Abstract
Most of the late diabetic complications such as retinopathy, nephropathy, and neuropathy, have their basis in disturbed microvascular function. Structural and functional changes in the micro-circulation are present in diabetes mellitus irrespective of the organ studied, and the pathogenesis is complex. Endothelial dysfunction, characterized by an imbalance between endothelium-derived vasodilator and vasoconstrictor substances, plays an important role in the pathogenesis of diabetic microangiopathy. Increased circulating levels of endothelin-1 (ET-1), a potent vasoconstrictor peptide, has been found in patients with diabetes, and a positive correlation between plasma ET-1 levels and microangiopathy in patients with type 2 diabetes has been demonstrated. In addition to its direct vasoconstrictor effects, enhanced levels of ET-1 may contribute to endothelial dysfunction through inhibitory effects on nitric oxide (NO) production. Vascular endothelial dysfunction may precede insulin resistance, although the feature of insulin resistance syndrome includes factors that have negative effects on endothelial function. Furthermore, ET-1 induces a reduction in insulin sensitivity and may take part in the development of the metabolic syndrome. In the following, the mechanisms by which ET-1 contributes to the development of diabetic microangiopathy and the potentially beneficial effect of selective ETA receptor antagonists are discussed.
Introduction
Incidence and prevalence rates of type 2 diabetes are rising in most countries (CitationKing et al 1998). Diabetes mellitus is associated with an increased risk of cardiovascular diseases related to both macro- and microangiopathy, eg, myocardial infarction, peripheral arterial occlusive disease, stroke, retino-, neuro-, and nephropathies, causing considerable disability and premature death in individuals with diabetes. Diabetic skin microangiopathy contributes to the development of chronic foot ulcers, a common and severe complication often leading to major disability and increased mortality and also frequently resulting in amputation of the leg (CitationJeffcoate et al 2003). Endothelium-dependent vasodilation is impaired in the skin microcirculation of patients with type 2 diabetes (CitationCaballero et al 1999). Furthermore, autonomic neuropathy may cause increased shunting of blood through arteriovenous anastomoses and lead to impaired circulation through nutritive capillaries (CitationBoulton et al 1982; CitationFagrell et al 1999; CitationTooke 2000). Endothelial dysfunction, characterized by an imbalance between endothelium-derived vasodilator and vasoconstrictor substances, plays an important role in the pathogenesis of vascular complications in diabetes, including microangiopathy (CitationTooke 1995; CitationCreager et al 2003; CitationLuscher et al 2003).
Diabetic microangiopathy
The microcirculation comprises the arterioles, capillaries, venules, and lymphatics, all <100 μm in diameter. These vessels are crucial for maintaining tissue metabolism. Structural and functional changes in the microcirculation are present in diabetes mellitus irrespective of the organ studied. We have shown that functional disturbances in the skin microcirculation of the fingers are present three years after the onset of type 1 diabetes, and the majority of the patients have developed disturbances after 7–12 years (Kalani et al pers comm). The pathophysiology of diabetic microangiopathy is complex in that it involves not only metabolic, but also genetic factors. Subjects with diabetes heredity show impaired microvascular responses to both endothelium- and nonendothelium-dependent stimuli in the skin microcirculation in spite of normal body dimensions, normal glucose tolerance, and normal insulin sensitivity (CitationJörneskog et al 2005). Early on in the course of the disease, microvascular perfusion is increased in many organs under resting conditions (CitationTooke 1983Tooke 1986). A cutaneous microvascular overperfusion occurs in the limbs, but most of the blood flow under normal thermal conditions passes through arteriovenous shunts, bypassing the nutritive capillary bed and leading to so-called “capillary ischemia” (CitationBoulton et al 1982; CitationTooke 1983; CitationFagrell et al 1999). Increased skin microvascular perfusion has been shown to be related to poor glycemic control (CitationGundersen et al 1974; CitationTymms et al 1988; CitationJörneskog et al 1998). It should be pointed out that the early microvascular hyperemia occurs only under resting conditions, while under conditions that stress the microcirculation, eg, tissue injury or a period of arterial occlusion, a limited hyperemic response is observed (CitationRayman et al 1986; CitationWalmsley et al 1989; CitationSandeman et al 1991). This has been clearly demonstrated by investigations of the nutritive skin capillary flow (capillary blood cell velocity; CBV) in diabetic feet using videophotometric capillaroscopy, along with measurements of the total skin microcirculation by laser Doppler fluxmetry (LDF), demonstrating reduced skin capillary hyperemia in terms of the post-occlusive peak value obtained and the time taken to reach peak flow (CitationWalmsley et al 1989; CitationTur et al 1991; CitationJörneskog 1995).
There are, however, probably differences in the pathogenesis of microangiopathy between type 1 and type 2 diabetes. In type 2 diabetes, there is a complex interaction between impaired insulin sensitivity, vascular endothelial dysfunction, and hypertension, which seems to play an important role in the development of functional disturbances in the microcirculation. Impaired insulin sensitivity is associated with a modification of arterial resistance and increased peripheral microvascular resistance, which contributes to the excessive prevalence of hypertension in type 2 diabetes. In these patients, an increased peripheral microvascular resistance occurs with even minor degrees of impaired glucose tolerance, which coexists with disturbed capillary pressure autoregulation, leading to the development of irreversible structural changes in the microvasculature (CitationGall et al 1991; CitationJaap et al 1994; CitationShore et al 1994).
Endothelin-1
Endothelin-1 (ET-1) is the principal cardiovascular isoform of the endothelin system (CitationYanagisawa et al 1988). Vascular ET-1 is produced primarily in the endothelium, although it can also be produced in vascular smooth muscle cells (VSMC), macrophages, leukocytes, cardiomyocytes, and fibroblasts (CitationResink et al 1990; CitationProperzi et al 1995). In the kidney, tubular epithelial cells, mesangial cell, and podocytes are capable of ET-1 release (CitationKohan 1997). Several mechanisms are involved in the clearance of ET-1 from plasma, including endocytosis in the lungs, enzymatic degradation, degradation of the endothelin B-receptor-ligand complex, and enzymatic processes in the kidney and liver (CitationAnggard et al 1989; CitationAbassi et al 1992; CitationJohnström et al 2005). Two receptor subtypes, endothelin A- and B-receptors (ETA and ETB), mediate the effects of ET-1. Vascular smooth muscle cells express both ETA and ETB, while endothelial cells express primarily ETB (CitationMolenaar et al 1993). On smooth muscle cells, ETA mediates vasoconstriction and mitogenesis, while ETB receptor has a dual function and has been shown to cause both vasoconstriction and vasodilation (CitationSakurai et al 1992; CitationSeo et al 1994). ETA receptor activation contributes to coronary constrictor tone and peripheral and coronary endothelial dysfunction (CitationKyriakides et al 2000; CitationHalcox et al 2001). In isolated human internal mammary and porcine coronary arteries, ETB receptor mediates ET-1-induced vasoconstriction (CitationSeo et al 1994). In healthy humans, selective ETB receptor antagonism increases peripheral vascular resistance, which means that vasodilation is the favored ETB pathway (CitationStrachan et al 1999). However, the balance between vasodilator and vasoconstrictor ETB pathways may be altered in pathological conditions (CitationCardillo et al 1999; CitationPernow et al 2000).
ET-1 is one of the most potent vasoconstrictors described and has been suggested to be involved in the development of cardiovascular disease. ET-1 also has pro-inflammatory and profibrotic effects, which may contribute to the pathogenesis of cardiovascular disease. Endogenous ET-1 is important for maintaining vascular tone, and enhanced endogenous ET-1 has been demonstrated in hypertension, coronary artery disease, and heart failure (CitationCardillo et al 1999, Citation2000; CitationCowburn et al 1999; CitationLove et al 2000; CitationNohria et al 2003).
The role of endothelin-1 in diabetic microangiopathy
The pathophysiology of diabetic microangiopathy is complex and many important aspects of it still are not fully understood. The major microvascular complications of diabetes are nephropathy, retinopathy, neuropathy, and skin microangi-opathy. Both metabolic and hemodynamic factors contribute to the development of diabetic microvascular complications (CitationCooper 1998; CitationGroop et al 2005), which, in spite of similar final clinical manifestations in both type of diabetes, probably have different pathophysiological pathways regarding the organ and/or complication studied. In type 2 diabetes, endothelial dysfunction is an early feature of the disease, linking cardiovascular risk factors and insulin resistance in different pathways to clinically manifest cardiovascular complications (CitationJansson 2007; CitationRask-Madsen et al 2007). The vascular endothelium maintains vascular tone and has important hemostatic function, and endothelial dysfunction is of major importance in the pathogenesis of atherosclerosis and diabetic angiopathy (CitationTooke et al 2000; CitationRask-Madsen et al 2007). Several studies support the hypothesis that endothelial dysfunction is a precursor of type 2 diabetes, indicating that vascular endothelial dysfunction may precede insulin resistance, although the features of insulin resistance syndrome include factors that have negative effects on endothelial function (CitationTooke et al 2000; CitationGroop et al 2005; CitationJansson 2007; CitationRask-Madsen et al 2007). Impaired endothelial-dependent and independent microvascular reactivity has also been demonstrated in healthy subjects with risk factors for type 2 diabetes (CitationCaballero et al 1999; CitationJörneskog et al 2005). One important feature of endothelial dysfunction is an increased production and biological activity of the potent vasoconstrictor and proinflammatory peptide ET-1. Elevated levels of ET-1 are found in patients with type 2 diabetes (CitationTakahashi et al 1990; CitationVerhaar et al 1998; CitationMather et al 2002), and ET-1-induced reduction in insulin sensitivity may take part in the development of the metabolic syndrome (CitationAhlborg et al 2002). In diabetes mellitus, a primary disturbance in ET-1 production from vascular endothelium exists as an early phenomenon rather than a result of advanced stage of the disease (CitationDonatelli et al 1994; CitationAnfossi et al 2007).
Furthermore, ET-1 may contribute to the development of endothelial dysfunction, and consequently insulin resistance, by increasing the production of reactive oxygen species, mainly superoxide anion, in the vasculature. This is mainly dependent upon the activation of NADPH oxidase protein expression and activity (CitationWedgwood et al 2001; CitationLi et al 2003; CitationRomero et al 2008).
Diabetic nephropathy
ET-1 is secreted by glomerular endothelial cells, mesangial cells, and epithelial cells. Activation of endothelin receptors in the kidney leads to constriction of renal vessels, inhibition of salt and water reabsorption, and enhanced glomerular proliferation. Alterations in ET-1, at both mRNA and receptor levels are seen in animal models of diabetes. Several human studies show a correlation between plasma or urinary levels of ET-1 and signs of diabetic nephropathy at different stages in terms of an increased glomerular filtration rate, mesangial expansion, macro- and/or microalbuminuria, and uremia (CitationLee et al 1994; CitationDe Mattia et al 1998; CitationAk et al 2001;CitationCandido et al 2002; CitationZanatta et al 2008). However, most of the interventional studies on selective or dual endothelin receptor blockers have been done in animal models with encouraging results (CitationChade et al 2006; CitationSasser et al 2007).
Diabetic neuropathy
Diabetic neuropathy is one of the most frequent and expensive complications of diabetes. The peripheral sensorimotor and autonomic neuropathies play an important role in the pathogenesis of diabetic foot ulceration. Sympathetic neuropathy also results in arteriovenous shunting, leading to impaired blood flow through nutritive capillaries. Both hemodynamic and metabolic factors contribute to the development of diabetic neuropathy. Microvascular dysfunction is seen at an early stage in the peripheral nerve, which contributes to impaired endoneurial blood flow, leading to destruction of neuronal and Schwann cells and, finally, nerve degeneration (CitationLow et al 1989; CitationCameron et al 1991, Citation1995). In patients with diabetes, endoneurial microangiopathy, and in particular basement membrane thickening, is related to clinical and neuro-physiological measures of neuropathy. Endoneurial capillary microangiopathy presages deterioration in glucose tolerance and seems to be an early and persistent feature in the processes underlying diabetic peripheral neuropathy (CitationThrainsdottir et al 2003). Interestingly, diabetic patients without evidence of neuropathy demonstrate endoneurial microangiopathy. Microangiopathy may therefore precede the development of peripheral neuropathy (CitationGiannini et al 1995).
ET-1 contributes to endothelial abnormalities and the altered balance of vasodilation and vasoconstriction in favor of the latter in diabetes. Furthermore, endothelin receptors are expressed in neurons and glial cells and are probably involved in the transduction of nociceptive information (CitationGokin et al 2001). ETA receptor blockade attenuates tactile allodynia in the streptozotocin-induced diabetic rat, suggesting that ETA receptors may contribute to the development of peripheral neuropathy in experimental diabetes (CitationJarvis et al 2000). Interestingly, a protective role for ETB receptors following neuronal injury has been described (CitationSiren et al 2002; CitationBerti-Mattera et al 2006).
Diabetic retinopathy
Diabetic retinopathy is a potentially sight-threatening complication that develops in nearly all patients with diabetes. Ocular tissues, eg, vascular and extravascular sites in the retina are a rich source of ET-1 expression, and ET-1 contributes to abnormal retinal hemodynamics in diabetic retinopathy (CitationKohner et al 1995; CitationPang et al 1997). Results from several studies in streptozotocin-induced diabetic rats have suggested a role of ET-1 in the pathogenesis of diabetic retinopathy (CitationChakrabarti et al 1997, Citation1998). An interaction between ET-1 and vascular endothelial growth factor (VEGF) has also been reported, and some positive results of treatment with endothelin receptor blockers have raised interest in these substances as potentially therapeutic agents (CitationMasuzawa et al 2006). However, most of the studies on the role of ET-1 in the pathogenesis of diabetic retinopathy and the importance of endothelin blockers in the treatment of this serious complication have been done in animal models. There is, however, sufficient evidence that strongly links ET-1 to the pathogenesis of diabetic retinopathy.
Diabetic skin microangiopathy
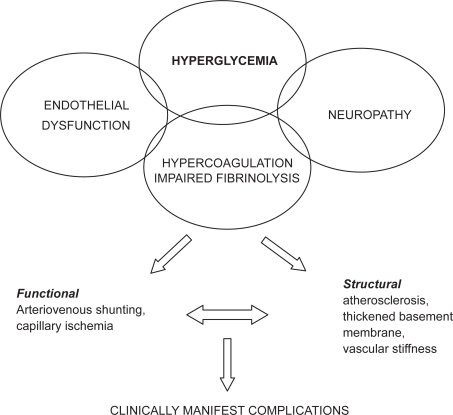
The pathogenesis of diabetic skin microangiopathy is complex (). Functional diabetic microangiopathy is characterized by reduced microvascular reactivity and increased blood flow through arteriovenous shunts leading to an impaired nutritive capillary circulation, so-called capillary ischemia (CitationBoulton et al 1982; CitationFagrell et al 1999; CitationTooke 2000). Impaired nutritive capillary circulation is especially pronounced in patients with peripheral arterial occlusive disease (CitationJörneskog et al 1995). A state of hypercoagulation and impaired fibrinolysis is also present in diabetic patients and may contribute to the deterioration of the skin microcirculation (CitationKalani et al 2007).
Figure 1 Pathogenesis of diabetic skin microangiopathy.
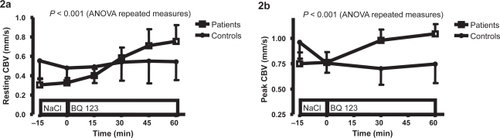
Recently, we have shown that ETA receptor blockade by BQ123 markedly increases the nutritive skin microcirculation in patients with type 2 diabetes and microangiopathy (CitationSettergren et al 2008). The results suggest that ET-1, through activation of the ETA receptor, is of importance for the regulation of the microcirculation in diabetic patients with micro-angiopathy. The skin nutritive microcirculation determined by nailfold capillary microscopy and the hyperemic response, ie, the peak value of the CBV following arterial occlusion, increased significantly during ETA receptor blockade, indicating improved microvascular reactivity () (CitationSettergren et al 2008). Interestingly, the increase in CBV during selective ETA receptor blockade was more pronounced in type 2 diabetic patients with a high body mass index (BMI) and low levels of insulin-like growth factor binding protein-1 (IGFBP-1), supporting the existence of a close relationship between insulin resistance and increased ET-1 activity. It is noteworthy that administration of the selective ETA receptor antagonist did not affect CBV in the nondiabetic control group. This supports the notion that the ET-1 system is upregulated in patients with type 2 diabetes and that ETA receptor blockade exerts hemodynamic effects only under such conditions.
Figure 2 Effect of BQ123 on resting capillary blood cell velocity (CBV) (a) and peak capillary blood cell velocity following a 1-min arterial occlusion (b) in patients with type 2 diabetes (n = 10) and nondiabetic controls (n = 8). Data are shown as the mean and SEM. A significant difference between groups in the change in resting CBV and peak CBV, respectively, following a 60-min infusion of BQ123 is shown. Copyright © 2008. Reproduced with the kind permission of Karger AG, Basel from CitationSettergren M, Pernow J, Brismar K, et al 2008. Endothelin-A receptor blockade improves nutritive skin capillary circulation in patients with type 2 diabetes and albuminuria. J Vasc Res, 45:295–302.
Enhanced ET-1–mediated vasoconstriction of precapillary resistance vessels leads to impaired blood flow through nutritive capillaries and increased arteriovenous shunting in patients with type 2 diabetes. These patients are prone to arterial hypertension, partly due to vasoconstriction of precapillary resistance vessels, leading to an increased capillary blood pressure (CitationFegan et al 2003) due to disturbed autoregulation of capillary pressure as a consequence of insulin resistance. A reduction in capillary blood pressure, as a consequence of reduced arteriovenous shunt flow and an increased arteriovenous pressure difference, might increase the capillary blood circulation (CitationFegan et al 2003). The effects of selective ETA receptor blockade on the skin microcirculation may be a consequence of blocking the precapillary constrictor effects of ET-1 mediated by ETA receptors. Furthermore, improvements in peak CBV reflect vasodilation at the precapillary level, indicating improved precapillary and capillary endothelial function.
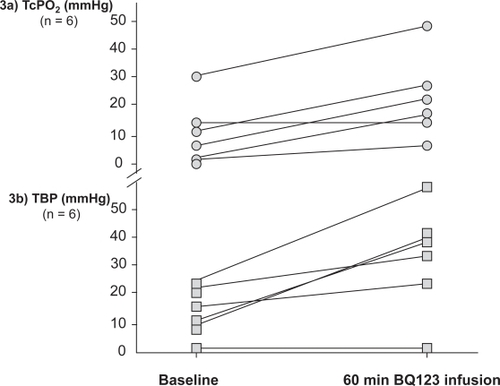
Diabetic foot ulcers in the presence of peripheral arterial disease threatens both life and limb in these patients. However, the local nutritive skin microcirculation is severely deteriorated in diabetic patients with peripheral arterial occlusive disease and new treatments are urgently needed. We conducted a pilot study to investigate whether ETA receptor blockade improves peripheral tissue perfusion in diabetic patients with critical limb ischemia. During infusions of the selective ETA receptor blocker BQ123, transcutaneous oxygen tension (TcPO2) at the dorsum of the foot and toe blood pressure (TBP) increased significantly () (CitationKalani et al 2008). The increased local skin oxygenation during infusions of BQ123 suggests an improved nutritive capillary circulation. TcPO2 may partly reflect local nutritive capillary circulation and has been suggested for the evaluation of peripheral arterial disease and the prediction of ulcer outcomes (CitationKalani et al 1999). Increased TBP during ETA receptor blockade may be due to vasodilation of precapillary resistance vessels. The observed effect of ETA receptor blockade on peripheral tissue perfusion in these patients may be a consequence of blocking the precapillary constrictor effects of ET-1 mediated by ETA receptors. Furthermore, ETA receptor blockade has been shown to improve endothelium-dependent vasodilation by enhancing the bioavailability of nitric oxide, which appears to be of importance for microvascular function in diabetes (CitationMather et al 2002). In addition to the increased levels of ET-1 in patients with diabetes, as compared to nondiabetic controls (CitationSettergren et al 2008), there are also indications of upregulation of ET receptors in diabetes (CitationKhan et al 2003). The marked increase in peripheral blood flow observed following BQ123 infusion in the diabetic patients may therefore be related to increased production of ET-1 as well as an upregulation of ETA receptors mediating vasoconstriction.
Figure 3 Effects of a 60-min infusion of a selective ETA receptor antagonist (BQ123) on transcutaneous oxygen tension (TcPO2) and toe blood pressure (TBP) in six patients with type 2 diabetes and critical limb ischemia.
Conclusions
Disturbed microvascular function in diabetes, ie, diabetic microangiopathy, plays an important role in the pathogenesis of specific complications in different organs. Impaired nutritive skin microcirculation has been demonstrated in both the diabetic hand and foot and might contribute to the development of such complications as sensorimotor neuropathy and nonhealing ulcers. ET-1 is a potent vasoconstrictor, proinflammatory, and mitogenic peptide produced by endothelial cells, VSMC, and inflammatory cells. The production and the plasma levels of ET-1 are elevated in patients with diabetes, and a positive correlation between plasma ET-1 levels and diabetic microangiopathy has been reported, suggesting a potential role of the endothelin system in the pathophysiology of vascular complications in diabetes. A large body of evidence from animal models and human studies indicates that ET-1 is causally involved in the pathogenesis of diabetic microangiopathy, but the potential of ET-1 blockers in the treatment of diabetic microangiopathy has not been investigated in human studies. Nevertheless, recent results from our studies in patients with diabetes indicate that targeting the ET-1 system might be of importance in the treatment of complications related to diabetic microangiopathy.
Acknowledgements
The author’s own studies were supported by grants from the Swedish Research Council and the Stockholm County Council. Perimed AB, Stockholm, Sweden, supported the studies with the equipment used to measure the peripheral macro- and microcirculation. The author reports no conflicts of interest in this work.
References
- AbassiZATateJEGolombE1992Role of neutral endopeptidase in the metabolism of endothelinHypertension2089951618556
- AhlborgGLindströmJ2002Insulin sensitivity and big ET-1 conversion to ET-1 after ETA- or ETB-receptor blockade in humansJ Appl Physiol9321122112391119
- AkGBuyukberberSSevincA2001The relation between plasma endothelin-1 levels and metabolic control, risk factors, treatment modalities, and diabetic microangiopathy in patients with type 2 diabetes mellitusJ Diabetes Complications15150711358684
- AnfossiGRussoIDoronzoG2007Relevance of the vascular effects of insulin in the rationale of its therapeutical useCardiovasc Hematol Disord Drug Targets72284918220724
- AnggardEGaltonSRaeG1989The fate of radioiodinated endothelin-1 and endothelin-3 in the ratJ Cardiovasc Pharmacol13S46S492473326
- Berti-MatteraLNGariepyCEBurkeRM2006Reduced expression of endothelin B receptors and mechanical hyperalgesia in experimental chronic diabetesExp Neurol20139940616806184
- BoultonAJScarpelloJHWardJD1982Venous oxygenation in the diabetic neuropathic foot: evidence of arteriovenous shunting?Diabetologia22687060849
- CaballeroAEAroraSSaouafR1999Microvascular and macro-vascular reactivity is reduced in subjects at risk for type 2 diabetesDiabetes4818566210480619
- CameronNECotterMALowPA1991Nerve blood flow in early experimental diabetes in rats: relation to conduction deficitsAm J Physiol261E1E81858864
- CameronNECotterMA1995Neurovascular dysfunction in diabetic rats. Potential contribution of autoxidation and free radicals examined using transition metal chelating agentsJ Clin Invest961159637635953
- CandidoRAllenTJ2002Haemodynamics in microvascular complications in type 1 diabetesDiabetes Metab Res Rev1828630412203944
- CardilloCKilcoyneCMCannonRO2000Increased activity of endogenous endothelin in patients with hypercholesterolemiaJ Am Coll Cardiol361483811079646
- CardilloCKilcoyneCMWaclawiwM1999Role of endothelin in the increased vascular tone of patients with essential hypertensionHypertension33753810024340
- ChadeARKrierJDTextorSC2006Endothelin-A receptor blockade improves renal microvascular architecture and function in experimental hypercholesterolemiaJ Am Soc Nephro173394403
- ChakrabartiSGanXTMerryA1998Augmented retinal endothelin-1, endothelin-3, endothelinA and endothelinB gene expression in chronic diabetesCurr Eye Res1730179543639
- ChakrabartiSSimaAA1997Endothelin-1 and endothelin-3-like immuno-reactivity in the eyes of diabetic and non-diabetic BB/W ratsDiabetes Res Clin Pract37109209279481
- CooperME1998Pathogenesis, prevention, and treatment of diabetic nephropathyLancet3529123213199683226
- CowburnPJClelandJGMcArthurJD1999Endothelin B receptors are functionally important in mediating vasoconstriction in the systemic circulation in patients with left ventricular systolic dysfunctionJ Am Coll Cardiol33932810091818
- CreagerMALuscherTFCosentinoF2003Diabetes and vascular disease: pathophysiology, clinical consequences, and medical therapy: Part ICirculation10815273214504252
- De MattiaGCassone-FaldettaMBelliniC1998Role of plasma and urinary endothelin-1 in early diabetic and hypertensive nephropathyAm J Hypertens1198389715792
- DonatelliMCollettiIBucaloML1994Plasma endothelin levels in NIDDM patients with macroangiopathyDiabetes Res25159647648786
- FagrellBJorneskogGIntagliettaM1999Disturbed microvascular reactivity and shunting – a major cause for diabetic complicationsVasc Med4125710512590
- FeganPGTookeJEGoodingKM2003Capillary pressure in subjects with type 2 diabetes and hypertension and the effect of antihypertensive therapyHypertension4111111712695416
- GallMARossingPSkottP1991Prevalence of micro- and macroalbuminuria, arterial hypertension, retinopathy and large vessel disease in European type 2 (non-insulin-dependent) diabetic patientsDiabetologia34655611955098
- GianniniCDyckPJ1995Basement membrane reduplication and pericyte degeneration precede development of diabetic polyneuropathy and are associated with its severityAnn Neurol374985047717686
- GokinAPFareedMUPanHL2001Local injection of endothelin-1 produces pain-like behaviour and excitation of nociceptors in ratsJ Neurosci2153586611438612
- GroopPHForsblomCThomasMC2005Mechanisms of disease: Pathway-selective insulin resistance and microvascular complications of diabetesNat Clin Pract Endocrinol Metab11001016929378
- GundersenHJG1974Peripheral blood flow and metabolic control in juvenile diabetesDiabetologia10225314845723
- HalcoxJPNourKRZalosG2001Coronary vasodilation and improvement in endothelial dysfunction with endothelin ET(A) receptor blockadeCirc Res899697611717152
- JaapAJHammersleyMSShoreAC1994Reduced microvascular hyper-aemia in subjects at risk of developing type 2 (non-insulin-dependent) diabetes mellitusDiabetologia37214168163058
- JanssonP-A2007Endothelial dysfunction in insulin resistance and type 2 diabetesJ Intern Med2621738317645585
- JarvisMFWessaleJLZhuCZ2000ABT-627, an endothelin ET(A) receptor-selective antagonist, attenuates tactile allodynia in a diabetic rat model of neuropathic painEur J Pharmacol388293510657544
- JeffcoateWJHardingKG2003Diabetic foot ulcersLancet36115455112737879
- JohnströmPFryerTDRichardsHK2005Positron emission tomography using 18F-labelled endothelin-1 reveals prevention of binding to cardiac receptors owing to tissue-specific clearance by ET B receptors in vivoBr J Pharmacol1441152215644875
- JörneskogGBrismarKFagrellB1995Skin capillary circulation is more impaired in toes of diabetic than non-diabetic patients with peripheral vascular diseaseDiabet Med1236417712701
- JörneskogGBrismarKFagrellB1998Pronounced skin capillary ischemia in the feet of diabetic patients with bad metabolic controlDiabetologia41410159562344
- JörneskogGKalaniMKuhlJ2005Early microvascular dysfunction in healthy normal-weight males with heredity for type 2 diabetesDiabetes Care281495715920077
- JörneskogG1995Functional Microangiopathy in the Digital Skin of Patients with Diabetes Mellitus [dissertation]Stockholm, SwedenKarolinska Institute
- KalaniMBrismarKFagrellB1999Transcutaneous oxygen tension and toe blood pressure as predictors for outcome of diabetic foot ulcersDiabetes Care221475110333917
- KalaniMPernowJBragdJ2008Improved peripheral perfusion during endothelin-A receptor blockade in patients with type 2 diabetes and critical limb ischemiaDiabetes Care31e5618594055
- KalaniMSilveiraABlombäckM2007Beneficial effects of dalteparin on haemostatic function and local tissue oxygenation in patients with diabetes, severe vascular disease and foot ulcersThromb Res1206536117275886
- KhanZAChakrabartiS2003Endothelins in chronic diabetic complicationsCan J Physiol Pharmacol816223412839273
- KingHAubertREHermanWH1998Global burden of diabetes 1995–2025: prevalence, numerical estimates and projectionsDiabetes Care211414319727886
- KohanDE1997Endothelins in the normal and diseased kidneyAm J Kidney Dis292269002526
- KohnerEMPatelVRassamSM1995Role of blood flow and impaired autoregulation in the pathogenesis of diabetic retinopathyDiabetes4460377789621
- KyriakidesZSKremastinosDTBofilisE2000Endogenous endothelin maintains coronary artery tone by endothelin type A receptor stimulation in patients undergoing coronary arteriographyHeart841768210908255
- LeeYJShinSJTsaiJH1994Increased urinary endothelin-1-like immunoreactivity in NIDDM patients with albuminuriaDiabetes Care1726368026280
- LiLFinkGDWattsSW2003Endothelin-1 increases vascular superoxide via endothelin(A)-NADPH oxidase pathway in low-renin hypertensionCirculation1071053812600921
- LoveMPFerroCJHaynesWG2000Endothelin receptor antagonism in patients with chronic heart failureCardiovasc Res471667210869543
- LowPALagerlundTDMcManisPG1989Nerve blood flow and oxygen delivery in normal, diabetic, and ischemic neuropathyInt Rev Neurobiol313554382557297
- LuscherTFCreagerMABeckmanJA2003Diabetes and vascular disease: pathophysiology, clinical consequences, and medical therapy: Part IICirculation10816556114517152
- MasuzawaKJesminSMaedaS2006Effect of endothelin dual receptor antagonist on VEGF levels in streptozotocin-induced diabetic rat retinaExp Biol Med23110904
- MatherKJMirzamohammadiBLteifA2002Endothelin contributes to basal vascular tone and endothelial dysfunction in human obesity and type 2 diabetesDiabetes5135172312453909
- MolenaarPO’ReillyGSharkeyA1993Characterization and localization of endothelin receptor subtypes in the human atrioventricular conducting system and myocardiumCirc Res72526387679333
- NohriaAGarrettLJohnsonW2003Endothelin-1 and vascular tone in subjects with atherogenic risk factorsHypertension4243812756218
- PangIHYorioT1997Ocular actions of endothelinsProc Soc Exp Biol Med21521349142135
- PernowJBohmFJohanssonBL2000Enhanced vasoconstrictor response to endothelin-B-receptor stimulation in patients with atherosclerosisJ Cardiovasc Pharmacol36S418S2011078438
- ProperziGTerenghiGGuXH1995Early increase precedes a depletion of endothelin-1 but not of von Willebrand factor in cutaneous microvessels of diabetic patients; a quantitative immunohistochemical studyJ Pathol175243527738721
- Rask-MadsenCKingGL2007Mechanisms of disease: endothelial dysfunction in insulin resistance and diabetesNat Clin Pract Endocrinol Metab3465617179929
- RaymanGWilliamsSASpencerPD1986Impaired microvascular hyperaemic response to minor skin trauma in type 1 diabetesBr Med J292129582939920
- ResinkTJHahnAWAScott-BurdenT1990Inducible endothelin messenger RNA expression and peptide secretion in cultured human vascular smooth muscle cellsBiochem Biophys Res Commun1681303102161221
- RomeroMJiménezRSánchezM2008Quercetin inhibits vascular superoxide production induced by endothelin-1: Role of NADPH oxidase, uncoupled eNOS and PKCAtherosclerosis316[Epub ahead of print].
- SakuraiTYanagisawaMMasakiT1992Molecular characterization of endothelin receptorsTrends Pharmacol Sci1310381315462
- SandemanDDPymCAGreenEM1991Microvascular vasodilata-tion in feet of newly diagnosed non-insulin dependent diabetic patientsBr Med J302112232043783
- SasserJMSullivanJCHobbsJL2007Endothelin A receptor blockade reduces diabetic renal injury via an anti-inflammatory mechanismJ Am Soc Nephrol181435417167119
- SeoBOemarBSSiebenmannR1994Both ETA and ETB receptors mediate contraction to endothelin-1 in human blood vesselsCirculation89120388124808
- SettergrenMPernowJBrismarK2008Endothelin-A receptor blockade improves nutritive skin capillary circulation in patients with type 2 diabetes and albuminuriaJ Vasc Res4529530218212505
- ShoreACJaapAJTookeJE1994Capillary pressure in patients with NIDDMDiabetes4311982027926288
- SirenALLewczukPHasselblattM2002Endothelin B receptor deficiency augments neuronal damage upon exposure to hypoxia-ischemia in vivoBrain Res945144912113963
- StrachanFESprattJCWilkinsonIB1999Systemic blockade of the endothelin-B receptor increases peripheral vascular resistance in healthy menHypertension3358159931169
- TakahashiKGhateiMALamHC1990Elevated plasma endothelin in patients with diabetes mellitusDiabetologia33306102198188
- ThrainsdottirSMalikRADahlinLB2003Endoneurial capillary abnormalities presage deterioration of glucose tolerance and accompany peripheral neuropathy in manDiabetes5226152214514647
- TookeJEHannemanMM2000Adverse endothelial function and the insulin resistance syndromeJ Int Med24742531
- TookeJE1983Capillary pressure in non-insulin-dependent diabetesInt Angiol216771
- TookeJE1983Microvascular haemodynamics in diabetes mellitusClin Sci70119253514078
- TookeJE1995Microvascular function in human diabetes. A physiological perspectiveDiabetes4472167789639
- TookeJE2000Possible pathophysiological mechanisms for diabetic angi-opathy in type 2 diabetesJ Diabetes Complications1419720011004428
- TurEYosipovitchBar-OnY1991Skin reactive hyperaemia in diabetic patients. A study by laser Doppler flowmetryDiabetes Care14958621797508
- TymmsDJTookeJE1988The effect of continuous subcutaneous insulin infusion (CSII) on microvascular blood flow in diabetes mellitusInt J Microcirc Clin Exp7347563220680
- VerhaarMCStrachanFENewbyDE1998Endothelin-A receptor antagonist-mediated vasodilatation is attenuated by inhibition of nitric oxide synthesis and by endothelin-B receptor blockadeCirculation9775269498538
- WalmsleyDWalesJKWilesPG1989Reduced hyperaemia following skin trauma: evidence for an impaired microvascular response to injury in the diabetic footDiabetologia3273692591641
- WedgwoodSMcMullanDMBekkerJM2001Role for endothelin-1-induced superoxide and peroxynitrite production in rebound pulmonary hypertension associated with inhaled nitric oxide therapyCirc Res893576411509453
- YanagisawaMKuriharaHKimuraS1988A novel potent vaso-constrictor peptide produced by vascular endothelial cellsNature332411152451132
- ZanattaCMGerchmanFBurttetL2008Endothelin-1 levels and albuminuria in patients with type 2 diabetes mellitusDiab Res Clin Pract80299304