Abstract
Pitavastatin is a potent HMG-CoA reductase inhibitor and efficient hepatocyte low-density lipoprotein cholesterol (LDL-C) receptor inducer, producing robust reduction of the serum LDL-C levels, even at a low dose. Pitavastatin and its lactone form are minimally metabolized by CYP enzymes, and are therefore associated with minimal drug–drug interactions (DDIs). Pitavastatin 2 to 4 mg has potent LDL-C-reducing activity, equivalent to that of atorvastatin 10 to 20 mg; several clinical trials have revealed consistently superior high-density lipoprotein cholesterol (HDL-C) elevating activity of pitavastatin than that of atorvastatin. Pitavastatin-induced HDL-C elevation has been shown to be sustained, even incremental, in long-term clinical trials. Pitavastatin was as well-tolerated as atorvastatin or simvastatin in double-blind randomized clinical trials. Two-year long-term safety and effectiveness of pitavastain has been confirmed in a large-scale, prospective post-marketing surveillance. The safety and efficacy profile of pitavastatin is favorable for the treatment of dyslipidemia, especially in metabolic syndrome patients. In addition to control of LDL-C, adequate control of triglyceride (TG) and HDL-C, hypertension and hyperglycemia is also necessary in metabolic syndrome patients. Pitavastatin produces adequate control of LDL-C and TG, along with potent and incremental HDL-C elevation, with a low frequency of DDIs.
Introduction
Low-density lipoprotein cholesterol (LDL-C) is an established risk factor for atherosclerotic disease, especially coronary artery disease (CAD), therefore, management of serum LDL-C levels is evidently the most important goal in the treatment of dyslipidemia.Citation1–Citation3 Several large-scale studies on primary and secondary prevention of coronary heart disease (CHD) conducted using 3-hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) reductase inhibitors (statins) have reported that the LDL-C-lowering statin therapy markedly reduced the incidence of CAD.Citation4 These results provide the rationale for wider use of statins in CHD treatment. A recent meta-analysis of 10 representative trials reported that treatment with statins for primary prevention reduced the risk of major coronary events by 30%, and that the treatment effect was noted even in clinical subgroups for which inconsistent results on efficacy have been reported, including older people, women, and patients with diabetes mellitus.Citation5 While the statins have been proven to be definitely efficacious in CHD prevention, the percentage of patients in whom the LDL-C treatment goal recommended in the National Cholesterol Education Program (NCEP)-Adult Treatment Panel (ATP) III in the US in 2003 is achieved by statin therapy alone is unsatisfactory: 55% in patients with diabetes mellitus, 40% in those with other CAD risk equivalents, and 62% in those with CHD.Citation6 Similarly, the rate of achievement by risk category of the LDL-C treatment goals as reported in the 2002 report of the Japan Atherosclerosis Society guidelines in 2003, is also unsatisfactory: 51% in patients with category B3, 54% in those with B4, and 31% in those with C.Citation7 Therefore, although strong statins such as atorvastatin, pitavastatin, and rosuvastatin are available for the treatment of dyslipidemia in routine clinical practice, use of these drugs at conventional doses may be unsatisfactory for LDL-C management in patients, including those with diabetes mellitus, other CHD risk equivalents, and CHD. For such patients, administration of statins at high doses or concomitant use of other agents for dyslipidemia should be considered. However, administration of statins at high doses may increase the risk of serious adverse drug reactions such as rhabdomyolysis. In addition, since concomitant therapy with a statin and ezemitibe has not provided sufficient evidence of the prevention of cardiovascular events, combined administration of lipid-lowering drugs has not been established for LDL-C management. From the above, combined therapy based on statins with other drugs, including those under development, is expected to be established.
Since even in patients with adequate reduction of the serum LDL-C levels, development of atherosclerotic disease, especially CAD, is not fully prevented, risk factors other than LDL-C should also be considered.Citation8,Citation9 For example, in the INTERHEART Study conducted on approximately 30000 patients in 52 countries, the association of various risk factors with the onset of acute myocardial infarction (AMI) was determined. This study reported the 9 important risk factors of smoking, abnormal lipid balance (apolipoprotein [Apo] B/ApoA1 ratio), hypertension, diabetes, abdominal obesity, stress, decreased consumption of fruits and vegetables, alcohol intake, and decreased physical activity. Judging from the odds ratio, the impact of these risk factors were equivalent in men and women and also in all regions of the world.Citation10 Because patients with these risk factors commonly have dyslipidemia, that is, hypertriglyceridemia and hypo-HDL cholestrolemia, management of serum triglyceride (TG) and high-density lipoprotein cholesterol (HDL-C) levels may also be as important as that of LDL-C for the prevention of atherosclerotic disease. Therefore, treatment of dyslipidemia requires management of the serum TG and HDL-C levels as well, as also of the complications of hypertension and diabetes, in addition to control of serum LDL-C levels, thus, combination therapy with a statin and other agents for dyslipidemia, hypertension, and diabetes should be considered. In particular, one of the recent major health issues emerging in developed countries is the metabolic syndrome, which has multiple risk factors other than LDL-C, and serves as a high risk factor for CHD. Patients with metabolic syndrome show high serum TG and low serum HDL-C levels, while the serum LDL-C levels may not be markedly elevated. Accordingly, statin monotherapy may not be efficient for comprehensive management of the lipid profile in these patients and concomitant therapy with other drugs for dyslipidemia, including fibrates and niacins, and cholesteryl ester transfer protein (CETP) inhibitors, which are under development, may be indicated. However, since concurrent therapy with statins and fibrates has been reported to be associated with an elevated risk of occurrence of rhabdomyolysis,Citation11 attention must be paid to drug–drug interactions when combined therapy with a statin and other drugs is considered. In addition, management of not only lipid parameters, but also of the blood pressure and glucose levels is important in patients with metabolic syndrome, and concurrent treatment of antihypertensive and antidiabetic drugs may be necessary. Nonetheless, there is little evidence regarding the efficacy of combination therapy with existing drugs for dyslipidemia, hypertension, and hyperglycemia and drugs under development. Results of further clinical studies on these issues are expected.
Taken together, for ideal dyslipidemia treatment, management of the serum TG, HDL-C levels and of complications such as hypertension and diabetes is also important in addition to strict LDL-C management. To achieve this goal satisfactorily, therapy based on conventional doses of statins with a minimum risk of drug interactions is required.
Pharmacological actions and mechanism of actions of pitavastatin
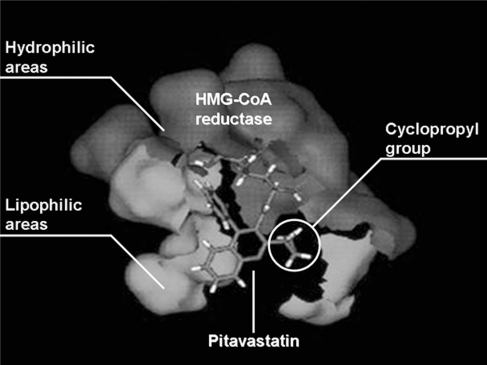
Pitavastatin has a characteristic structure, with heptenoate as the basic structure and a quinoline ring at the core. Its side chain has fluorophenyl and cyclopropyl moieties (). Its structure provides improved pharmacokinetics, including optimal activity as a HMG-CoA reductase inhibitor and better drug absorption. shows simulation imaging of the binding mode with the active site (spliced out 5Å from the active center) on the reductase.Citation12
Figure 1 Chemical structure of pitavastatin.
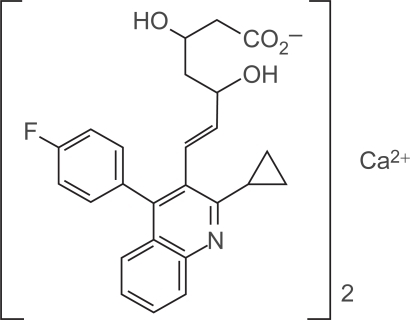
Figure 2 Binding image of pitavastatin and HMG-CoA reductase.Citation12
In one study, the IC50 of pitavastatin for HMG-CoA reductase inhibition in rat liver microsomes was 6.8 nM, being 2.4-fold higher than that of simvastatin and 6.8-fold higher than that of pravastatin.Citation13 Pitavastatin inhibits HMG-CoA reductase and synthesis of cholesterol in the liver like other statins, however, the IC50 for the inhibition of cholesterol synthesis from [14C] acetic acid in the cultured human hepatoma cell line HepG2 was found to be 5.8 nM, being 2.9-fold higher than that of simvastatin and 5.7-fold higher than that of atorvastatin.Citation14 Since these results might simply indicate stronger inhibition of HMG-CoA reductase by pitavastatin, the effects of the drugs on induction of the LDL receptor was compared at the standardized concentration determined by the inhibitory action of the drugs on cholesterol synthesis. Pitavastatin showed more effective induction of LDL receptor expression than either atorvastatin or simvastatin.Citation14 Pitavastatin induced expression of the LDL receptor more efficiently than the other statins and promoted the uptake of LDL from the blood to the liver to lower the serum LDL-C levels. The ED50 of oral pitavastatin for inhibition of sterol synthesis in the rat liver was 0.13 mg/kg, being 2.8-foldCitation13 and 15.9-fold higher, respectively, than that of simvastatin in rats and guinea pigs. This result showed pitavastatin inhibited the secretion of VLDL, one of the TG-rich lipoproteins, from the liver.Citation15 In addition, the effect on the secretion of ApoA1, a constituent of HDL, from the liver was evaluated using HepG2 cells. Pitavastatin was noted to have superior ApoA1 secretion-promoting effect as compared to atorvastatin and simvastatin. Pitavastatin was also found to promote ATP-binding cassette transporter A1 (ABCA1) expression in HepG2 cells, and to possibly facilitate HDL neogenesis by ApoA1-dependent cholesterol efflux in hepatocytes.Citation16
Pleiotropic effects of pitavastatin
Plaque rupture, the essential pathogenetic mechanism in acute coronary syndrome (ACS), is thought to be caused by structural changes, including thinning of the fibrous cap or increased lipid core, and provocation of a certain type of inflammation.Citation17 In general, statins have multifaceted effects called pleiotropic effects in addition to their LDL-C-lowering effect.Citation18 shows the pleiotropic effects of pitavastatin.
Table 1 Pleiotropic effects reported for pitavastatin
After administration of pitavastatin (0.5 mg/kg/day) in drinking water to Watanabe heritable hyperlipidemic (WHHL) rabbits for 16 weeks, the aortic arch of the animals was examined pathologically. Pitavastatin showed a tendency to improve the composition of vulnerable plaques, represented by increased collagen deposition and decreased macrophage infiltration ().Citation19 Imaging analysis of the aorta revealed that the area occupied by collagen and the α-actin-positive area increased by about 66% and 92%, respectively, in the pitavastatin group; on the other hand, the macrophage-positive area was reduced by about 39%.Citation19 Thus, pitavastatin may improve the composition of vulnerable plaques and help plaque stabilization.
Table 2 Effect of pitavastatin on components of aortic plaque in wHHL rabits
Additionally, in vitro experiments have shown that pitavastatin has an inhibitory effect on the C-reactive-protein-induced interleukin-8 (IL-8) production by endothelial cells, and also on monocyte adhesion to the endothelial cells, via monocyte chemoattractant protein-1 (MCP-1) stimulation,Citation20,Citation21 confirming the anti-inflammatory effects of the drug. Moreover, pitavastatin is reported to have an inhibitory effect on plasminogen activator inihibitor-1 (PAI-1)Citation22,Citation23 and tissue factor (TF)Citation23 which are important factors in thrombosis formation, and to induce tissue plasminogen activator (t-PA)Citation23 and thrombomodulin (TM) expression.Citation22,Citation24 Therefore, pitavastatin is expected to exert its anti-atherosclerotic effect via various mechanisms.
These pleiotropic effects of pitavastatin were compared with those of other statins using the inhibitory effects on the proliferation of smooth muscle cells (SMCs) derived from the human coronary arteries as an indicator. Even at low concentrations, pitavastatin was found to inhibit the proliferation of SMCs derived from human coronary arteries more strongly than atorvastatin, simvastatin, fluvastatin, rosuvastatin, or pravastatin.Citation25
To evaluate a new effect of pitavastatin on the blood vessels, the changes in the gene expression profiles brought about by statins were investigated in cultured normal human umbilical vein endothelial cells and normal human coronary artery SMCs by DNA microarray analysis. Pitavastatin inhibited the expression of pentraxin 3 (PTX3) related to acute inflammation.Citation26 PTX3 is found to be elevated especially in arterial inflammation in patients with unstable angina pectoris, and increased expression of PTX3 has attracted attention as a new effect of pitavastatin.Citation27
Pharmacokinetics of pitavastatin
Absorption, distribution, metabolism and excretion
In pharmacokinetic studies, pitavastatin has been demonstrated to show a high bioavailablity of 80% in rats and 88% in canines after administration at the dose of 1 mg/kg. It is distributed selectively to the target organ, the liver, and pharmacokinetic studies in rats conducted using 14C-pitavastatin have confirmed approximately 54 times higher radioactivity in the liver than that in the serum.Citation36
shows the metabolic pathway of pitavastatin. Many lipophillic drugs are metabolized in the liver by the drug-metabolizing enzyme, cytochrome P450 (CYP).Citation37,Citation38 Statins are also metabolized by CYPs, for example, lipophilic statins such as simvastatin and atorvastatin are metabolized by CYP3A4, and fluvastatin by CYP2C9.Citation39 Pitavastatin is lipophilic, but is scarcely metabolized by CYPs. It is rapidly glucuronized by uridine diphosphate-glucuronyltransferase (UGT) 1A1, UGT1A3, and UGT2B7, and is then converted to pitavastatin lactone, an inactive form, by elimination reaction of the glucuronic acid.Citation37 Pitavastatin is minimally metabolized by CYP2C9 to the M-13 form,Citation40 which is not detected clinically.Citation41 The CYP metabolic properties of pitavastatin are similar to those of the hydrophilic pravastatin and rosuvastatin, and pitavastatin is classified into a non-CYP metabolizable type ().Citation39 All statins but pitavastatin are metabolized by CYP3A4 after being transformed to the lactone form through glucuronidation, however, pitavastatin lactone is not metabolized by CYPs.Citation38
Figure 3 Metabolic pathway of pitavastatin. Adapted with permission from Fujino H, Yamada I, Shimada S, et al. Metabolic fate of pitavastatin, a new inhibitor of HMG-CoA reductase: human UDP-glucuronosyltransferase enzymes involved in lactonization. Xenobiotica. 2003;33(1):27–41;Citation37 Fujino H, Saito T, Tsunenari Y, et al. Metabolic properties of the acid and lactone forms of HMG-CoA reductase inhibitors. Xenobiotica. 2004;34(11–12):961–971.Citation38 Copyright © 2003, 2004 Taylor & Francis.
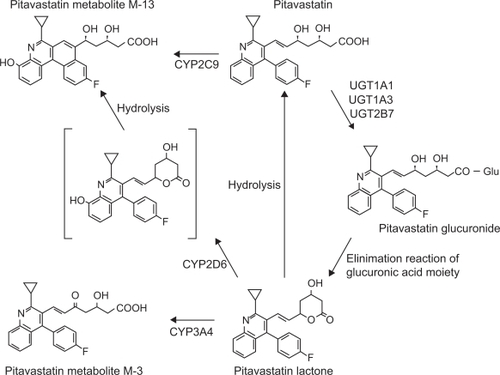
Table 3 Pharmacokinetic parameters of statins
To evaluate the effects of grapefruit juice (GFJ), a CYP3A4 inhibitor, on the pharmacokinetics of pitavastatin and atorvastatin, 8 healthy adults were administered either GFJ or water 3 times daily for 4 days, followed by a single dose of 4 mg pitavastatin or 20 mg atorvastatin. GFJ increased the area under the curve (AUC) 0–24 of atorvastatin by 83% (95% confidence interval [CI] 23% to 144%) and that of pitavastatin by only 13% (–3% to 29%).Citation42 Pitavastatin appears to be scarcely affected by CYP3A4-mediated drug–drug interaction.
The in vitro inhibitory effects of each type of statin on CYP metabolism were evaluated using model substrates. Simvastatin, simvastatin acid, and atorvastatin lactone inhibited CYP metabolism of the model substrates, while pitavastatin scarcely inhibited it.Citation43 This result suggests that pitavastatin is scarcely involved in drug–drug interactions mediated by CYPs.
As for the distribution of pitavastatin, it is reported to be taken up into the liver through organic anion transporter protein 2 (OATP2),Citation44 and the AUC0–24 of pitavastatin was increased by 4.6-fold by concurrent administration of cyclosporine, an OATP2 inhibitor.Citation45 Other statins are also reported to be taken up into the liver, mainly by OATP2, and combined therapy with cyclosporine increases their plasma concentrations.Citation46 On the other hand, multidrug resistance protein 1 (MDR1), a P glycoprotein, is not involved in pitavastatin pharmacokinetics.Citation47
Combined therapy may cause an increase in the blood concentration of either drug to increase the incidence of adverse drug reactions and enhance the effects. Pitavastatin is non-CYP metabolizable and rarely causes drug–drug interactions through CYP isoforms. Therefore, pitavastatin is expected to be easily applied for the treatment of patients with metabolic syndrome, which may require multidrug therapy, including drugs for dyslipidemia, hypertension and diabetes.
Pharmacokinetic study in patients with liver dysfunction
After administration of a single 2 mg dose pitavastatin, the plasma concentrations of 12 male patients with liver cirrhosis (6 patients with Child–Pugh grade A, 6 with Child–Pugh grade B disease) were compared with those of 6 healthy male volunteers without liver disease. 1.19-and 2.47-fold increase of the Cmax, and 1.27-and 3.64-fold increase of the AUCt were observed in patients with Child–Pugh grade A and Child–Pugh grade B, respectively, as compared with the values in healthy adults without liver disease.Citation48
Pharmacokinetic study in the elderly
The pharmacokinetics of plasma pitavastatin and pitavastatin lactone were compared between 6 elderly subjects aged 65 to 71 years and 5 non-elderly subjects aged 22 to 24 years who received repeated oral administration of pitavastatin 2 mg for 5 days. Pharmacokinetic parameters of pitavastatin and pitavastatin lactone did not significantly differ between the elderly and the non-elderly. Aging is considered to cause little change in the pharmacokinetics of pitavastatin.Citation49
Studies on efficacy
Studies of the LDL-C-lowering effect of pitavastatin
The LDL-C-lowering effect of statins increases in a dose-dependent manner, and the safety risk increases with dose escalation.Citation50 Therefore, the LDL-C-lowering effect at the initial dose is important, and the statins are classified into strong statins, which have a strong LDL-C-lowering action at the initial doses, including atorvastatin and rosuvastatin, and others.Citation51 Pitavastatin belongs to the category of strong statins due to the similar LDL-C-lowering action of this drug to that of atorvastatin at the initial dose.
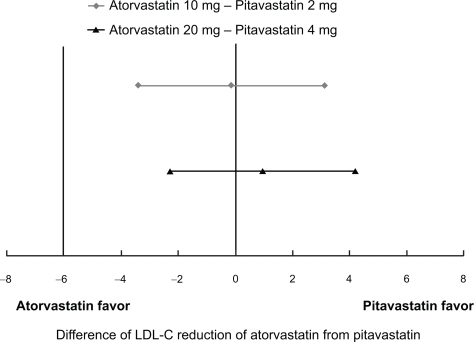
In a dose-finding study in patients with hypercholesterolemia conducted in Japan, where pitavastatin was first developed, the LDL-C-lowering effect of pitavastatin after 12-week administration was 34% (n = 81) at the dose of 1 mg, 42% (n = 75) at the dose of 2 mg, and 47% (n = 76) at the dose of 4 mg.Citation52 In a Phase III study, the effect of 12-week treatment with pitavastatin 2 mg was compared with that of pravastatin 10 mg. The mean percent reduction in LDL-C following pitavastatin treatment was 38% (n = 120) and that following pravastatin treatment was 18% (n = 105).Citation53 LDL-C reduction by pitavastatin 4 mg was observed by 46% (n = 25) after 8-week administration in another Phase II study similar to the dose finding study.Citation54 Almost similar results were obtained in the development studies conducted in Korea and Europe. In a Phase III study conducted in Korea, mean percent reduction in LDL-C after 8-week administration of pitavastatin 2 mg (n = 49) was 38%, similar to that in the control simvastatin 20 mg group (n = 46).Citation55 In a Phase III study conducted in Europe, mean percent reduction in LDL-C following 12-week administration of pitavastatin 2 mg (n = 315) and 4 mg (n = 298) were 38% and 45%, respectively, being comparable to that observed following administration of the control drug atorvastatin at 10 mg (n = 102) and 20 mg (n = 102) ().Citation56 In another Phase III study in Europe compared pitavastatin and simvastatin with the same design, pitavastatin 2 mg demonstrated significantly superior reduction in LDL-C by 39% (n = 307) to that of simvastatin 20 mg by 35% (n = 107) (p = 0.014) while pitavastatin 4 mg and simvastatin 40 mg demonstrated similar reduction in LDL-C by 44% (n = 319) and 43% (n = 110), respectively.Citation57
Figure 4 95% confidence interval on treatment difference in adjusted mean percentage change in LDL-C observed in phase III double-blind clinical trial of pitavastatin vs atorvastatin.Citation56
The efficacy of pitavastatin was evaluated in 30 heterozygous familial hypercholesterolemia patients. Decrease of the serum LDL-C levels by 40% was observed after 8-week administration of pitavastatin 2 mg, and by 48% after another 8-week administration at the dose of 4 mg.Citation58
From the above-mentioned clinical results on the LDL-C-lowering efficacy of statins, the LDL-C-lowering action of pitavastatin at doses of 2 to 4 mg was as strong as that of atorvastatin at doses of 10 to 20 mg; also, pitavastatin 2 mg was efficacious equivalent or more than simvastatin 20 mg.
Studies of the efficacy of pitavastatin on lipid parameters other than LDL-C
Since even in patients with sufficiently reduced serum LDL-C levels, development of atherosclerotic disease, especially CHD, is not fully prevented, other risk factors than LDL-C also should be considered. The clinical effects of pitavastatin on various lipid parameters other than LDL-C have been reported. In particular, pitavastatin has been demonstrated to show superior HDL-C-elevating effect as compared to atorvastatin.
In a Phase III study conducted in Japan, administration of pitavastatin 2 mg produced a statistically significant increase of the serum HDL-C level by 8.9%.Citation54 In a Phase III study conducted in Europe, significant increases of the serum HDL-C level by 4.0% and 5.0% were observed following administration of pitavastatin at the doses of 2 mg and 4 mg, respectively. In the same study, increases of the serum HDL-C level by 3.0% and 2.5% were observed following administration of atorvastatin at the doses of 10 mg and 20 mg, respectively, there being no significant difference in effect from that of pitavastatin.Citation56
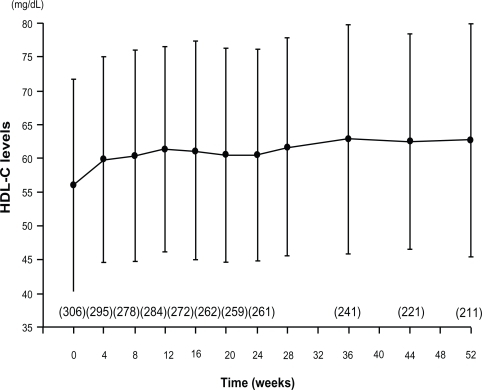
The HDL-C-elevating effect of some statins has been reported to diminish with long-term treatment.Citation59 A phase III long-term administration study of pitavastatin 1 to 4 mg for 52 weeks was conducted in 317 patients. The serum HDL-C level, which was 56.0 ± 15.7 mg/dL at the baseline, showed significant and sustained increase from 4 weeks of treatment, to rise by 6.0 mg/dL after 52 weeks ().Citation60 A total of 43 hypercholesterolemic patients with low serum HDL-C levels were examined to determine the effect of pitavastatin on the serum HDL-C levels. Administration of pitavastatin produced a significant and sustained increase of the serum HDL-C levels (from 36.0 ± 5.9 mg/dL at baseline to 40.5 ± 9.1 mg/dL at 12 months, P < 0.001) and Apo A-I levels (from 108.4 ± 18.0 mg/dL to 118.7 ± 19.3 mg/dL, P < 0.01).Citation61 In a clinical study conducted to confirm the effect of pitavastatin on the HDL metabolism,Citation30 29 patients with hypercholesterolemia were treated with pitavastatin 2 mg for 4 weeks. In this study, pitavastatin administration produced a decrease of the serum total cholesterol by 26.9% and of the serum LDL-C levels by 39.8%, with increase of the serum HDL-C and HDL2-C levels by 6.0% and 9.0%, respectively. On the other hand, there was no change of the serum HDL3-C level and significant decrease of the serum preβ1-HDL level.Citation62 In a randomized study comparing the HDL-C-elevating effect of pitavastatin 2 mg with that of atorvastatin 10 mg for 52 weeks, pitavastatin (n = 88) was significantly superior to atorvastatin (n = 85) in increasing the serum HDL-C levels (8.2% vs 2.9%, P = 0.031). The percent change in the serum Apo A-1 level in the pitavastatin group was significantly higher (5.1%) than that in the atorvastatin group (0.6%) (P = 0.019).Citation63 In a comparative study of pitavastatin and atorvastatin in Japanese hypercholesterolemic patients (Collaborative Study on Hypercholesterolemia Drug Intervention and Their Benefits for Atherosclerosis Prevention [CHIBA study]), the efficacy of pitavastatin 2 mg on the serum non-HDL-C levels was compared with that of atorvastatin 10 mg after 12-week treatment. The results revealed similar reduction of the serum non-HDL-C levels with pitavastatin treatment (39.0%, n = 93) and atorvastatin treatment (40.3%, n = 98), but a significant increase of the serum HDL-C levels only with pitavastatin treatment. In the CHIBA study, the waist circumference, body weight, and body mass index (BMI) were correlated with the percent reduction of the serum non-HDL-C only in the atorvastatin group. Improvement of the lipid parameters in the subgroup of patients with metabolic syndrome was more favorable in the pitavastatin group (n = 28) than in the atorvastatin group (n = 25). The pitavastatin group showed a significant increase of the serum HDL-C levels and decrease of the serum TG levels.Citation64
Figure 5 Time course of mean HDL-C over 52 weeks in a long-term study of pitavastatin.Citation60
As for the TG-lowering effect of pitavastatin in patients with pretreatment TG levels of 150 mg/dL or more, in a phase III study, pitavastatin 2 mg administration for 12 weeks (n = 50) produced a significant decrease of the serum TG levels by 23%, and in a phase II study, treatment with 4 mg of the drug for 8 weeks (n = 25) produced a significant decrease of the serum TG levels by 42%.Citation52,Citation54 In a double-blind placebo controlled cross-over study, pitavastatin 2 mg produced a significant decrease of the serum TG levels by 20% compared with placebo.Citation65
The effects of pitavastatin on the serum levels of other atherogenic lipoproteins, including remnant-like particle cholesterol (RLP-C) and small, dense LDL, have also been investigated. A total of 34 hypercholesterolemic patients with type 2 diabetes were treated with pitavastatin 2 mg for 8 weeks. With the treatment, significant decrease of the serum RLP-C levels and the proportion of small, dense LDL, and significant increase of the peak particle diameter, an indicator of the LDL particle size, were observed.Citation66 In the Kansai Investigation of Statin for Hyperlipidemic Intervention in Metabolism and Endocrinology (KISHIMEN), pitavastatin at the dose of 1 or 2 mg was administered to 178 patients with hypercholesterolemia for 6 to 12 months. Significant decreases of the serum LDL-C and RLP-C levels by 30.3% (n = 139) and 22.8% (n = 47), respectively, were observed. Serum TG levels decreased by 15.9% in 64 patients with basal TG levels of 150 mg/dL or more, and the serum HDL-C levels significantly increased.Citation67 The effects of pitavastatin 2 mg on the serum RLP-C and small, dense LDL-cholesterol levels were compared with those of atorvastatin 10 mg in heterozygous patients with familial hypercholesterolemia. A total of 17 heterozygous patients with familial hypercholesterolemia received pitavastatin 2 mg or atorvastatin 10 mg. After 12 weeks, the serum levels of RLP-C and small, dense LDL-C were significantly reduced in both groups, with no differences noted between the groups.Citation68
From the above clinical results on the effects of pitavastatin on lipid parameters other than LDL-C, pitavastatin exhibits TG-reducing and HDL-C-elevating effects, and the HDL-C elevating effect of pitavastatin is superior to that of atorvastatin. Pitavastatin also improves other atherogenic lipid parameters, including non-HDL-C, small, dense LDL, and RLP-C, as efficiently as atorvastatin. These comprehensive effects of pitavastatin on the lipid profile is expected to exert favorable effects on abnormal atherogenic lipoproteins and dysfunction of anti-atherosclerotic lipoproteins, which are typically noted in patients with metabolic syndrome, who need sufficient LDL-C-lowering treatment for reducing the risk of CHD, and frequently have hypertriglyceridemia and hypo-HDL-cholesterolemia.
Studies of the efficacy of pitavastatin on factors other than the lipid parameters
Since pitavastatin 2 to 4 mg has been demonstrated to show potent LDL-C reducing effects equivalent to atorvastatin 10 to 20 mg, it was expected that this drug would also reduce the risk of cardiovascular events, like atorvastatin. Several clinical studies have consistently demonstrated the efficacy of pitavastatin on plaques in the coronary arteries and in the carotid arteries while the usefulness of this effect as a surrogate marker is controversial.
Eighty-two patients matched for age and gender from among 870 patients undergoing intravascular ultrasound (IVUS)-guided percutaneous coronary intervention (PCI) were retrospectively assigned to either lipid-lowering therapy (n = 41, pitavastatin 2 mg) or a control group (n = 41, diet only). Significant reduction of the plaque volume index (PVI) was observed in the pitavastatin group (10.6% ± 9.4% decrease) as compared with that in the control group (8.1% ± 14.0% increase, P < 0.001). There were significant correlations between the percent change in the PVI and the follow-up serum LDL-C levels (r = 0.500, P < 0.001) and percent change of the serum LDL-C levels (r = 0.479, P < 0.001).Citation69 A prospective study to determine the effects on carotid plaques was conducted in patients treated with pitavastatin 4 mg (n = 33) or placebo (n = 32) within 3 days of onset of the acute coronary syndrome (ACS). In the pitavastatin group, greater improvement of the vulnerable carotid plaques at 1 month, as analyzed by carotid ultrasound integrated backscatter (IBS), was observed in the pitavastatin group as compared with that in the placebo group. Significantly greater improvement of the levels of inflammatory biomarkers, such as C-reactive protein (CRP), vascular endotherial growth factor (VEGF), and tumor necrosis factor alpha (TNF-α), at 1 month was observed in the pitavastatin group as compared with that in the placebo group.Citation70 To evaluate the effect on coronary plaques prospectively, the Japan Assessment of Pitavastatin and Atorvastatin in Acute Coronary Syndrome (JAPAN-ACS) Study was conducted in 252 patients with ACS who underwent IVUS-guided PCI. The effects of 8-month treatment with pitavastatin 4 mg and atorvastatin 20 mg were compared. The mean percent change in the plaque volume (PV) was −16.9% ± 13.9% in the pitavastain group and −18.1% ± 14.2% in the atorvastatin group, indicating a significant decrease in both groups. Administration of pitavastatin in patients with ACS is thus supposed to cause regression of coronary plaques ().Citation71 A similar study using pravastatin as control is ongoing.Citation72
Table 4 Percent changes of parameters for coronary plaque observed in JAPAN-ACS study
In addition, administration of pitavastatin has been reported to induce a decrease in the serum level of high-sensitivity CRP associated with atherosclerosis, and increase in the serum level of adiponectin.Citation67,Citation73 The short-and intermediate-term effects of pitavastatin and atorvastatin on the endothelial functions have been evaluated. The short-term effects of pitavastatin on the endothelial functions were superior to those of atorvastatin.Citation74 Moreover, beneficial effects of pitavastatin on the cardiac and renal functions, as well as on bone metabolism, have been reported.Citation75–Citation77 A clinical study is ongoing to evaluate the effect of pitavastatin for prevention of type 2 diabetes mellitus.Citation78
Safety and tolerability
According to the clinical findings obtained to date, the safety of pitavastatin at the initial dose is equivalent to that of the statins already on the market, and the tolerability at the initial dose is equivalent to that of atorvastatin. Pitavastatin is supposed to rarely cause adverse drug reactions (ADRs) related to glucose metabolism and the kidneys, notable new ADRs of strong statins.
Integrated safety analysis of clinical studies
In the clinical studies conducted in Japan prior to the drug approval, ADRs, as defined by signs and symptoms, occurred in 50 (5.6%) out of 886 patients. ADRs, as defined by laboratory abnormalities, occurred in 167 patients (18.8%), and included increase of the serum γ-glutamyl-transferase (GTP), creatine phosphokinase (CK [CPK]), serum alanine aminotransferase (ALT [glutamic pyruvic transaminase, GPT]), and aspartate aminotransferase (AST [glutamic oxaloacetic transaminase, GOT]) values, not specific to pitavastatin, and their frequency and severity were similar to those noted for the existing statins.Citation51 The incidence of ADRs by the dose of pitavastatin, as defined by signs, symptoms and laboratory abnormalities, for each dose was 20.3% (26/128 patients) for 1 mg, 23.3% (121/519) for 2 mg, and 20.9% (50/239) for 4 mg, demonstrating the absence of a dose relationship. There was no increase in the incidence or severity of ADRs due to long-term administration, and no development of new ADRs.Citation79
Comparative studies with other statins
In the Phase III double-blind comparative studies conducted in Japan, Korea and Europe, the safety profile of pitavastatin 2 mg was similar to that of pravastatin 10 mg, simvastatin 20 mg, and atorvastatin 10 mg. Thus, the safety of pitavastatin at the initial dose is considered to be equivalent to that of the other existing statins. Pitavastatin showed similar tolerability to atorvastatin 10 mg, and the safety of pitavastatin at an initial dose appeared to be same as that of atorvastatin.Citation53,Citation55,Citation56
ADRs due to high-dose statins are reported to be associated with a decrease in coenzyme Q10 (CoQ10). An open, randomized, cross-over study using pitavastatin 4 mg and atorvastatin 20 mg was conducted to compare their efficacy, safety, and effect to decrease the CoQ10 levels at an increased dose of them in 19 Japanese patients with heterozygous familial hypercholesterolemia. Plasma levels of CoQ10 were reduced by atorvastatin (–26.1%, P = 0.0007), but not by pitavastatin (–7.7%, P = 0.39).Citation80
Effects on glucose metabolism
Several studies have reported deterioration of the glucose metabolism following administration of statins.Citation81–Citation84 The effects of pitavastatin on glucose metabolism have been reported by several clinical studies.
Pitavastatin 1 mg or 2 mg was administered for 8 weeks to 79 type 2 diabetic patients with hypercholesterolemia who had never been treated with statins, and the effects on the fasting plasma glucose, hemoglobin A1c (HbA1c), AST, ALT, γ-GTP, and CK levels were evaluated. No statistically significant changes in the fasting plasma glucose levels (from 8.2 ± 2.7 to 8.3 ± 2.1 mmol/L) or HbA1c levels (from 7.3% ± 1.6% to 7.3% ± 1.5%) were observed following administration of pitavastatin. Changes in other clinical laboratories were also not statistically significant. None of the subjects withdrew from the study because of ADRs.Citation85
Glycemic control was retrospectively evaluated in type 2 diabetic patients receiving atorvastatin 10 mg (n = 99), pravastatin 10 mg (n = 85), or pitavastatin 2 mg (n = 95) for 3 months. The random blood glucose and HbA1c levels deteriorated only in the atorvastatin group.Citation86
A basic research was conducted to examine glucose uptake by insulin under administration of atorvastatin, simvastatin, pravastatin, or pitavastatin using 3T3-L1 cells. Glucose uptake was reduced in the atorvastatin and simvastatin groups, while no change was observed in the pravastatin or pitavastatin group. Reduction of solute carrier family 2, member 4 (SLC2A4) and CCAAT/enhancer binding protein (C/EBP) α expressions, involved in glucose uptake by cells, may occur, leading to a decrease of the glucose uptake following administration of atorvastatin.Citation87
Patient-focused outcomes
To detect 99% or more of unknown ADRs with an incidence of 0.05% or more, the LIVALO Effectiveness and Safety (LIVES) study was conducted in about 20000 patients with hypercholesterolemia or familial hypercholesterolemia for up to 2 years. A total of 20,279 patients were enrolled from 2811 facilities. The Treatment Outcome Study reported the analyzed results for 3 months after the initiation of pitavastatin administration. According to the results of 3-month treatment, the incidence of ADRs was 6.1% (1206/19921 patients).Citation88 As for the treatment outcome studies of other strong statins, the incidence of ADRs was 12.0% (576/4805 patients) for Lipitor® (atorvastatin) and 11.1% (978/8795 patients) for Crestor® (rosvastatin). The incidence of ADRs to pitavastatin was about a half compared with the above incidences.Citation89,Citation90
According to the analyzed results after 2 years of pitavastatin administration, the incidence of ADRs was 10.4%. Regarding the main ADRs of statins, the incidence of ADRs related to the musculoskeletal system was 2.1%, and that related to liver dysfunction was 1.0%. According to the severity, mild ADRs occurred in 1045 patients, moderate in 155, and severe in 6 patients. Almost all of the ADRs were classified as mild. shows the major ADRs. The major ADRs, CK increased and transaminase increased, occurred less frequently than that noted with other strong statins. The ADRs related to glucose metabolism or the kidneys, notable new ADRs of strong statins, scarcely occurred. In the stratified analysis on the occurrence of ADRs by the concomitantly administered drugs, no significant increase in the incidence of ADRs was observed even when azole antifungals, macrolide antibiotics, or coumarin anticoagulants, which should be given with care due to drug–drug interactions though CYPs for other statins, were administered concomitantly. In addition, concomitant administration of various antiplatelet, antihypertensive and/or antidiabetic drugs did not significantly increase the incidence of ADRs. These results suggest the absence of any special problems related to drug-drug interactions for pitavastatin. shows the presumed cumulative incidence of ADRs using the Kaplan-Meier method over 2 years after the initiation of pitavastatin treatment. The incidence rose gradually from 12 weeks to 52 weeks, with no abrupt increase in the incidence of ADRs.Citation91
Figure 6 Cumulative incidence of adverse drug reactions by Kaplan-Meier method in LIVES study.Citation91
Modified from Kurihara et al.Citation91
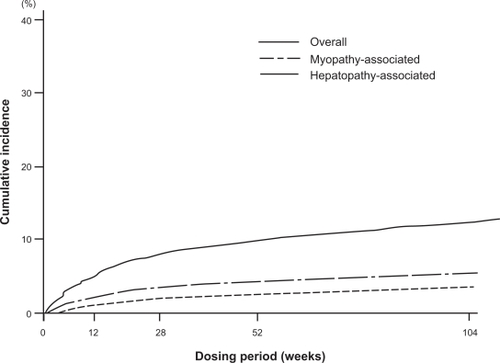
The results at 104 weeks have been analyzed until date, and the LIVES-Extension study is ongoing; it is expected to be carried out for another 3 years, with total follow-up duration of 5 years.
Conclusion
Cerivastatin was withdrawn from the market due to reports of fatal rhabdomyolysis induced by high-doses of cerivastatin or drug–drug interactions caused by coadministration of gemfibrozil. Recently, strong statins such as atorvastatin and rosuvastatin have been widely used for their potent LDL-C-lowering effect at the initial dose, and combinations of these drugs with ezetimibe have been more frequently applied than increase in the dose of the statins. However, serum LDL-C treatment goal have not been achieved in high-risk patients, particularly those with multiple risk factors for CHD in routine clinical settings in Europe, the US, or Japan. Therefore, since high-dose statin administration should be avoided, it is anticipated that a new drug to be coadministered with statins will appear as an alternative to ezemitibe in the future.
Pitavastatin is a strong statin with the same LDL-C-lowering effect as that of atorvastatin at the initial dose and associated with minimal drug–drug interactions. Although various LDL-C-lowering drugs under development are expected to become available for clinical use in the future, the use of statins as the mainstay for the treatment of dyslipidemias appears to remain unchanged. Therefore, pitavastatin may have the potential to become the standard drug for dyslipidemia treatment because of its potent LDL-C-lowering effect, equivalent to that of atorvastatin at the initial dose, and association with minimal drug–drug interactions.
Moreover, pitavastatin has TG-lowering and HDL-elevating effects, and is anticipated to be useful in improving the overall lipid profile. In particular, serum HDL-C elevation by pitavastatin is superior to that observed for atorvastatin. These pitavastatin profiles are favorable for the treatment of metabolic syndrome patients, which is a major concern in developed countries because of its association with a high risk of CHD. The reasons why pitavastatin would be favored for the treatment of metabolic syndrome are as follows. First, the serum LDL-C levels are not markedly elevated in most patients with metabolic syndrome, however, these patients also require sufficient decrease of the serum LDL-C because of the associated high risk of CHD. Second, patients with metabolic syndrome frequently show elevated serum TG and reduced serum HDL-C levels, and statin monotherapy is often inadequate for satisfactory overall control of the lipid profile. Since pitavastatin is a strong statin associated with a low risk of drug–drug interactions, there is little concern about drug–drug interactions when it is administered to patients with metabolic syndrome in combination with antihypertensive and/or antidiabetic agents. Therefore, pitavastatin may have the potential to become the standard drug for the treatment of metabolic syndrome, because it is suitable for improving the overall lipid profile in patients with metabolic syndrome, the incidence of which appears to continue to increase throughout the world, and the drug is associated with a low risk of drug–drug interactions.
In conclusion, pitavastatin is strongly expected to become a standard agent for the treatment of dyslipidemia, especially for the treatment of dyslipidemia in patients with metabolic syndrome.
Acknowledgments/disclosures
The author reports no conflicts of interest in this work.
References
- TeramotoTSasakiJUeshimaHExecutive summary of Japan Atherosclerosis Society (JAS) guideline for diagnosis and prevention of atherosclerotic cardiovascular diseases for JapaneseJ Atheroscler Thromb2007142455017485887
- GrundySMCleemanJIMerzCNNational Heart, Lung, and Blood Institute; American College of Cardiology Foundation; American Heart AssociationImplications of recent clinical trials for the National Cholesterol Education Program Adult Treatment Panel III guidelinesCirculation20041102227239Erratum in: Circulation 2004;110(6):763.15249516
- GrahamIAtarDBorch-JohnsenKEuropean guidelines on cardiovascular disease prevention in clinical practice: full text. Fourth Joint Task Force of the European Society of Cardiology and other societies on cardiovascular disease prevention in clinical practice (constituted by representatives of nine societies and by invited experts)Eur J Cardiovasc Prev Rehabil200714Suppl 2S1S11317726407
- BaigentCKeechAKearneyPMCholesterol Treatment Trialists’ (CTT) CollaboratorsEfficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statinsLancet200536694931267127816214597
- BrugtsJJYetginTHoeksSEThe benefits of statins in people without established cardiovascular disease but with cardiovascular risk factors: meta-analysis of randomised controlled trialsBMJ2009338b237619567909
- DavidsonMHMakiKCPearsonTAResults of the National Cholesterol Education (NCEP) Program Evaluation ProjecT Utilizing Novel E-Technology (NEPTUNE) II survey and implications for treatment under the recent NCEP Writing Group recommendationsAm J Cardiol200596455656316098311
- TeramotoTKashiwagiAMabuchiHStatus of lipid-lowering therapy prescribed based on recommendations in the 2002 report of the Japan atherosclerosis society guideline for diagnosis and Treatment of Hyperlipidemia in Japanese Adults: A study of the Japan lipid assessment program (J-LAP)Curr Ther Res Clin Exp20056628095
- BarterPGottoAMLaRosaJCTreating to New Targets Investigators. HDL cholesterol, very low levels of LDL cholesterol, and cardiovascular eventsN Engl J Med2007357131301131017898099
- DembowskiEDavidsonMHA review of lipid management in primary and secondary preventionJ Cardiopulm Rehabil Prev200929121219158581
- YusufSHawkenSOunpuuSINTERHEART Study InvestigatorsEffect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control studyLancet2004364943893795215364185
- McClureDLValuckRJGlanzMStatin and statinfibrate use was significantly associated with increased myositis risk in a managed care populationJ Clin Epidemiol200760881281817606177
- YamazakiHFujinoHKanazawaMPharmacological and pharmacokinetic features and clinical effects of pitavastatin (Livalo Tablet®). [In Japanese]Folia Pharmacol Jpn2004123349362
- AokiTNishimuraHNakagawaSPharmacological profile of a novel synthetic inhibitor of 3-hydroxy-3-methylglutaryl-coenzyme A reductaseArzneimittelforschung19974789049099296275
- MorikawaSUmetaniMNakagawaSRelative induction of mRNA for HMG CoA reductase and LDL receptor by five different HMG-CoA reductase inhibitors in cultured human cellsJ Atheroscler Thromb20007313814411480454
- SuzukiHAokiTTamakiTHypolipidemic effect of NK-104, a potent HMG-CoA reductase inhibitor, in guinea pigsAtherosclerosis1999146225927010532682
- MaejimaTYamazakiHAokiTEffect of pitavastatin on apolipoprotein A-I production in HepG2 cellBiochem Biophys Res Commun2004324283583915474503
- RossRAtherosclerosis–an inflammatory diseaseN Engl J Med199934021151269887164
- TakemotoMLiaoJKPleiotropic effects of 3-hydroxy-3-methylglutaryl coenzyme a reductase inhibitorsArterioscler Thromb Vasc Biol200121111712171911701455
- SuzukiHKobayashiHSatoFPlaque-stabilizing effect of pitavastatin in Watanabe heritable hyperlipidemic (WHHL) rabbitsJ Atheroscler Thromb200310210911612740485
- KibayashiEUrakazeMKobashiCInhibitory effect of pitavastatin (NK-104) on the C-reactive-protein-induced interleukin-8 production in human aortic endothelial cellsClin Sci (Lond)2005108651552115701058
- HiraokaMNittaNNagaiMMCP-1-induced enhancement of THP-1 adhesion to vascular endothelium was modulated by HMG-CoA reductase inhibitor through RhoA GTPase-, but not ERK1/2-dependent pathwayLife Sci200475111333134115234191
- MorikawaSTakabeWMatakiCThe effect of statins on mRNA levels of genes related to inflammation, coagulation, and vascular constriction in HUVEC. Human umbilical vein endothelial cellsJ Atheroscler Thromb20029417818312226549
- MarkleRAHanJSummersBDPitavastatin alters the expression of thrombotic and fibrinolytic proteins in human vascular cellsJ Cell Biochem2003901233212938153
- MasamuraKOidaKKaneharaHPitavastatin-induced thrombomodulin expression by endothelial cells acts via inhibition of small G proteins of the Rho familyArterioscler Thromb Vasc Biol200323351251712615662
- NakanoKEgashiraKPitavastatin has most potent pro-healing effects on endothelial cells and inhibitory effects on proliferation of vascular smooth muscle cells-a potential treatment strategy for drug-eluting stentsThe 41st Annual Scientific Meeting of the Japan Atherosclerosis Society (July, 2009) general presentation No. 21.
- MorikawaSTakabeWMatakiCGlobal analysis of RNA expression profile in human vascular cells treated with statinsJ Atheroscler Thromb2004112627215153665
- InoueKSugiyamaAReidPCEstablishment of a high sensitivity plasma assay for human pentraxin3 as a marker for unstable angina pectorisArterioscler Thromb Vasc Biol200727116116717095712
- InoueIItohFAoyagiSFibrate and statin synergistically increase the transcriptional activities of PPARalpha/RXRalpha and decrease the transactivation of NFkappaBBiochem Biophys Res Commun2002290113113911779144
- SagaraNKawajiTTakanoAEffect of pitavastatin on experimental choroidal neovascularization in ratsExp Eye Res20078461074108017418120
- KohnoMShinomiyaKAbeSInhibition of migration and proliferation of rat vascular smooth muscle cells by a new HMG-CoA reductase inhibitor, pitavastatinHypertens Res200225227928512047044
- HanJZhouXYokoyamaTPitavastatin downregulates expression of the macrophage type B scavenger receptor, CD36Circulation200410979079614970117
- KawakamiATaniMChibaTPitavastatin inhibits remnant lipoprotein-induced macrophage foam cell formation through ApoB48 receptor-dependent mechanismArterioscler Thromb Vasc Biol200525242442915591219
- HiraokaMYoshidaMA novel HMG-CoA reductase inhibitor, pitavastatin inhibits IL-6-induced CRP in liver cells via ERK1/2-dependent but not STAT3-dependent signaling transductionCirc J200367Suppl 1271
- ChinenIShimabukuroMYamakawaKVascular lipotoxicity: endothelial dysfunction via fatty-acid-induced reactive oxygen species overproduction in obese Zucker diabetic fatty ratsEndocrinology2007148116016517023526
- OtaKSuehiroTAriiKEffect of pitavastatin on transactivation of human serum paraoxonase 1 geneMetabolism200554214215015690306
- KimataHFujinoHKoideTStudies on the metabolic fate of NK-104, a new Inhibitor of HMG-CoA reductase (1): Absorption, distribution, metabolism and excretion in ratsDrug Metab Pharmacokinet1998135484498
- FujinoHYamadaIShimadaSMetabolic fate of pitavastatin, a new inhibitor of HMG-CoA reductase: human UDP-glucuronosyltransferase enzymes involved in lactonizationXenobiotica2003331274112519692
- FujinoHSaitoTTsunenariYMetabolic properties of the acid and lactone forms of HMG-CoA reductase inhibitorsXenobiotica20043411–1296197115801541
- MukhtarRYReidJRecklessJPPitavastatinInt J Clin Pract200559223925215854203
- FujinoHYamadaIKojimaJStudies on the metabolic fate of NK-104, a new inhibitor of HMG-CoA reductase. (5). In vitro metabolism and plasma protein binding in animals and humansXenobio Metabol Dispos1999146415424
- NakayaNTatenoMNakamuraTPharmacokinetics of reported dose NK-104 (pitavastatin) in healthy elderly and non-elderly volunteers [in Japanese]J Clin Therap Med2001176957970
- AndoHTsuruokaSYanagiharaHEffects of grapefruit juice on the pharmacokinetics of pitavastatin and atorvastatinBr J Clin Pharmacol200560549449716236039
- SakaedaTFujinoHKomotoCEffects of acid and lactone forms of eight HMG-CoA reductase inhibitors on CYP-mediated metabolism and MDR1-mediated transportPharm Res200623350651216388406
- HiranoMMaedaKShitaraYContribution of OATP2 (OATP1B1) and OATP8 (OATP1B3) to the hepatic uptake of pitavastatin in humansJ Pharmacol Exp Ther2004311113914615159445
- HasunumaTNakamuraMYajiTThe drug-drug interactions of pitavastatin (NK-104), a novel HMG-CoA reductase inhibitor and cyclosporine [in Japanese]J Clin Therap Med2003194381389
- NeuvonenPJNiemiMBackmanJTDrug interactions with lipid-lowering drugs: mechanisms and clinical relevanceClin Pharmacol Ther200680656558117178259
- FujinoHYamadaIShimadaSMetabolic fate of pitavastatin, a new inhibitor of HMG-CoA reductase–effect of cMOAT deficiency on hepatobiliary excretion in rats and of mdr1a/b gene disruption on tissue distribution in miceDrug Metab Pharmacokinet200217544945615618696
- HuiCKCheungBMLauGKPharmacokinetics of pitavastatin in subjects with Child-Pugh A and B cirrhosisBr J Clin Pharmacol200559329129715752374
- NakayaNTatenoMNakamuraTPharmacokinetics of repeated dose NK-104 (pitavastatin) in healthy elderly and non-elderly volunteers [in Japanese]J Clin Therap Med2001176957970
- JacobsonTAThe safety of aggressive statin therapy: how much can low-density lipoprotein cholesterol be lowered?Mayo Clin Proc20068191225123116970219
- HayashiTYokoteKSaitoYPitavastatin: efficacy and safety in intensive lipid loweringExpert Opin Pharmacother2007108142315232717927486
- SaitoYTeramotoTYamadaNClinical Efficacy of NK-104 (Pitavastatin), a New Synthetic HMG-CoA Reductase inhibitor, in the Dose Finding, Double Blind, Three-group Comparative Study [in Japanese]J Clin Therap Med2001176829855
- SaitoYYamadaNTeramotoTA randomized, double-blind trial comparing the efficacy and safety of pitavastatin versus pravastatin in patients with primary hypercholesterolemiaAtherosclerosis2002162237337911996957
- NakayaNSaitoYMorisakiNPhase II Clinical Study of NK-104 (Pitavastatin) in Patients with Hyperlipidemia [in Japanese]J Clin Therap Med2001176789806
- ParkSKangHJRimSJA randomized, open-label study to evaluate the efficacy and safety of pitavastatin compared with simvastatin in Korean patients with hypercholesterolemiaClin Ther20052771074108216154486
- BudinskiDArnesonVHounslowNPitavastatin compared with atorvastatin in primary hypercholesterolemia or combined dyslipidemiaClinical Lipidology200943291302
- OseLBudinskiDHounslowNComparison of Pitavastatin to Simvastatin in Primary Hypercholesterolemia or Combined DyslipidemiaCurr Med Res Opin2009In press.
- KajinamiKKoizumiJUedaKEffects of NK-104, a new hydroxymethylglutaryl-coenzyme reductase inhibitor, on low-density lipoprotein cholesterol in heterozygous familial hypercholesterolemia. Hokuriku NK-104 Study GroupAm J Cardiol200085217818310955373
- OlssonAGIstadHLuurilaORosuvastatin Investigators GroupEffects of rosuvastatin and atorvastatin compared over 52 weeks of treatment in patients with hypercholesterolemiaAm Heart J200214461044105112486429
- TeramotoTSaitoYYamadaNClinical safety and efficacy of NK-104 (pitavastatin), a new synthetic HMG-CoA reductase inhibitor, in the long-term treatment of hyperlipidemia – results of a multicenter long-term study. [in Japanese]J Clin Therap Med2001176885913
- FukutomiTTakedaYSuzukiSHigh density lipoprotein cholesterol and apolipoprotein A-I are persistently elevated during long-term treatment with pitavastatin, a new HMG-CoA reductase inhibitorInt J Cardiol200910[Epub Jan 12 2009].
- KawanoMNagasakaSYagyuHPitavastatin decreases plasma prebeta1-HDL concentration and might promote its disappearance rate in hypercholesterolemic patientsJ Atheroscler Thromb2008151414618270457
- SasakiJIkedaYKuribayashiTA 52-week, randomized, open-label, parallel-group comparison of the tolerability and effects of pitavastatin and atorvastatin on high-density lipoprotein cholesterol levels and glucose metabolism in Japanese patients with elevated levels of low-density lipoprotein cholesterol and glucose intoleranceClin Ther200830610891010118640465
- YokoteKBujoHHanaokaHMulticenter collaborative randomized parallel group comparative study of pitavastatin and atorvastatin in Japanese hypercholesterolemic patients: collaborative study on hyper-cholesterolemia drug intervention and their benefits for atherosclerosis prevention (CHIBA study)Atherosclerosis2008201234535218472103
- SasakiJIkedaYYamamotoKEffect of NK-104 (Pitavastatin) on Serum Lipids in Patients with Hypertriglyceridemia – Double-Blind, Cross-Over Placebo Controlled Study – [in Japanese]J Clin Therap Med2001176807827
- SoneHTakahashiAShimanoHHMG-CoA reductase inhibitor decreases small dense low-density lipoprotein and remnant-like particle cholesterol in patients with type-2 diabetesLife Sci200271202403241212231401
- KoshiyamaHTaniguchiATanakaKKansai Investigation of Statin for Hyperlipidemic Intervention in Metabolism and Endocrinology Investigators. Effects of pitavastatin on lipid profiles and high-sensitivity CRP in Japanese subjects with hypercholesterolemia: Kansai Investigation of Statin for Hyperlipidemic Intervention in Metabolism and Endocrinology (KISHIMEN) investigatarsJ Atheroscler Thromb200815634535019075492
- NozueTMichishitaIItoYEffects of statin on small dense low-density lipoprotein cholesterol and remnant-like particle cholesterol in heterozygous familial hypercholesterolemiaJ Atheroscler Thromb200815314615318603821
- TakashimaHOzakiYYasukawaTImpact of lipid-lowering therapy with pitavastatin, a new HMG-CoA reductase inhibitor, on regression of coronary atherosclerotic plaqueCirc J200771111678168417965484
- NakamuraTObataJEKittaYRapid stabilization of vulnerable carotid plaque within 1 month of pitavastatin treatment in patients with acute coronary syndromeJ Cardiovasc Pharmacol200851436537118427279
- HiroTKimuraTMorimotoTEffect of intensive statin therapy on regression of coronary atherosclerosis in patients with acute coronary syndrome: a multi-center randomized trial evaluated by volumetric intravascular ultrasound using pitavastatin versus atorvastatin (JAPAN-ACS Study)J Am Coll Cardiol20095429330219608026
- NozueTYamamotoSTohyamaSTreatment with statin on atheroma regression evaluated by intravascular ultrasound with Virtual Histology (TRUTH Study): rationale and designCirc J200973235235519110505
- InamiNNomuraSShouzuAEffects of pitavastatin on adiponectin in patients with hyperlipidemiaPathophysiol Haemost Thromb20073611818332608
- SakabeKFukudaNFukudaYComparisons of short-and intermediate-term effects of pitavastatin versus atorvastatin on lipid profiles, fibrinolytic parameter, and endothelial functionInt J Cardiol2008125113613817400311
- AoyagiTNakamuraFTomaruTBeneficial effects of pitavastatin, a 3-hydroxy-3-methylglutaryl coenzyme a reductase inhibitor, on cardiac function in ischemic and nonischemic heart failureInt Heart J2008491495818360064
- NakamuraTSugayaTKawagoeEffect of pitavastatin on urinary liver-type fatty-acid-binding protein in patients with nondiabetic mild chronic kidney diseaseAm J Nephrol2006261828616534182
- MajimaTShimatsuAKomatsuYShort-term effects of pitavastatin on biochemical markers of bone turnover in patients with hypercholesterolemiaIntern Med200746241967197318084118
- ClinicalTrialsgov [web site on the Internet] United States: the US National Institute of Health; ClinicalTrials.gov identifier: NCT00301392: Japan Prevention Trial of Diabetes by Pitavastatin in Patients With Impaired Glucose Tolerance (J-PREDICT) [updated on 2007 Jan 19; cited on 2006 Mar 5] Available from: http://clinicaltrials.gov/ct2/
- TajimaSHMG-CoA Reductase Inhibitor LIVALO Tablet [in Japanese]HosodaSSasayamaSKitamuraSThe series of advanced medicine, No 28 Cardiac Diseases “The frontier of diagnosis and treatment of cardiac diseases”TokyoResearch Center for Advanced Medical Technology2004343348
- KawashiriMANoharaATadaHComparison of effects of pitavastatin and atorvastatin on plasma coenzyme Q10 in heterozygous familial hypercholesterolemia: results from a crossover studyClin Pharmacol Ther200883573173917957184
- SeverPSDahlöfBPoulterNRASCOT investigatorsPrevention of coronary and stroke events with atorvastatin in hypertensive patients who have average or lower-than-average cholesterol concentrations, in the Anglo-Scandinavian Cardiac Outcomes Trial – Lipid Lowering Arm (ASCOT-LLA): a multicentre randomised controlled trialLancet200336193641149115812686036
- SabatineMSWiviottSDMorrowDAHighi-Dose Atorvastatin Associated with Glycemic Control: A PROVE-IT TIMI 22 SubstudyCirculation2004110Suppl IS834
- ColhounHMBetteridgeDJDurringtonPNCARDS investigators. Primary prevention of cardiovascular disease with atorvastatin in type 2 diabetes in the Collaborative Atorvastatin Diabetes Study (CARDS): multicentre randomised placebo-controlled trialLancet2004364943568569615325833
- RidkerPMDanielsonEFonsecaFAJUPITER Study GroupRosuvastatin to prevent vascular events in men and women with elevated C-reactive proteinN Engl J Med2008359212195220718997196
- KawaiTTokuiMFunaeOEfficacy of pitavastatin, a new HMG-CoA reductase Inhibitor, on lipid and glucose metabolism in patients with type 2 diabetesDiabetes Care200528122980298116306567
- YamakawaTTakanoTTanakaSInfluence of pitavastatin on glucose tolerance in patients with type 2 diabetes mellitusJ Atheroscler Thromb200815526927518981652
- NakataMNagasakaSKusakaIEffects of statins on the adipocyte maturation and expression of glucose transporter 4 (SLC2A4): implications in glycaemic controlDiabetologia20064981881189216685502
- KuriharaYDouzonoTKawakitaKA large-scale, prospective post-marketing surveillance of pitavastatin (LIVALO® Tablet) – drug use investigation. [in Japanese]Jpn Pharmacol Ther200751940
- KomanoNMasakiMKawaiHThe safety and efficacy in post-marketing surveys of atorvastatin. [in Japanese]Prog Med2005251131142
- YoshidaSCrestor: Safety and efficacy in clinical esperience investigation. [in Japanese]Prog Med200727511591189
- KuriharaYDouzonoTKawakitaKA large-scale, long-term, prospective post-marketing surveillance of pitavastatin (LIVALO® Tablet) – LIVALO Effectiveness and Safety (LIVES) StudyJpn Pharmacol Ther2008368709731