJ Renin Angiotensin Aldosterone Syst8190818205098
- VaidyanathanSVelenciaJKempC2006Lack of pharmacokinetic interactions of aliskiren, a novel direct renin inhibitor for the treatment of hypertension, with the antihypertensives amlodipine, valsartan, hydrochlorothiazide (HCTZ) and ramipril in healthy volunteersInt J Clin Pract6013435617073832
- VaidyanathanSReynoldsCYehCM2007Pharmacokinetics, safety and tolerability of the novel oral direct renin inhibitor aliskiren in elderly healthy subjectsJ Clin Pharmacol474536017389554
- VerdecchiaPCalvoCMockelV2007Safety and efficacy of the oral direct renin inhibitor aliskiren in elderly patients with hypertensionBlood Press163819118058456
- VillamilAChrysantSGCalhounD2007Renin inhibition with aliskiren provides additive antihypertensive efficacy when used in combination with hydrochlorothiazideJ Hypertens252172617143194
- WaeberB2003Combination therapy with ACE inhibitors/angiotensin II receptor antagonists and diuretic in hypertensionExpert Rev Cardiovascular Ther14350
- WaldmeierFJGlaenzelUWirzB2007Absorption, distribution, metabolism and elimination of the direct renin inhibitor aliskiren in healthy volunteersDrug Metab Dispos3514182817510248
- WantanabeTBarkerTABerkBC2005Angiotensin II and the endothelium: diverse signals and effectsHypertension45163915630047
- WeirMRBushCAndersonDR2007Antihypertensive efficacy, safety, and tolrability of the oral direct renin inhibitor aliskiren in patients with hypertension: a pooled analysisJ Am Soc Hypertens126477
- WilliamsB2001Angiotensin II and the pathophysiology of cardiovascular remodelingAm J Cardiol8710C17C
- Whaley-ConnellAHabibiJCooperSA2008Effect of renin inhibition and AT1R blockade on myocardial remodeling in the transgenic Ren2 ratAm J Physiol Endocrinol Metab(Epub ahead of print)
- Wolf-MaierKCooperRSKramerH2004Hypertension treatment and control in five European countries, Canada and the United StatesHypertension4310714638619
- WoodJMMailbaumJRahuelJ2003Structure based design of aliskiren, a novel orally effective renin inhibitorBiochem Biophys Res Commun30869870512927775