Abstract
Complications of pacemaker implantation include myocardial perforation, venous thrombosis, vegetations of the tricuspid valve or pacing lead, and tricuspid regurgitation. We report a patient presenting with a case of delayed ventricular lead perforation through the right ventricle. The lead was uneventfully extracted under transesophageal echocardiographic observation in the operating room with cardiac surgery backup.
Keywords:
Introduction
Implantation of permanent pacemakers (PM) represents an effective treatment option for several cardiac arrhythmias. The incidence of acute complications from device implantation, such as pneumothorax, cardiac effusion, and lead perforation ranges from 1% to 7%.Citation1,Citation2 Delayed complications mostly include infection, subclavian vein thrombosis, failure of sensing and pacing, and erosion of the pulse generator or lead connections.Citation3 As a rare late complication, delayed lead perforation has also been reported in several case reports.Citation4–Citation7 This complication is defined as delayed perforation beyond one month of device implantation. We report a case of uneventful transvenous extraction of a passive fixation lead with perforation of the right ventricle three months after implantation of a permanent pacemaker.
Case report
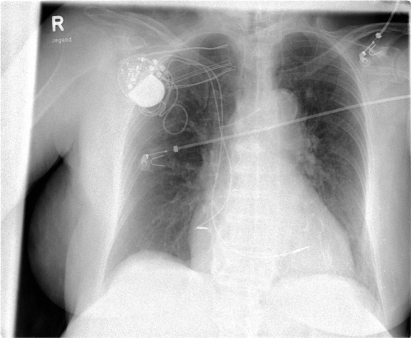
A 78-year-old female presented to our department with asymptomatic right ventricular lead dislocation. Three months earlier she underwent implantation of a permanent dual-chamber pacemaker (St. Jude Medical Verity ADx XL DR 5356) with the following fixation leads (atrial: Medtronic 5076-58 cm active fixation lead; ventricular: Medtronic 4074-58 cm passive fixation lead) due to sick sinus syndrome and intermittent atrioventricular block II. The chest X-ray prior to discharge showed correct position of the atrial and ventricular leads (). Routine testing one month after implantation was uneventful. Testing after three months showed loss of ventricular sensing and pacing. A chest X-ray was performed but was not highly suspicious for lead dislocation (). However, chest computed tomography (CT) with 3-D reconstruction of the lateral wall of the right ventricle confirmed perforation of the passive-fixation right ventricular lead through the right ventricle and pericardium into the left lateral chest from the right ventricular apical site (). Transthoracic echocardiography (TTE) showed no pericardial effusion. Lead explantation was scheduled. The right ventricular lead was then retracted into the right ventricle and explanted under surveillance by transesophageal echocardiography (TEE) with cardiothoracic backup in the operation room. TEE showed intraoperatively no pericardial effusion. The patient presented stable hemodynamics during the whole procedure. In the next step, a new ventricular lead (Medtronic 5076-58 cm) was implanted via transvenous approach. Under stable conditions, the patient was admitted to the intensive care unit for close monitoring. There was no pericardial effusion prior to discharge and chest X-ray demonstrated correct position of the leads (). The patient was discharged with correct pacemaker function on the second postoperative day.
Figure 1 Chest X-ray after pacemaker implantation.
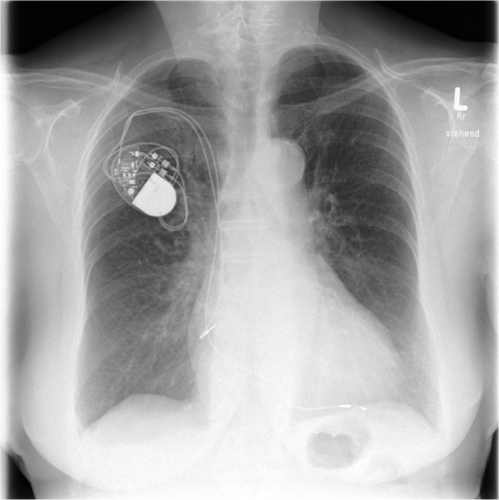
Figure 2 A) Three-month follow-up chest X-ray; B) three-month follow-up lateral chest X-ray suspicious of dislocation.
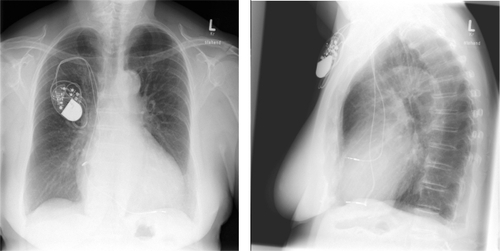
Figure 3 A) Chest computed tomography (CT) shows a perforated ventricular lead tip through the right ventricle and pericardium. B) 3D-recontruction of CT shows a perforated ventricular lead tip through the right ventricle and pericardium.
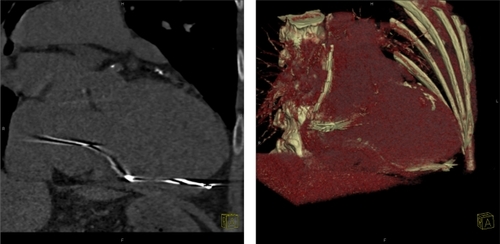
Figure 4 Chest X-ray prior to discharge demonstrates correct position of the leads.
Discussion
Unlike acute myocardial perforation, that has been reported to occur in 1%–7% of pacemaker implantation,Citation1 late perforation (diagnosed later than one month after implantation) is less well recognized as a classic complication of pacemaker implantation. Clinical presentation of late perforation may vary widely from asymptomatic patients to sudden cardiac death. This highlights the importance of a high degree of suspicion and the need of proper diagnostic methods. In our case, the patient showed neither of the typical symptoms like chest pain, diaphragmatic pacing or pericardial friction rubs.Citation8 But ECG showed failure of ventricular sensing and pacing. Chest X-ray was not suspicious for myocardial perforation and CT-scan, showing the lead’s tip outside the heart shadow, was necessary to make the diagnosis. In our opinion, imaging diagnostic with CT-scan should be reserved for patients with unsuspicious chest X-ray presenting with an exit-block at least one month after implantation.
Currently, appropriate management of lead perforation is uncertain. Furthermore, the management described in the literature depends on the lead type. While active fixation leads have mostly been extracted transvenously after retraction of the coil, extraction of passive fixation leads causes concern because of the bulky tip of the lead may cause tissue damage during removal. Khan and colleagues recommend that lead extraction should be done in the operating room under TEE observation with cardiac surgery backup.Citation4 Although open chest surgery offers more safety in the extraction of the lead, this invasive procedure is associated with increased hospital stay. In our opinion, removal and repositioning of the perforated lead or implantation of a new one are less invasive as open chest surgery. An alternative approach to minimize the risk of perforation could be to place the lead in sites other than the right ventricular apex such as the atrial or ventricular septal walls.Citation9
Conclusions
Delayed lead perforation is a rare complication of pacemaker implantation. Considering our findings and those of others, management schemes for patients who present with delayed lead perforation should be provided.
References
- KiviniemiMSPirnesMAEränenHJKettunenRVHartikainenJEComplications related to permanent pacemaker therapyPacing Clin Electrophysiol19992271172010353129
- TriganoJAPaganelliFRichardPPerforation du Cœur après Implantation Transveineuse de Stimulation CardiaquePresse Med19992883684010337335
- EllenbogenKAWoodMAShepardRKDelayed complications following pacemaker implantationPacing Clin Electrophysiol2002251155115812358163
- KhanMJosephGKhaykinYZiadaKWilkoffBDelayed lead perforation: A disturbing trendPacing Clin Electrophysiol20052825125315733190
- AkyolAAydinAErdinlerIOguzELate perforation of the heart, pericardium, and diaphragm by an active-fixation ventricular leadPacing Clin Electrophysiol20052835035115826277
- SanoussiAEl NakadiBLardinoisIDe BruyneYJorisMLate right ventricular perforation after permanent pacemaker implantation: How far can the lead goPacing Clin Electrophysiol20052872372516008811
- VelavanPAn unusual presentation of delayed cardiac perforation caused by atrial screw in leadHeart20038936412639855
- AsanoMMishimaAIshiiTTakeuchiYSuzukiYManabeTSurgical treatment for right ventricular perforation caused by transvenous pacing electrodes: a report of three casesSurg Today199626119339358931229
- VlaySCComplications of active-fixation electrodesPacing Clin Electrophysiol20022581153115412358162