Abstract
Background and aims:
Metalloproteinases (MMPs) are considered to be key enzymes in the pathogenesis of abdominal aortic aneurysms (AAA), with elevated levels in diseased aorta and in patient sera. Statins seem to exert an inhibitory effect on MMP activity in the aortic wall. No data exist on the effect of statins on serum activity of MMPs and inflammatory cytokines (interleukins, IL).
Methods:
The serum activities of MMP2 and MMP9, osteoprotegerin (OPG), and IL6 and IL10 in 63 patients undergoing elective infrarenal aneurysm repair were measured on the day before surgery. Levels were correlated to statin therapy and aneurysm diameter.
Results:
There was no significant difference between the two groups in the activity of circulating levels of MMP2/9, OPG, and IL6/10 in patients with infrarenal aortic aneurysm. IL6 levels in patients with AAA larger than 6 cm were significantly elevated; differences in serum activities of MMP2/9, OPG, and IL10 were not related to AAA diameter.
Conclusion:
Serum activities of MMP2/9, OPG, and IL6/10 are not correlated to statin therapy; IL6 levels are higher in patients with large aneurysms. Hence the effect of statin therapy in the treatment of aneurismal disease remains to be elucidated.
Introduction
Metalloproteinases (MMPs) are believed to play a key role in the development of aneurismal disease of the aorta, although the precise mechanisms leading to aneurysm formation remain unclear. Elevated levels of MMP2 and MMP9 have been shown in the extract tissue from surgical specimens and in the sera of patients with aortic aneurysm, compared with nondiseased aorta and healthy controls, respectively (CitationTamarina at al 1997; CitationHovsepian et al 2000; CitationLindholt et al 2000; CitationAnnabi et al 2002).
A common feature of vascular disease and aneurysm formation is an inflammatory process in the aneurismal wall with invasion of monocytes and macrophages and increased levels of interleukins (IL) such as IL6 (CitationDawson et al 2007). Hence one therapeutic approach in the conservative management of patients with aortic aneurysm aims to inhibit this inflammation and matrix turnover by statins and angiotensin II inhibitors (Abisi et al 2007; CitationEvans et al 2007). Simvastatin has been shown to suppress experimental aneurysm formation in rats (CitationKalyanasundaram et al 2006). Currently, the cessation of smoking, and antiplatelet and statin therapy are recommended in conservative treatment of patients with small aortic aneurysms (CitationDiehm et al 2007; Golledge et al 2007). Statin treatment has been shown to reduce circulating levels of MMPs in patients with acute coronary syndrome (CitationTziakas et al 2004). However, no data are available on the effect of statins on circulating levels of representative MMPs and cytokines in patients with abdominal aortic aneurysm (AAA). Hence we studied the serum activity of MMP2/9, osteoprotegerin (OPG) – a recently identified promoter of vascular disease that has been correlated to aneurysm expansion (CitationMoran et al 2005) – and IL6 and IL10 in patients undergoing elective infrarenal aortic aneurysm repair and correlated the measurements to statin therapy and aneurysm diameter.
Methods
The study was approved by the local ethics committee and informed consent was obtained from all patients preoperatively. Sixty-three patients undergoing elective infarenal aneurysm repair were recruited for this study; 25 patients were on regular statin therapy before surgery. Statin therapy lasted for at least 4 weeks before surgery; 23 patients were on simvastatin at a dose of 10–40 mg once daily, and 2 patients were on fluvastatin 80 mg once daily. All subjects had their surgical procedure at the Department of Thoracic and Vascular Surgery, University of Ulm, between 2005 and 2007. Blood samples were taken 1 day before surgery, immediately centrifuged for 10 min at 4000 rpm, and stored at –80 °C until measurements.
Matrix metalloproteinase activity bioimmunoassay
Active forms of MMP2 and MMP9 were measured using specific quantitative activity bioimmunoassays (Chemicon) according to the manufacturer′s instructions. MMP2 and MMP9 activity was expressed in nanograms per milliliter.
Osteoprotegerin
OPG activity was measured using a commercially available Enzyme Linked Immuno Sorbent Assay (BioCat) according to the manufacturer′s instructions. OPG activity was expressed in picograms per milliliter.
Interleukin 6 and 10
Levels of IL6 and IL10 were determined using a Enzyme Linked Immuno Sorbent Assay (R&D Systems). The manufacturer’s instructions were followed throughout.
Statistical analysis
For discrete variables, absolute and relative frequencies are given. For continuous frequencies, median values and range are applied as they were not normally distributed. To calculate the significance of difference in activity between the treatment groups the Mann Whitney U test was used. To calculate the significance of the relationship between AAA diameter and serum activity the Kruskal-Wallis one way analysis of variance on ranks was applied. P values <0.05 were regarded as significant. Statistical analysis was performed in collaboration with the Department of Biometry using the computer program SigmaStat.
Results
Patient data
The two patient groups were comparable for age, aneurysm diameter, sex, and pre-existing risk factors ().
Table 1 Demographic data of 63 patients undergoing elective aneurysm repair according to statin use
Biomarker activity as a function of statin therapy
There was no statistically significant difference in the serum activity of MMP2/9, OPG, and IL6/10 in patients with or without statin therapy: median values for MMP2 activity were 209 vs 211 ng/mL respectively, and for MMP9 activity 38 vs 37 ng/mL, respectively. OPG values were 417 vs 430 pg/mL, respectively. IL6 and IL10 levels also did not differ significantly: 5 vs 7 pg/mL and 6 vs 5 pg/mL, respectively (–).
Figure 1 Serum activity of MMP9 according to statin use; median values were 38 and 37 ng/mL, respectively (p = 0.868).
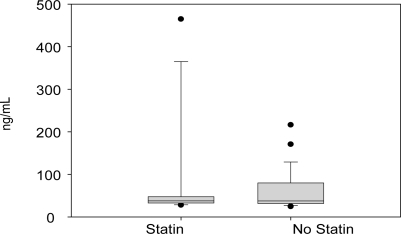
Figure 2 Serum activity of MMP2 according to statin use; median values were 209 and 211 ng/mL, respectively (p = 0.394).
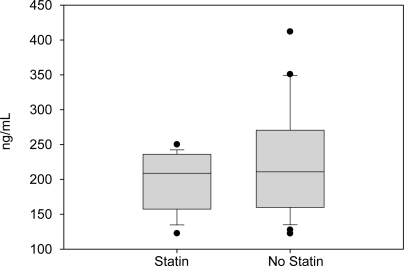
Figure 3 Serum levels of IL10 according to statin use; median values were 6 and 5 pg/mL, respectively (p = 0.679).
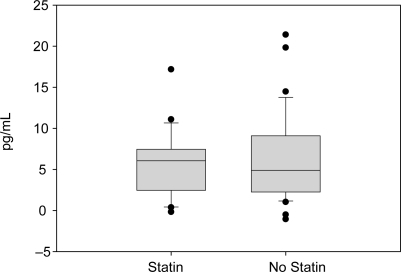
Figure 4 Serum levels of IL6 according to statin use; median values were 5 and 7 pg/mL, respectively (p = 0.085).
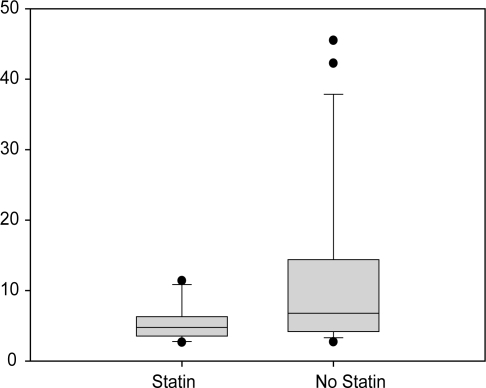
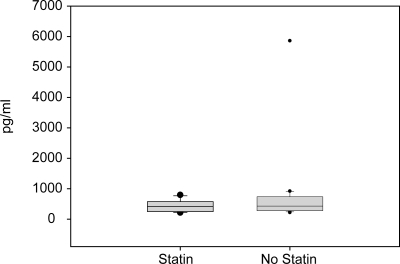
Figure 5 Serum activity of OPG according to statin use; median values did not differ significantly: 417 vs 430 pg/mL, respectively (p = 0.369).
Biomarker activity as a function of AAA diameter
To test the correlation of biomarker activity and AAA diameter, patients were divided into 3 groups: AAA diameter ≤5 cm, 5.1–6.0 cm, >6.0 cm. Using this separation there was no difference in the serum activity of MMP2, MMP9, OPG, and IL10; aneurysms >6 cm in diameter showed significantly higher levels of IL6 than smaller aneurysms ().
Table 2 Correlation of biomarker activity and aneurysm diameter
Discussion
This in vivo study examined the association between statin treatment and the serum activity of potent matrix remodeling proteases and inflammatory cytokines known to be present in patients suffering from aortic aneurysm. In recent years increasing understanding of the pathogenesis of AAA has generated hope that pharmacotherapy can be applied to patients with small aortic aneurysms (CitationDiehm et al 2007). In vitro and in vivo data have been published that show that HMG CoA reductase inhibitors (statins) may limit AAA growth by inhibitory action on MMP activity in the aortic wall (CitationSchouten et al 2006; CitationEvans et al 2007). Hence statin therapy is now recommended in the conservative management of patients with aortic aneurysms to slow aneurysm growth rate (CitationGolledge et al 2006). Circulating levels of MMPs and OPG are elevated in aneurysm patients, and monitoring of these markers may be helpful in managing these patients and surveying medical treatment. In patients with unstable angina, statin administration reduces circulating levels of inflammatory markers (CitationTousoulis et al 2006). In patients with aortic aneurysms no data are available on circulating levels of MMPs and other inflammatory cytokines in relation to statin therapy. Hence we analyzed blood samples from patients undergoing elective infrarenal aortic aneurysm repair for the levels of MMP2 and MMP9, OPG, and IL6 and 10 and correlated the data to statin therapy and aneurysm diameter. Surprisingly, statin therapy was not correlated to the circulating levels of the investigated biomarkers. Serum levels in patients on statin therapy were similar to those in patients without statin therapy. Correlation to aneurysm diameter did not reveal significant differences between small, medium-sized, and large aneurysms: patients with small aneurysms, smaller than 5 cm, showed similar activity of MMPs, OPG, and IL10 as did patients with aneurysms larger than 5 cm; however, patients with aneurysms larger than 6 cm showed significantly higher levels of IL6 than patients with smaller aneurysms. This result is in line with those of other investigators who demonstrated that the aortic aneurysm was the source of IL6 and who correlated IL6 levels to aneurysm surface (CitationDawson et al 2007). Nevertheless, our results partly contradict findings that showed that MMP2 levels were correlated to aneurysm expansion and MMP9 levels to aneurysm rupture (CitationPetersen et al 2002). Other investigators have reported on elevated serum levels of MMP9 in AAA compared with healthy controls and patients with aorto-iliac occlusive disease (CitationMcMillan and Pearce 1999; CitationHovsepian et al 2000). However, in this context several issues are now discussed.
First: studies on human blood samples in patients with aortic aneurysm are limited, as patients are usually referred for surgical repair; therefore our measurements are only snapshots in the course of aneurismal expansion and no data on growth rates were available. So the relationship between statin treatment and aneurysm expansion could not be determined – a problem that has already been confirmed by other investigators (CitationAbisi et al 2008). Subsequently the lack of correlation between statin therapy and biomarker activity may not necessarily document a lack of effect of statins on aneurysm growth.
Second: Results are contradictory on the relationship between circulating levels of MMPs and degenerative mechanisms in the wall of aortic aneurysms. On the one hand it has been shown that circulating MMP9 levels fell significantly after aneurysm exclusion (CitationWatanabe et al 2006); on the other hand the negative predictive value of normal MMP9 levels is about 52% (CitationHovsepian et al 2000). It appears that proteinases from the tissue compartment – the aortic wall – are not released to the plasmatic compartment and therefore MMP levels in the serum of patients do not reflect the situation in the aneurismal wall. Hence further investigations should focus on the correlation between tissue activitiy and serum activitiy in patients with AAA.
Third: Most studies on the role of MMPs and other inflammatory markers in aortic aneurysms use healthy volunteers or patients with arterial occlusive disease as control. Only a few investigations have compared patients with aortic aneurysm and statin therapy (CitationEvans et al 2007; CitationAbisi et al 2008).
Finally, the power of our investigation was limited (<20%) and the lack of significant correlations may be related to the relatively small number of patients. However, our results, together with published research, suggest that statins may exert an inhibitory effect on proteolytic activity in the aneurismal wall which is not reflected in the serum of aneurysm patients; hence it remains questionable if MMPs and other inflammatory markers such as ILs and OPG can serve as biomarkers in aneurismal disease. In addition the precise mechanisms of statin therapy in the conservative treatment of aortic aneurysm have yet to be examined. To elucidate the role of statins on aneurysm growth long-term follow up in clinical trials would be necessary. However, statins have been documented to be associated with reduced cerebro-cardio-vascular mortality in vascular patients and patients undergoing AAA surgery (CitationKertai et al 2004; CitationWelten et al 2007). Consequently most vascular patients are on statin treatment and such a clinical trial would prove ethically impossible. Nevertheless, further investigations on the mechanisms of aneurysm growth and effects of pharmacological agents are necessary to develop the best treatment regimen for patients with aortic aneurysms.
Disclosures
The authors have no conflicts of interest to disclose.
References
- AbisiSBurnandKGHumphriesJ2008Effect of statins on proteolytic activity in the wall of abdominal aortic aneurysmsBr J Surg95333717968978
- AnnabiBShédidDGhosnP2002Differential regulation of matrix metalloproteinase activities in abdominal aortic aneurysmsJ Vasc Surg355394611877705
- DawsonJCockerillGWChokeE2007Aortic aneurysms secrete interleukin-6 into the circulationJ Vasc Surg45350617264016
- DiehmNDickFSchaffnerT2007Novel insight into the pathobiology of abdominal aortic aneurysm and potential future treatment conceptsProg Cardiovasc Dis502091717976505
- EvansJPowellJTSchwalbeE2007Simvastatin attenuates the activity of matrix metalloprotease-9 in aneurysmal aortic tissueEur J Vasc Endovasc Surg34302317574455
- GolledgeJMullerJDaughertyA2006Abdominal aortic aneurysm: pathogenesis and implications for managementArterioscler Thromb Vasc Biol2626051316973970
- HovsepianDMZiporinSJSakuraiMK2000Elevated plasma levels of matrix metalloproteinase-9 in patients with abdominal aortic aneurysms: a circulating marker of degenerative aneurysm diseaseJ Vasc Interv Radiol1113455211099248
- KalyanasundaramAElmoreJRManazerJR2006Simvastatin suppresses experimental aortic aneurysm expansionJ Vasc Surg431172416414398
- KertaiMDBoersmaEWesterhoutCM2004A combination of statins and beta-blockers is independently associated with a reduction in the incidence of perioperative mortality and nonfatal myocardial infarction in patients undergoing abdominal aortic aneurysm surgeryEur J Vasc Endovasc Surg283435215350554
- LindholtJSVammenSFastingH2000The plasma level of matrix metal-loproteinase 9 may predict the natural history of small abdominal aortic aneurysms. A preliminary studyEur J Vasc Endovasc Surg20281510986027
- McMillanWDPearceWH1999Increased plasma levels of metalloproteinase-9 are associated with abdominal aortic aneurysmsJ Vasc Surg291227 discussion 127–99882796
- MoranCSMcCannMKaranM2005Association of osteoprotegerin with human abdominal aortic aneurysm progressionCirculation11131192515939823
- PetersenEWågbergFAngquistKA2002Proteolysis of the abdominal aortic aneurysm wall and the association with ruptureEur J Vasc Endovasc Surg23153711863333
- SchoutenOvan LaanenJHBoersmaE2006Statins are associated with a reduced infrarenal abdominal aortic aneurysm growthEur J Vasc Endovasc Surg3221616520071
- TamarinaNAMcMillanWDShivelyVP1997Expression of matrix metalloproteinases and their inhibitors in aneurysms and normal aortaSurgery12226471 discussion 271–29288131
- TousoulisDAntoniadesCKatsiV2006The impact of early administration of low-dose atorvastatin treatment on inflammatory process, in patients with unstable angina and low cholesterol levelInt J Cardiol109485216002160
- TziakasDNChalikiasGKParissisJT2004Serum profiles of matrix metalloproteinases and their tissue inhibitor in patients with acute coronary syndromes. The effects of short-term atorvastatin administrationInt J Cardiol942697715093992
- WatanabeTSatoASawaiT2006The elevated level of circulating matrix metalloproteinase-9 in patients with abdominal aortic aneurysms decreased to levels equal to those of healthy controls after an aortic repairAnn Vasc Surg203172116779512
- WeltenGMChoncholMHoeksSE2007Statin therapy is associated with improved outcomes in vascular surgery patients with renal impairmentAm Heart J1549546117967603