Abstract
There is a need to evaluate oral glucose-lowering agents not only for their value in achieving glycemic control but also for their impact on cardiac risk factor modification. This article reviews the evidence base for the two thiazolinediones currently available, pioglitazone and rosiglitazone. These drugs exert their effects through actions affecting metabolic control, lipid profiles, and the vascular wall. They have been shown to be as efficacious in establishing glycemic control, in both monotherapy and combination therapy regimens, as more traditional oral agents, and may be able to sustain that control in the long term. Both thiazolidinediones have demonstrated favorable effects on markers of cardiovascular disease. Evidence from the large PROactive outcomes study suggests that pioglitazone may exert protective effects in patients with type 2 diabetes and macrovascular disease. Thiazolidinediones are generally well tolerated but they can cause weight gain, induce fluid retention, and may contribute to bone loss in postmenopausal women. The place of thiazolidinediones in the management of type 2 diabetes is well established. The potential for additional benefits in reducing macrovascular risk encourages further long-term study of these agents.
Introduction
The thiazolidinediones (TZDs, or glitazones) class, which currently includes rosiglitazone and pioglitazone, are effective and frequently prescribed treatments for type 2 diabetes that complement existing treatment approaches and form an important part of treatment algorithms. In the decade since their introduction, the prevalence of obesity, diabetes, and the metabolic syndrome has increased exponentially.Citation1–Citation3 Diabetes is also closely associated with cardiovascular disease – myocardial infarction and stroke are the major causes of premature death in people with diabetes, and type 2 diabetes is considered an independent risk equivalent for developing another vascular event.Citation4 The increasing prevalence of diabetes will therefore be closely followed by increases in cardiovascular-related morbidity and mortality. However, diabetes and cardiovascular disease develop only over time, providing a window of opportunity for interventions to prevent both diseases and/or delay their progression. As the use of glucose-lowering agents continues to increase and new agents appear, there is a growing need to evaluate products not only on the basis of their use in achieving glycemic control, but also in the context of their effect on global cardio-metabolic risk factor modification.
The TZDs are a unique class of oral glucose-lowering agents that work primarily by activating the nuclear transcription factor peroxisome proliferator-activated receptor gamma (PPAR-γ), thereby turning on and off specific genes for the regulation of glucose, lipids and protein metabolism. There is now considerable research to suggest, that beyond reducing insulin resistance and providing durable glycemic control, the TZDs exert a number of pleiotropic effects that may play an important role in the treatment of type 2 diabetes mellitus.
Documented evidence for the benefits of pioglitazone on cardiovascular outcomes in patients with type 2 diabetes has been provided by the results of the Prospective Pioglit-Azone Clinical Trial In Macrovascular Events (PROactive).Citation5 However, there has been recent debate about the possible differences between the two TZDs in terms of cardiovascular disease outcome.Citation6 In this context, the complex, nonoverlapping mechanisms of action and impact on metabolic parameters such as lipid profiles of pioglitazone and rosiglitazone may be relevant, making it unwise to extrapolate these results to other drugs in the class.
It therefore seems timely to review TZDs and their place in the management of type 2 diabetes. This review will focus on what is known about TZDs as a class and the current clinical evidence base regarding the efficacy and safety of individual agents. We consider the contemporary literature on TZDs, highlighting these agents’ multiple metabolic effects and summarizing the data relating to their clinical effectiveness in the management of type 2 diabetes (in terms of both glucose control and clinical outcomes) when used as monotherapy or in combination with other glucose-lowering agents.
Type 2 diabetes – complex pathogenesis
Type 2 diabetes is a complex disorder. Hyperglycemia is the core metabolic defect and combines with a range of metabolic risk factors to impart high risk for cardiovascular events. Insulin resistance and β-cell dysfunction both play important roles in the development and progression of type 2 diabetes.Citation7,Citation8 Evidence has shown, that while insulin resistance lays the groundwork for glucose intolerance, the progression to type 2 diabetes does not occur until a degree of β-cell dysfunction has taken place, allowing blood glucose levels to rise.Citation9,Citation10 Both defects remain closely linked with the progression of the disease – declining β-cell function is associated with deteriorating glycemic controlCitation11,Citation12 and insulin resistance is associated with numerous risk factors for cardiovascular disease.Citation13–Citation15
TZDs – rationale for a role in the management of diabetes
TZDs bind to the ligand-activated transcription factor PPAR-γ.Citation16 Members of the PPAR family (PPAR-α, -γ and -δ) play a pivotal role in the regulation of lipid metabolism and homeostasis and are important indirect as well as direct regulators of cellular insulin sensitivity. However, PPAR subtypes appear to have highly specialized functions when acting on endogenous genes.Citation17,Citation18 Thus, PPAR-α primarily activates genes encoding proteins involved in fatty acid oxidation. PPAR-δ is ubiquitously expressed in various tissues and is one of the key regulators of energy homeostasis in skeletal muscle. PPAR-γ is expressed predominantly in adipose tissue and skeletal muscle and is involved in the regulation of adipocyte proliferation and differentiation, as well as lipid storage.Citation19 This is achieved by an increase in the number of insulin-sensitive small adipocytes, which leads to a transfer of fat distribution from visceral to subcutaneous depots. The effect of PPAR-γ activation is to enhance the action of insulin in insulin-sensitive tissue by increasing glucose uptake in skeletal muscle and adipose tissue and decreasing hepatic glucose production.
While improvements in metabolic control and lipid profiles have important effects on cardiovascular disease in patients with diabetes, PPAR-γ agonists also have a range of independent actions on the vascular wall, which impacts on atherogenesis.Citation20,Citation21 PPAR-γ is expressed in vascular and inflammatory cells, where it interacts with several processes involved in the development and progression of atherosclerosis, particularly with respect to macrophage foam cell formation and the transcriptional regulation of genes mediating the inflammatory response. In preclinical studies, activation of PPAR-γ by TZDs acts on a number of pathogenic pathways implicated in the development of atherosclerosis, including inflammation, oxidative stress, metalloproteinase activity, advanced glycation end product accumulation and activation of the renin–angiotensin system.Citation22 These actions manifest as reduced lipid deposition in vessels.Citation23
TZDs may also enhance β-cell function, which has potential implications for maintaining long-term glycemic control in type 2 diabetes.
Altering the natural history of type 2 diabetes – TZDs and durable glycemic control
Type 2 diabetes is a progressive condition characterized by a combination of two fundamental defects: insulin resistance and impaired β-cell function. Insulin resistance in the liver, muscle, and adipose tissue leads to decreased glucose uptake in peripheral tissues, increased hepatic glucose production, and increased lipolysis. Once established, insulin resistance remains fairly constant throughout the natural course of type 2 diabetes; whereas declining β-cell function appears to be the critical factor in the disease’s progression. Early in the natural history of this disease, before the emergence of marked hyperglycemia, increased insulin secretion partially compensates for insulin resistance. Eventually, however, as β-cell function deteriorates, insulin secretion can no longer overcome the metabolic burden posed by insulin resistance, and hyperglycemia results. The presence of dual pathophysiological defects suggests that optimal glucose-lowering therapy for patients with type 2 diabetes should address both sources of metabolic dysregulation.
The primary goal of patient management in diabetes is to achieve and maintain glycemic control. Initially, mono-therapy with oral glucose-lowering agents may be effective, but because diabetes is a progressive disease there is a continual need to reassess and intensify therapy (either through dose increases or additional therapies) in order to maintain glycemic control over the longer term.Citation24,Citation25
Monotherapy
A number of trials have reported the use of TZDs as mono-therapy and have shown significant reductions in the level of glycated hemoglobin (HbA1c) compared with placebo. In randomized, double-blind, placebo-controlled studies with pioglitazone, mean HbA1c reductions ranged from 0.8% (at a 30 mg dose) to 1.6% (with 45 mg).Citation26–Citation28 Similar studies using rosiglitazone showed mean HbA1c reductions ranging from 0.9% (2 mg twice daily) to 1.5% (4 mg twice daily).Citation29,Citation30 A meta-analysis of 23 randomized, placebo-controlled trials comparing monotherapy with pioglitazone or rosiglitazone for 12 to 26 weeks found that each drug similarly reduced HbA1c levels more than placebo, by 1.0% to 1.5%.Citation31
The TZDs have also been shown to be at least as effective as traditional oral glucose-lowering agents (metformin and sulfonylureas) in achieving and maintaining good glycemic control. A comparison of pioglitazone (45 mg) and gliclazide demonstrated an HbA1c reduction of 1.4% for both drugs after 52 weeks of treatment.Citation32 In another study, the effects of pioglitazone and gliclazide were compared for 2 years in 567 patients.Citation33 In patients who had received pioglitazone, the target HbA1c was reached more often (47.8%) than in the patients who had received gliclazide (37.0%).
A comparison of 45 drug-naïve patients randomized to treatment with rosiglitazone (4 mg twice daily), metformin, or placebo showed that both treatments significantly reduced HbA1c after 26 weeks in comparison with placebo.Citation34 Several randomized studies have compared pioglitazone and metformin and showed a comparable reduction in HbA1c.Citation35–Citation39
While a number of studies comparing TZDs with sulfonylureas or metformin have demonstrated similar decreases in HbA1c after 1 year of treatment, the TZDs appear better able to sustain glycemic control in the long term. The A Diabetes Outcome Progression Trial (ADOPT) investigated the durability of the antihyperglycemic effects of rosiglitazone, metformin, and glyburide (or glibencamide [UK]) in 4360 drug-naive patients.Citation40 The 4-year trial found that in the long-term rosiglitazone-treated patients experienced significantly greater durability in terms of reduction of both HbA1c and fasting plasma glucose levels; albeit, the absolute differences in glycemic control between the rosiglitazone and metformin groups were small.
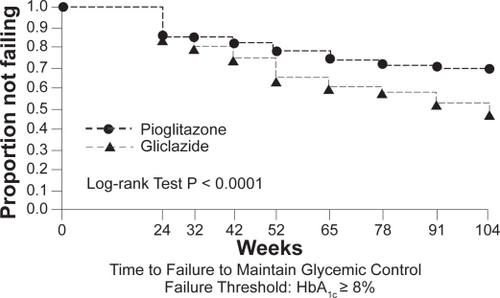
Pioglitazone has also demonstrated sustained glycemic control. Data from a 2-year extension study, in which patients were initially randomized to pioglitazone or gliclazide, have shown that the proportion of patients in the pioglitazone group who maintained HbA1c < 8% at any time during the second year of treatment was higher than that in the gliclazide group ().Citation41,Citation33 This evidence for durability of effect on blood glucose control with the TZDs has been recognized in the recently updated NICE guidelines.Citation42 Declining β-cell function is the predominant reason for deterioration in glucose tolerance. Both rosiglitazone and pioglitazone have been shown to slow the rate of loss of β-cell function and improve insulin sensitivity to a greater extent than other currently used oral agents.Citation5,Citation40 These findings are consistent with a greater durability of glycemic control with the TZDs.
Figure 1 Kaplan–Meier curves showing the proportion of patients in pioglitazone and gliclazide treatment groups not failing (HbA1c <8.0%) at various time points over 2 years. Copyright © 2005 American Diabetes Association. From Diabetes Care®, Vol. 28, 2005;544–550. Reprinted with permission from The American Diabetes Association.
Combination therapy with oral agents
Type 2 diabetes is a chronic disease with a progressive deterioration in glycemic control due to the continuing loss of β-cell function. Monotherapy for type 2 diabetes may therefore not be sufficient to maintain glycemic control over time. Subsequent therapeutic decisions are made principally on the basis of the HbA1c value – a goal of <6.5% is consistent with the most recent recommendations from NICE and the IDF.Citation42,Citation43
Early, aggressive control of glucose levels with combination therapy may be able to slow the decline in glycemic control, compared with monotherapy,Citation44 and reduce the complications of diabetes. To meet the goal of achieving and maintaining glucose levels close to the nondiabetic range, current guidelines and treatment algorithms emphasize initial therapy with lifestyle intervention and metformin and then rapid addition of medications and transition to new regimens when target glycemic goals are not achieved or sustained.Citation42,Citation43,Citation45
When selecting a therapeutic regimen, it is important to consider whether agents address the underlying pathophysiology. The sulfonylureas, metformin, and TZDs act at different sites in the body to improve insulin secretion or to improve insulin action. The sulfonylureas act on the β-cells in the pancreas to stimulate insulin secretion. Metformin is an insulin sensitizer with effects on the liver and muscle. It decreases hepatic glucose production by inhibiting both gluconeogenesis and glycogenolysis, and it also increases the uptake and utilization of glucose by muscle tissue. The TZDs also improve insulin sensitivity by increasing glucose uptake in adipose, liver, and skeletal muscle tissue.
The advantages of combination therapy are that drugs with complementary modes of action can target both the underlying insulin resistance and β-cell dysfunction. For example, although both the TZDs and metformin effectively increase sensitivity to insulin, they have different target organs – metformin exerting most of its glycemic effect by decreasing hepatic glucose production and the TZDs by enhancing insulin sensitivity primarily in muscle and adipose tissue. As a result the two agents have additive effects, and the addition of a TZD to metformin can lower HbA1c by up to 0.8%.Citation46,Citation47
The combination of a sulfonylurea and a TZD is also logical as these agents exert opposing effects on β-cell function. The sulfonylureas focus on stimulating β-cells to secrete more insulin. Over time, studies have shown that chronic exposure to a sulfonylurea can lead to acceleration of β-cell apoptosis, exhaustion, or desensitization.Citation48 The TZDs may attenuate this effect. Although the exact manner in which TZDs achieve this is not entirely understood, possible mechanisms suggested by results from animal studies include direct or indirect reductions in lipotoxicity, prevention of decreases in β-cell mass via an effect on reducing apoptosis and reduced secretory demand, as well as a possible contribution from a reduction in glucotoxicity.Citation49
To determine whether TZD-induced improvement in glycemic control is associated with improved β-cell function, 53 patients with type 2 diabetes were randomized to receive a TZD or placebo for 4 months.Citation50 The study examined insulin secretion during an oral glucose tolerance test while simultaneously taking into account changes in insulin sensitivity. Following 4 months of pioglitazone or rosiglitazone treatment, β-cell glucose sensitivity, ie, the ability of the β-cell to respond to a given change in plasma glucose concentration, improved by ∼2- to 2.8-fold and remained unchanged in the placebo-treated groups.
Further evidence of the positive effects of pioglitazone and rosiglitazone therapy on β-cell function is available from a number of randomized, controlled trials using these agents as monotherapy or in combination with metformin or a sulfonylurea. Rosiglitazone has been shown to restore normal insulin secretion in individuals with impaired glucose toleranceCitation51 and pioglitazone to reduce the development of diabetes in women of Latin American descent with a history of gestational diabetes by improving insulin sensitivity and preventing the progressive deterioration of β-cell function. 52 In the large, randomized ACT NOW study, pioglitazone (up to 45 mg/day) prevented the progression to diabetes in patients with impaired glucose tolerance by 81% compared with placebo at an average 2.6 years of follow-up.Citation53 The rate of progression to diabetes (fasting plasma glucose ≥7.0 mmol/L or higher during follow-up) was 1.5% per year for pioglitazone compared with 6.8% per year for placebo (hazard ratio 0.19, p < 0.00001). Patients treated with pioglitazone were also more likely to return to normal glucose tolerance (42% versus 28% with placebo, p < 0.001). These benefits appeared to be due to a greater improvement in β-cell function with pioglitazone (as demonstrated using a variety of measures). In the Diabetes REduction Assessment with ramipril and rosiglitazone Medication (DREAM) trial, rosiglitazone 8 mg administered daily for 3 years significantly reduced progression to type 2 diabetes (by 60%) and allowed reversion to normoglycemia among a large proportion of adults with impaired fasting glucose, impaired glucose tolerance, or both.Citation54 The ADOPT trial tested the hypothesis that rosiglitazone preserves β-cell function better than other drugs used as first-line therapy for type 2 diabetes, thus delaying or preventing deterioration in glycemic control. The results showed that initial treatment with rosiglitazone slowed the progression to monotherapy failure more effectively than either metformin or glyburide.Citation40 In PROactive, patients randomized to pioglitazone had a reduced need to start taking insulin compared with those on placebo.Citation5
A wealth of short- and long-term studies and literature reviews attest to the fact that the combined use of TZDs with agents such as metformin or sulfonylureas provides better glycemic control compared with further intensifying the metformin or sulfonylurea monotherapy.Citation32,Citation36,Citation38,Citation44,Citation47,Citation48,Citation55–Citation64 A TZD–metformin combination has a powerful effect on reducing insulin resistance and is effective in the early stages of type 2 diabetes when more endogenous insulin is still available. This combination is also associated with minimal hypoglycemia and less weight gain. A sulfonylurea–TZD combination offers the added benefit of lowered insulin resistance and potential improvement in β-cell function. The combination of pioglitazone or rosiglitazone with metformin or with a sulfonylurea has been shown to be an effective alternative to combined metformin and sulfonylurea.Citation38,Citation63,Citation65–Citation68
The observation that early introduction of oral combination therapy is more effective in achieving glycemic control than increasing doses of metformin or sulfonylurea monotherapy has prompted the introduction of fixed-dose single-tablet combinations of TZDs with metformin or a sulfonylurea.
The clinical evidence – impact of TZDs on cardiovascular risk factors and outcomes
Diabetic dyslipidemia, characterized by increased concentrations of triglycerides, reduced concentrations of high-density lipoprotein cholesterol (HDL-C), and increased concentrations of small dense low-density lipoprotein (LDL) particles is a major risk factor for cardiovascular disease. The TZDs appear to improve this atherogenic diabetes lipid profile, and a host of clinical studies have demonstrated improved lipid profiles with pioglitazone and to a lesser extent with rosiglitazone.Citation26,Citation28,Citation39,Citation66,Citation69–Citation72 A large meta-analysis evaluated the effects of rosiglitazone and pioglitazone therapies on diabetic dyslipidemia. Both TZDs significantly raised HDL-C levels.Citation31 Compared with placebo, pioglitazone further improved the lipid profile, significantly lowering triglyceride levels and having a neutral effect on LDL-C and total cholesterol levels. In contrast, rosiglitazone was found to increase LDL-C and total cholesterol levels and to demonstrate a neutral effect on triglyceride levels. The results of the meta-analysis suggest that pioglitazone produces a more favorable lipid profile. More recent head-to-head comparisons of the two agents have confirmed these findings.Citation73,Citation74 In the study of Goldberg et al a total of 802 subjects were randomized to blinded treatment with maximal dose of either pioglitazone or rosiglitazone to determine the effect of these agents on fasting lipids in the setting of no other glucose or lipid-lowering therapy.Citation73 The observed changes in lipid concentrations are shown in . A significant difference in favor of pioglitazone over rosiglitazone was noted for HDL-C, triglycerides, LDL particle size, and LDL particle concentration.Citation73 Furthermore, in an open-label study, patients with type 2 diabetes demonstrated marked improvements in lipid profiles along with stable glycemic control after treatment conversion from rosiglitazone to pioglitazone while maintaining stable statin therapy.Citation72 In addition, pioglitazone but not rosiglitazone therapy significantly increased LDL-C particle size to large, less-atherogenic particles.Citation39,Citation72,Citation75–Citation77
Table 1 In the study of Goldberg et al a total of 802 subjects were randomized to blinded treatment with maximal dose of either pioglitazone or rosiglitazone to determine the effect of these agents on fasting lipids in the setting of no other glucose or lipid-lowering therapy. The observed changes in lipid concentrations from baseline are shownCitation73
The TZDs have demonstrated favorable effects on other surrogate markers of cardiovascular disease. Adipose tissue produces substantial amounts of plasminogen activator inhibitor type-1 (PAI-1) – this when increased is an established cardiovascular risk factor. Both rosiglitazone and pioglitazone have been shown to reduce levels of PAI-1.Citation78,Citation79 Similarly, both agents have demonstrated significantly greater anti-inflammatory and antiatherogenic effects, compared with control agents, including reductions in C-reactive protein and matrix metalloproteinase-9Citation79,Citation80 and increases in adiponectin levels.Citation80,Citation81 Carotid intima-media thickness (CIMT) is a marker of coronary atheroscelerosis and independently predicts subsequent cardiovascular events. Two studies of pioglitazone versus glimepiride have demonstrated beneficial effects on CIMT. In a 24-week study, a significant reduction in CIMT was observed with pioglitazone,Citation80 while the CHI-CAGO (Carotid intima-media tHICkness in Atherosclerosis using pioGlitazOne) trial demonstrated that pioglitazone significantly slowed progression of CIMT compared with glimepiride over an 18-month period.Citation82
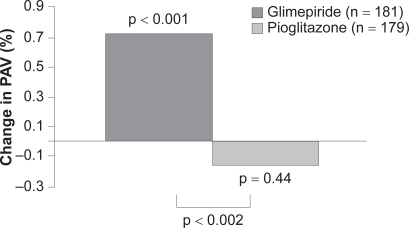
In addition to favorable effects on surrogate markers of cardiovascular disease, recently published data from the PERISCOPE trial demonstrate a significant effect of pioglitazone on atheroma volume.Citation83 In patients with type 2 diabetes undergoing angiography for clinical indications, baseline intravascular ultrasound (IVUS) was performed to determine atheroma volume. A total of 543 patients were then randomized to pioglitazone 15 to 45 mg or glimepiride 1 to 4 mg titrated to maximally tolerated dose by 16 weeks. After 18 months, IVUS of the originally examined coronary artery was performed in 360 participants and revealed that pioglitazone had prevented the progression of coronary atherosclerosis compared with glimepiride ().
Figure 2 In patients with type 2 diabetes and coronary artery disease, treatment with pioglitazone resulted in a significantly lower rate of progression of coronary atherosclerosis compared with glimepiride. Developed from data of Nissen et al 2008.Citation83
Improved glycemic control is linked to better clinical outcomes in diabetes. In addition, the TZDs have beneficial effects on a number of cardiovascular risk markers. However, few studies have compared outcomes for glucose-lowering medications beyond their glucose-lowering efficacy.
PROactive is the only large treatment trial to date designed a priori to examine cardiovascular endpoints in TZD-treated patients. In this trial, a total of 5238 patients with type 2 diabetes and macrovascular disease were randomized to receive either pioglitazone (15 to 45 mg daily) or placebo while continuing existing therapy with glucose-lowering agents, lipid-lowering medications, and antihypertensives.Citation5 The primary endpoint, which was a composite of all-cause mortality, nonfatal myocardial infarction (including silent infarction), stroke, acute coronary syndrome, endovascular or surgical intervention in the coronary or leg arteries, and amputation above the ankle, did not reach statistical significance. This composite endpoint was challenging, however; it included procedural endpoints and was designed to demonstrate benefit in multiple vascular beds – cardiac, cerebral, and peripheral. Pioglitazone was associated with a statistically significant 16% reduction in the occurrence of the predetermined principal secondary endpoint (composite of all-cause mortality, nonfatal myocardial infarction, and stroke). This endpoint is identical or similar to primary composite endpoints used in many other major cardiovascular outcome studies.
In a prespecified subgroup analysis, the PROactive investigators looked at stroke endpoints in patients with (n = 984) and without (n = 4254) a prior history of stroke.Citation85 Recurrent stroke was reduced by 47% in patients with a prior history of stroke who received pioglitazone compared with those administered placebo (hazard ratio 0.53; 95% CI 0.34–0.85, p = 0.008). Similarly, in the subgroup of patients who had a previous myocardial infarction (n = 2445), pioglitazone had a statistically significant beneficial effect on the prespecified endpoints of fatal and nonfatal myocardial infarction (28% risk reduction; p = 0.045) and acute coronary syndrome (37% risk reduction; p = 0.035).Citation86 As in other TZD trials, pioglitazone was associated with greater weight gain and with increased rates of edema and heart failure compared with placebo-treated patients, although mortality due to heart failure did not differ between the groups.Citation86 Less robust data in the form of a meta-analysis of noncardiovascular endpoint trials, which included 16,390 patients in 19 studies, provide further support for pioglitazone’s cardiovascular safety.Citation87
The evidence base for rosiglitazone is less extensive, with no completed cardiovascular outcomes trials. Contrary to findings with pioglitazone, a recent meta-analysis of noncardiovascular endpoint trials has suggested that rosiglitazone may be associated with an increased risk of cardiovascular events in patients with type 2 diabetes.Citation88 The findings warrant further investigation, however. In the individual large published trials included in the study (specifically DREAM and ADOPT), there were no increases in the rates of myocardial ischemia or cardiovascular death. The findings have also not been confirmed by randomized prospective trials (including the interim analysis of the RECORD trial).Citation58 Rosiglitazone was also widely prescribed in two large cardiovascular outcomes trials comparing intensive and standard glucose-lowering targets in type 2 diabetes that have been published since the meta-analysis.Citation89,Citation90 While these trials were assessing a treatment strategy and not any specific drug, no evidence that rosiglitazone is associated with excess cardiovascular events was found.
Other large cardiovascular outcomes trials with rosiglitazone, such as BARI 2D, will provide further information on the cardiovascular safety profile of rosiglitazone. However, based on available data, the US Food and Drug Administration has concluded that the use of rosiglitazone for the treatment of type 2 diabetes may be associated with a greater risk of myocardial ischemic events than placebo, metformin, or sulfonylureas. The agency has added label warnings to the prescribing information until the results of long-term cardiovascular outcome trials for rosiglitazone become available.
Safety aspects of TZDs
Weight gain is a class effect of the TZDs either as mono-therapy or in combination with other glucose-lowering agents. Most studies report an average weight gain of 3 to 4 kg over the first 6 months of TZD treatment, in line with the weight gain observed with sulfonylureas and insulin. Weight gain associated with TZDs may vary greatly depending on the individual and on the treatment regimen employed. In particular, weight gain is more pronounced when TZDs are combined with sulfonylureas or insulin.Citation70,Citation91
The most important side effects of the TZDs are fluid retention (usually manifest as peripheral edema) and an increase in subcutaneous fat, which both contribute to weight gain. The individual contributions of excess fluid and subcutaneous fat to TZD-associated weight gain have not been confirmed, although one study suggests that fluid accounts for as much as 75% of body weight increase.Citation92 Other studies, however, have estimated fat to have the greater contribution.Citation93 The likelihood of edema increases when TZDs are used in combination with insulin – patients using this combination should be monitored carefully. TZD-induced fluid retention may cause or aggravate diabetic macular edema by increasing plasma volume and vascular permeability.Citation94,Citation95 In addition, as edema can be associated with new or worsened heart failure, these agents should be used with caution in patients with edema or a history of heart failure. Four recent large-scale outcomes studies have shown an increased risk of non-fatal heart failure versus comparator drugs or placebo.Citation5,Citation40,Citation54,Citation58 In the US, initiation of rosiglitazone and pioglitazone is contraindicated in patients with established New York Heart Association Class III or IV heart failure and both TZDs carry a box warning for congestive heart failure, which is entirely separate from the recent concerns over the increased myocardial ischemia risk associated with rosiglitazone. In Europe, heart failure at any stage is a contraindication to the use of TZDs.
Although the underlying mechanisms of TZD-induced edema remain unclear, in vitro and animal data suggest that PPAR-γ agonists stimulate sodium reabsorption in the distal nephron by upregulating the expression and the translocation of the collecting duct epithelial sodium channel. Preliminary evidence suggests that diuretic agents, such as spironolactone and hydrochlorothiazide, which interfere with the signaling of PPAR-γ in the renal distal collecting duct, may be an effective means of reversing TZD-induced fluid retention.Citation96
Both TZDs have been associated with reductions in markers of bone formation and reductions in bone mineral density.Citation97–Citation99 Preliminary analyses of the ADOPT trial revealed a small but significant number of leg and forearm fractures in postmenopausal women with rosiglitazone.Citation40 A similar finding has been reported for pioglitazone in an analysis carried out using the manufacturer’s clinical trial database.Citation100 An observational study has also reported increased bone loss with TZD use in 160 older diabetic men,Citation101 although the study did not have sufficient power to control for potential confounders such as HbA1c level, use of other medications, or diabetic complications. With both agents, the majority of fractures observed were in the upper arm (humerus), hand, or foot. These sites of fracture are different from those associated with postmenopausal osteoporosis (eg, hip or spine). None of the studies were designed to study the effect of TZDs on bone and therefore multiple known risk factors for fractures cannot be excluded as confounding variables. However, as it is known that PPAR-γ activation may influence bone metabolism (for a review see Lau and Harper 2007Citation102), future research should include a randomized, controlled trial in which fracture incidence and type of fracture are prospective outcome measures. Manufacturers have advised practitioners to consider the risk of fracture when initiating or treating female patients with type 2 diabetes using TZD-containing products.
The first available medication in the TZD class, troglitazone, was withdrawn from the market due to severe liver toxicity. Pioglitazone and rosiglitazone have not been associated with severe liver toxicity either as monotherapy or with oral antidiabetic agent or insulin combinations; however, it is recommended that liver enzymes are checked before initiating therapy in all patients and are monitored periodically thereafter based on clinical judgment. Both TZDs are contraindicated for use in patients with hepatic impairment.
Conclusions
A wealth of clinical data attest to the efficacy of pioglitazone and rosiglitazone mono- and combination therapies in achieving and sustaining glycemic control, both in patients with newly diagnosed disease and in those with more advanced disease who are not well controlled on other therapies. Conventional glucose-lowering agents such as sulfonylureas or metformin are often unable to maintain durable glycemic control when used as monotherapy. As agents that can preserve β-cell function and reduce insulin resistance either as monotherapy or in combination, the TZDs address fundamental mechanisms in the development and progression of type 2 diabetes, and complement existing treatments. Current data also hold the promise that early therapy with TZDs may decrease cardiovascular risk independently of glycemic control. Pioglitazone and (to a lesser extent) rosiglitazone have demonstrated favorable effects on surrogate markers of cardiovascular disease such as lipid profiles, inflammatory markers, and CIMT, and recently published data for pioglitazone also demonstrate a significant reduction in atheroma volume.Citation83 Documented evidence for a benefit on cardiovascular outcomes has been demonstrated only with pioglitazone,Citation5 but a number of trials are being conducted to address the effect of TZDs on cardiovascular outcomes – specifically, prevention of macrovascular complications. The UKPDS showed that the lower the HbA1c level the lower the risk for long-term complications.Citation103 Therefore attaining and maintaining HbA1c treatment goals is critical in the management of type 2 diabetes.
Although generally well tolerated, TZDs can cause weight gain and induce fluid retention that occasionally leads to a diagnosis of heart failure (in susceptible individuals) and may contribute to bone loss in a small number of postmenopausal women. Concerns over heart failure risks associated with TZDs in general are entirely separate from the concerns over the increased myocardial ischemia risk associated with rosiglitazone. To date, increased risk of cardiac ischemia has not been reported with pioglitazone. While the ADA and EASD urge greater caution in the use of TZDs, particularly in patients with heart failure, in the latest update to their diabetes treatment guidelines, pioglitazone remains a possible choice for a second-line agent in patients who do not achieve HbAlc levels below 7% with lifestyle modification and metformin.Citation104 Overall, the place of TZDs in the management of type 2 diabetes is well established and the potential for additional benefits on macrovascular risk beyond glucose-lowering efficacy continue to encourage further study of the long-term effects of these agents.
Disclosures
Professor Barnett has received research funding and honoraria for advisory work and lectures from relevant companies, including Takeda, GSK, Servier, MSD and Novartis.
References
- Department of HealthForecasting obesity to 2010Department of Health82006Available from: http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsStatistics/DH_4138630 (accessed 17 October 2008).
- AmosAFMcCartyDJZimmetPThe rising global burden of diabetes and its complications: estimates and projections to the year 2010Diabet Med199714S1S859450510
- FordESPrevalence of the metabolic syndrome defined by the International Diabetes Federation among adults in the USDiabetes Care2005282745274916249550
- Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in AdultsExecutive summary of the third report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III)JAMA20012852486249711368702
- DormandyJACharbonnelBEcklandDJSecondary prevention of macrovascular events in patients with type 2 diabetes in the PROactive Study (PROspective pioglitAzone Clinical Trial In macroVascular Events): a randomised controlled trialLancet20053661279128916214598
- BloomgardenZTThe Avandia debateDiabetes Care2007302401240817726191
- WeyerCTataranniPABogardusCPratleyREInsulin resistance and insulin secretory dysfunction are independent predictors of worsening of glucose tolerance during each stage of type 2 diabetes developmentDiabetes Care200124899411194248
- KahnSEThe importance of the β-cell in the pathogenesis of type 2 diabetes mellitusAm J Med2000108Suppl 6a2S8S10764844
- DeFronzoRA1988 Lilly Lecture The triumvirate: beta-cell, muscle, liver. A collusion responsible for NIDDMDiabetes1987376676873289989
- BergmanRNAderMHueckingKVan CittersGAccurate assessment of β-cell function: the hyperbolic correctionDiabetes200251Suppl 1S212S22011815482
- UK Prospective Diabetes Study (UKPDS) GroupIntensive blood-glucose control with sulfonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33)Lancet19983528378539742976
- UK Prospective Diabetes Study (UKPDS) GroupUKPDS 16. Overview of 6 years’ therapy of type II diabetes: a progressive diseaseDiabetes199544124912587589820
- NestoRWThe relation of insulin resistance syndromes to risk of cardiovascular diseaseRev Cardiovasc Med20034Suppl 6S111814668699
- SmileyTOhPShaneLGThe relationship of insulin resistance measured by reliable indexes to coronary artery disease risk factors and outcomes–a systematic reviewCan J Cardiol20011779780511468646
- BonoraEFormentiniGCalcaterraFHOMA-estimated insulin resistance is an independent predictor of cardiovascular disease in type 2 diabetic subjects: prospective data from the Verona Diabetes Complications StudyDiabetes Care2002251135114112087010
- TontonozPSpiegelmanBMFat and beyond: the diverse biology of PPAR-γAnn Rev Biochem20087728931218518822
- RavnskjærKBørgesenMRubiBPeroxisome proliferator-activated receptor alpha (PPARalpha) potentiates, whereas PPARgamma attenuates, glucose-stimulated insulin secretion in pancreatic beta-cellsEndocrinology20051463266327615878969
- SmithSAPeroxisome proliferator-activated receptors and the regulation of mammalian lipid metabolismBiochem Soc Trans200230(Pt 6):1086109012440979
- OlefskyJMSaltielARPPAR gamma and the treatment of insulin resistanceTrends Endocrinol Metab20001136236811042466
- FonsecaVARationale for the use of insulin sensitizers to prevent cardiovascular events in type 2 diabetes mellitusAm J Med20071209 Suppl 2S18S2517826042
- LeiterLACan thiazolidinediones delay disease progression in type 2 diabetes?Curr Med Res Opin2006221193120116846552
- CalkinACThomasMCPPAR agonists and cardiovascular disease in diabetesPPAR Res2008245410.
- PatelCBDe LemosJAWyneKLMcGuireDKThiazolidinediones and risk for atherosclerosis: pleiotropic effects of PPARγ agonismDiabetes Vasc Dis Res200636571
- TurnerRCCullCAFrighiVHolmanRGlycemic control with diet, sulfonylurea, metformin, or insulin in patients with type 2 diabetes mellitus: progressive requirement for multiple therapies (UKPDS 49)JAMA19992812005201210359389
- CookMNGirmanCJSteinPPAlexanderCMHolmanRRGlycemic control continues to deteriorate after sulfonylureas are added to metformin among patients with type 2 diabetesDiabetes Care200528995100015855556
- AronoffSRosenblattSBraithwaiteSEganJWMathisenALSchneiderRLPioglitazone hydrochloride monotherapy improves glycemic control in the treatment of patients with type 2 diabetes: a 6-month randomized placebo-controlled dose-response study. The Pioglitazone 001 Study GroupDiabetes Care2000231605161111092281
- ScherbaumWAGokeBMetabolic efficacy and safety of once-daily pioglitazone monotherapy in patients with type 2 diabetes: a double-blind, placebo-controlled studyHorm Metab Res20023458959512439788
- HerzMJohnsDReviriegoJA randomized, double-blind, placebo-controlled, clinical trial of the effects of pioglitazone on glycemic control and dyslipidemia in oral antihyperglycemic medication-naive patients with type 2 diabetes mellitusClin Ther2003251074109512809958
- LebovitzHEDoleJFPatwardhanRRappaportEBFreedMIfor the Rosiglitazone Clinical Trials Study GroupRosiglitazone monotherapy is effective in patients with type 2 diabetesJ Clin Endocrinol Metab20018628028811232013
- PhillipsLSGrunbergerGMillerEfor the Rosiglitazone Clinical Trials Study GroupOnce- and twice-daily dosing with rosiglitazone improves glycemic control in patients with type 2 diabetesDiabetes Care20012430831511213884
- ChiquetteERamirezGDeFronzoRA meta-analysis comparing the effect of thiazolidinediones on cardiovascular risk factorsArch Intern Med20041642097210415505122
- CharbonnelBHMatthewsDRSchernthanerGHanefeldMBrunettiPfor The QUARTET Study GroupA long-term comparison of pioglitazone and gliclazide in patients with type 2 diabetes mellitus: a randomized, double-blind, parallel-group comparison trialDiabet Med20052239940515787663
- TanMHBaksiAKrahulecBfor the GLAL Study GroupComparison of pioglitazone and gliclazide in sustaining glycemic control over 2 years in patients with type 2 diabetesDiabetes Care20052854455015735185
- HällstenKVirtanenKALönnqvistFRosiglitazone but not metformin enhances insulin- and exercise-stimulated skeletal muscle glucose uptake in patients with newly diagnosed type 2 diabetesDiabetes2002513479348512453903
- PavoIJermendyGVarkonyiTTEffect of pioglitazone compared with metformin on glycemic control and indicators of insulin sensitivity in recently diagnosed patients with type 2 diabetesJ Clin Endocrinol Metab2003881637164512679450
- HanefeldMBrunettiPSchernthanerGHMatthewsDRCharbonnelBHfor the QUARTET Study GroupOne-year glycemic control with a sulfonylurea plus pioglitazone versus a sulfonylurea plus metformin in patients with type 2 diabetesDiabetes Care20042714114714693980
- NagasakaSAisoYYoshizawaKIshibashiSComparison of pioglitazone and metformin efficacy using homeostasis model assessmentDiabet Med20042113614114984448
- CharbonnelBSchernthanerGBrunettiPLong-term efficacy and tolerability of add-on pioglitazone therapy to failing monotherapy compared with addition of gliclazide or metformin in patients with type 2 diabetesDiabetologia2005481093110415889234
- SchernthanerGMatthewsDRCharbonnelBHanefeldMBrunettiPfor the QUARTET Study GroupEfficacy and safety of pioglitazone versus metformin in patients with type 2 diabetes mellitus: a double-blind, randomized trialJ Clin Endocrinol Metab2004896068607615579760
- KahnSEHaffnerSMHeiseMAfor the ADOPT Study GroupGlycemic durability of rosiglitazone, metformin, or glyburide mono-therapyN Engl J Med20063552427244317145742
- TanMHJohnsDStrandJfor the GLAC Study GroupSustained effects of pioglitazone vs glibenclamide on insulin sensitivity, glycaemic control, and lipid profiles in patients with Type 2 diabetesDiabet Med20042185986615270789
- National Institute for Health and Clinical Excellence (NICE)Type 2 diabetes: the management of type 2 diabetes (update) Available from: http://www.nice.org.uk/CG66 (accessed 17 October 2008).
- IDF Clinical Guidelines Task ForceGlobal guideline for type 2 diabetes: recommendations for standard, comprehensive, and minimal careDiabet Med20062357959316759299
- RosenstockJRoodJCobitzABiswasNChouHGarberAInitial treatment with rosiglitazone/metformin fixed-dose combination therapy compared with monotherapy with either rosiglitazone or metformin in patients with uncontrolled type 2 diabetesDiabetes Obes Metab2006865066017026489
- NathanDMBuseJBDavidsonMBManagement of hyperglycaemia in type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapyDiabetologia2006491711172116802130
- FonsecaVRosenstockJPatwardhanRSalzmanAEffect of metformin and rosiglitazone combination therapy in patients with type 2 diabetes mellitusJAMA20002831695170210755495
- BaileyCJBagdonasARubesJRosiglitazone/metformin fixed dose combination compared with uptitrated metformin alone in type 2 diabetes mellitus: a 24 week, multicenter, randomized, double blind, parallel group studyClin Ther2005271548156116330291
- HanefeldMPioglitazone and sulfonylureas: effectively treating type 2 diabetesInt J Clin Pract2007S1532027
- SmileyTThe role of declining beta cell function in the progression of type 2 diabetes: implications for outcomes and pharmacological managementCan J Diabetes200327277286
- GastaldelliAFerranniniEMiyazakiYMatsudaMMariADefronzoRAThiazolidinediones improve beta-cell function in type 2 diabetic patientsAm J Physiol Endocrinol Metab2007292E871E88317106061
- JuhlCBHollingdalMPørksenNPrangeALönnqvistFSchmitzOInfluence of rosiglitizone treatment on β-cell function in type 2 diabetes: evidence of an increased ability of glucose to entrain high-frequency insulin pulsatilityJ Clin Endocrinol Metab2003883794380012915671
- XiangAPetersRKjosSEffect of pioglitizone on pancreatic β-cell function and diabetes risk in Hispanic women with gestational diabetesDiabetes2006555172216443789
- TripathyDBanerjiMABrayGAACTos NOW for the Prevention of Diabetes (ACT NOW) Study [Abstract]Diabetologia200851Suppl 1S99
- DREAM (Diabetes REduction Assessment with ramipril and rosiglitazone Medication) Trial InvestigatorsEffect of rosiglitazone on the frequency of diabetes in patients with impaired glucose tolerance or impaired fasting glucose: a randomised controlled trialLancet20063681096110516997664
- GarberAKleinEBruceSSankohSMohideenPMetformin–glibenclamide versus metformin plus rosiglitazone in patients with type 2 diabetes inadequately controlled on metformin monotherapyDiabetes Obes Metab2006815616316448519
- HamannAGarcia-PuigJPaulGDonaldsonJStewartMComparison of fixed-dose rosiglitazone/metformin combination therapy with sulfonylurea plus metformin in overweight individuals with type 2 diabetes inadequately controlled on metformin aloneExp Clin Endocrinol Diabetes200811661318095238
- StewartMWCirkelDTFurusethKEffect of metformin plus roziglitazone compared with metformin alone on glycaemic control in well-controlled Type 2 diabetesDiabet Med2006231069107816978370
- HomePDPocockSJBeck-NielsenHfor the RECORD Study GroupRosiglitazone evaluated for cardiovascular outcomes–an interim analysisN Engl J Med2007357283817551159
- DorkhanMFridAA review of pioglitazone HCL and glimepiride in the treatment of type 2 diabetesVasc Health Risk Manag2007372173118078023
- DerosaGPioglitazone plus glimepiride: a promising alternative in metabolic controlInt J Clin Pract2007S1532836
- StaelsBMetformin and pioglitazone: Effectively treating insulin resistanceCurr Med Res Opin200622Suppl 2S27S3716914073
- SeufertJA fixed-dose combination of pioglitazone and metformin: a promising alternative in metabolic controlCurr Med Res Opin200622Suppl 2S39S4816914074
- MatthewsDRCharbonnelBHHanefeldMBrunettiPSchernthanerGLong-term therapy with addition of pioglitazone to metformin compared with the addition of gliclazide to metformin in patients with type 2 diabetes: a randomized, comparative studyDiabetes Metab Res Rev20052116717415386821
- KerenyiZSamerHJamesRYanYStewartMCombination therapy with rosiglitazone and glibenclamide compared with upward titration of glibenclamide alone in patients with type 2 diabetes mellitusDiabetes Res Clin Pract20046321322314757293
- ComaschiMDemicheliADi PietroCBellatrecciaAMarizSfor the COM06 Study InvestigatorsEffects of pioglitazone in combination with metformin or a sulfonylurea compared to a fixed-dose combination of metformin and glibenclamide in patients with type 2 diabetesDiabetes Technol Ther2007938739817705695
- BetteridgeDJVergesBLong-term effects on lipids and lipoproteins of pioglitazone versus gliclazide addition to metformin and pioglitazone versus metformin addition to sulfonylurea in the treatment of type 2 diabetesDiabetologia2005482477248116283239
- DerosaGCiceroAFGaddiAA comparison of the effects of pioglitazone and rosiglitazone combined with glimepiride on prothrombotic state in type 2 diabetic patients with the metabolic syndromeDiabetes Res Clin Pract20056951315955382
- DerosaGGaddiAVPiccinniMNDifferential effect of glimepiride and rosiglitazone on metabolic control of type 2 diabetic patients treated with metformin: a randomized, double-blind, clinical trialDiabetes Obes Metab2006819720516448524
- EinhornDRendellMRosenzweigJEganJWMathisenALSchneiderRLPioglitazone hydrochloride in combination with metformin in the treatment of type 2 diabetes mellitus: a randomized, placebo-controlled study. The Pioglitazone 027 Study GroupClin Ther2000221395140911192132
- RosenblattSMiskinBGlazerNBPrinceMJRobertsonKEThe impact of pioglitazone on glycemic control and atherogenic dyslipidemia in patients with type 2 diabetes mellitusCoron Artery Dis20011241342311491207
- MattooVEcklandDWidelMMetabolic effects of pioglitazone in combination with insulin in patients with type 2 diabetes mellitus whose disease is not adequately controlled with insulin therapy: results of a six-month, randomized, double-blind, prospective, multicenter, parallel-group studyClin Ther20052755456715978304
- BerhanuPKipnesMSKhanMAEffects of pioglitazone on lipid and lipoprotein profiles in patients with type 2 diabetes and dyslipidaemia after treatment conversion from rosiglitazone while continuing stable statin therapyDiab Vasc Dis Res20063394416784180
- GoldbergRBKendallDMDeegMAA comparison of lipid and glycemic effects of pioglitazone and rosiglitazone in patients with type 2 diabetes and dyslipidemiaDiabetes Care2005281547155415983299
- DerosaGD’AngeloARagonesiPDMetformin–pioglitazone and metformin–rosiglitazone effects on non-conventional cardiovascular risk factors plasma level in type 2 diabetic patients with metabolic syndromeJ Clin Pharm Ther20063137538316882108
- DeegMABuseJBGoldbergRBfor the GLAI Study InvestigatorsPioglitazone and rosiglitazone have different effects on serum lipoprotein particle concentrations and sizes in patients with type 2 diabetes and dyslipidemiaDiabetes Care2007302458246417595355
- LawrenceJMReidJTaylorGJStirlingCRecklessJPFavorable effects of pioglitazone and metformin compared with gliclazide on lipoprotein subfractions in overweight patients with early type 2 diabetesDiabetes Care200427414614693964
- PerezAKhanMJohnsonTKarunaratneMPioglitazone plus a sulfonylurea or metformin is associated with increased lipoprotein particle size in patients with type 2 diabetesDiabetes Vasc Dis Res200414450
- DerosaGD’AngeloARagnonesiPDEffects of rosiglitazone and pioglitazone combined with metformin on the prothrombotic state of patients with type 2 diabetes mellitus and metabolic syndromeJ Int Med Res20063454555517133785
- GoldsteinBJWeissmanPNWooddellMJWaterhouseBRCobitzARReductions in biomarkers of cardiovascular risk in type 2 diabetes with rosiglitazone added to metformin compared with dose escalation of metformin: an EMPIRE trial sub-studyCurr Med Res Opin2006221715172316968575
- PfutznerAMarxNLubbenGImprovement of cardiovascular risk markers by pioglitazone is independent from glycemic control: results from the PIONEER studyJ Am Coll Cardiol2005451925193115963388
- YangWSJengCYWuTYSynthetic peroxisome proliferator-activated receptor-γ agonist, rosiglitazone, increases plasma levels of adiponectin type 2 diabetic patientsDiabetes Care20022537638011815513
- MazzoneTMeyerPMFeinsteinSBEffect of pioglitazone compared with glimepiride on carotid intima-media thickness in type 2 diabetes: a randomized trialJAMA20062962572258117101640
- NissenSENichollsSJWolskiKComparison of pioglitazone vs glimepiride on progression of coronary atherosclerosis in patients with type 2 diabetes: the PERISCOPE randomized controlled trialJAMA20082991561157318378631
- UK Prospective Diabetes Study (UKPDS) GroupEffect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34)Lancet19983528548659742977
- WilcoxRBousserM-GBetteridgeDJfor the PROactive InvestigatorsEffects of pioglitazone in patients with type 2 diabetes with or without previous stroke: results from PROactive (PROspective pioglitAzone Clinical Trial In macroVascular Events 04)Stroke20073886587317290029
- ErdmannEDormandyJACharbonnelBMassi-BenedettiMMoulesIKSkeneAMfor the PROactive InvestigatorsThe effect of pioglitazone on recurrent myocardial infarction in 2,445 patients with type 2 diabetes and previous myocardial infarction. Results from the PROactive (PROactive 05) studyJ Am Coll Cardiol2007491772178017466227
- LincoffAMWolskiKNichollsSJNissenSEPioglitazone and risk of cardiovascular events in patients with type 2 diabetes mellitus: a meta-analysis of randomized trialsJAMA20072981180118817848652
- NissenSEWolskiKEffect of rosiglitazone on the risk of myocardial infarction and death from cardiovascular causesN Engl J Med20073562457247117517853
- Action to Control Cardiovascular Risk in Diabetes Study GroupGersteinHCMillerMEByingtonRPGoffDCJrBiggerJTEffects of intensive glucose lowering in type 2 diabetesN Engl J Med20083582545255918539917
- DuckworthWCAmerican Diabetes Association 68th Scientific Sessions: VA Diabetes Trial SymposiumPresented 682008
- RaskinPRendellMRiddleMCDoleJFFreedMIRosenstockJfor the Rosiglitazone Clinical Trials Study GroupA randomized trial of rosiglitazone therapy in patients with inadequately controlled insulin-treated type 2 diabetesDiabetes Care2001241226123211423507
- BasuAJensenMDMcCannFMukhopadhyayDJoynerMJRizzaRAEffects of pioglitazone versus glipizide on body fat distribution, body water content, and hemodynamics in type 2 diabetesDiabetes Care2006951051416505497
- BaysHMandarinoLDeFronzoRARole of the adipocyte, free fatty acids, and ectopic fat in pathogenesis of type diabetes mellitus: peroxisomal proliferator-activated receptor agonists provide a rational therapeutic approachJ Clin Endocrinol Metab20048946347814764748
- RyanMacular Edema associated with glitazoneRetina20062656257016770264
- LiazosSpontaneous resolution of diabetic macular edema after discontinuation of thizolidinedionesDiabet Med20082586086218644073
- KarallieddeJBuckinghamRStarkieMLorandDStewartMVibertiGfor the Rosiglitazone Fluid Retention Study GroupEffect of various diuretic treatments on rosiglitazone-induced fluid retentionJ Am Soc Nephrol2006173482349017093067
- GreyABollandMGambleGThe peroxisome proliferator-activated receptor-γ agonist rosiglitazone decreases bone formation and bone mineral density in healthy postmenopausal women: a randomized, controlled trialJ Clin Endocrinol Metab2007921305131017264176
- BerberogluZGursoyABayraktarNYaziciACBascil TutuncuNGuvener DemiragNRosiglitazone decreases serum bone-specific alkaline phosphatase activity in postmenopausal diabetic womenJ Clin Endocrinol Metab2007923523353017595249
- GlintborgDAndersenMHagenCHeickendorffLHermannAPAssociation of pioglitazone treatment with decreased bone mineral density in obese premenopausal patients with polycystic ovary syndrome: a randomized, placebo-controlled trialJ Clin Endocrinol Metab2008931696170118285411
- MeymehRHWooltortonEDiabetes drug pioglitazone (Actos): risk of fractureCMAJ200717772372417823139
- YaturuSBryantBJainSKThiazolidinediones treatment decreases bone mineral density in type 2 diabetic menDiabetes Care2007301574157617363747
- LauAHarperWThiazolidinediones and their effect on bone metabolism: a reviewCan J Diabetes200731378383
- StrattonIMAdlerAINeilHAAssociation of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational studyBMJ200032140541210938048
- NathanDMBuseJBDavidsonMBFerranniniEHolmanRRSherwinRZinmanBMedical management of hyperglycaemia in type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapy. A consensus statement of the American Diabetes Association and the European Association for the Study of DiabetesDiabetes Care200932111