Abstract
The number of percutaneous coronary interventions (PCI) prior to coronary artery bypass grafting (CABG) increased drastically during the last decade. Patients are referred for CABG with more severe coronary pathology, which may influence postoperative outcome. Outcomes of 200 CABG patients, collected consecutively in an observational study, were compared (mean follow-up: 5 years). Group A (n = 100, mean age 63 years, 20 women) had prior PCI before CABG, and group B (n = 100, mean age 66, 20 women) underwent primary CABG. In group A, the mean number of administered stents was 2. Statistically significant results were obtained for the following preoperative criteria: previous myocardial infarction: 54 vs 34 (P = 0.007), distribution of CAD (P < 0.0001), unstable angina: 27 vs 5 (P < 0.0001). For intraoperative data, the total number of established bypasses was 2.43 ± 1.08 vs 2.08 ± 1.08 (P = 0.017), with the number of arterial bypass grafts being: 1.26 ± 0.82 vs 1.07 ± 0.54 (P = 0.006). Regarding the postoperative course, significant results could be demonstrated for: adrenaline dosage (0.83 vs 0.41 mg/h; [p is not significant (ns)]) administered in 67 group A vs 47 group B patients (P = 0.006), and noradrenaline dosage (0.82 vs 0.87 mg/h; ns) administered in 46 group A vs 63 group B patients (P = 0.023), CK/troponine I (P = 0.002; P < 0.001), postoperative resuscitation (6 vs 0; P = 0.029), intra aortic balloon pump 12 vs 1 (P = 0.003), and 30-day mortality (9% in group A vs 1% in group B; P = 0.018). Clopidogrel was administered in 35% of patients with prior PCI and in 19% of patients without prior PCI (P = 0.016). Patients with prior PCI presented for CABG with more severe CAD. Morbidity, mortality and reoperation rate during mid term were significantly higher in patients with prior PCI.
Keywords:
Introduction
Acceptance of percutanous coronary intervention (PCI) and use in patients with symptomatic coronary artery disease (CAD) has drastically expanded during the last decade,Citation1,Citation2 whereas rates of coronary artery bypass grafting (CABG) have a decreasing tendency.Citation2,Citation3
Randomized trials conducted before and after the implementation of intracoronary stents have demonstrated comparable long-term survival between patients undergoing PCI and patients undergoing CABG for single and/or multivessel CAD.Citation4–Citation6 While PCI was offered only to patients with isolated coronary lesions and single-vessel disease years ago, it is now being used with higher frequency in a broader spectrum of patients. Consequently, a number of referred patients had received PCI, some multiple times, before undergoing CABG.
Results from medical literature comparing PCI and CABG have shown that initial PCI may lead to significantly higher rates of recurrent symptoms and redo operations than patients who undergo CABG initially.Citation7–Citation16 Although numerous studies have established that reoperative CABG is associated with increased perioperative and long-term mortality and morbidity,Citation17–Citation20 knowledge of outcomes in patients who undergo PCI prior to CABG is limited. The objective of this study was to compare the outcomes, including mortality, of group A and group B.
Patients and methods
Patient population
Two hundred patients who underwent CABG between January 2001 and June 2003 at the Department of Cardiac Surgery at the University Hospital of Munich were consecutively observed for our study. Group A included 100 patients (20 women) who had undergone PCI with the implantation of a minimum of one stent prior to CABG, at an average of 321.2 ± 501.8 days before surgery. Among them, in 70 patients, bare metal stents, and in 30 patients, drug-eluting stents were applied. The other 100 patients (group B, 20 women) were referred for primary CABG. Patients with organic valvular disease were excluded. Ethical committee approval was gained from the ethics committee of the University.
Demographic data for all patients, their classical cardiovascular risk factors and comorbidities are summarized in .
Table 1 Patient’s demographics, cardiovascular risk factors and comorbidities
In group A, additional data regarding PCI and related vessels as well as number of stent implantation in total and per vessel were documented ().
Table 2 Group A PCI details prior to CABG
Operative data including operative times, emergency status, number and kind of bypass grafts were recorded in all patients (). Data on postoperative course are displayed in . Aspects of intensive care stay, postoperative blood loss, application of blood products and catecholamines were registered. Postoperative outcomes, complications, and mortality after a follow up of 5 years were obtained. Comparison of all data in both groups was established.
Table 3 Intraoperative data
Table 4 Postoperative data
Statistical data analysis was carried out with R statistical software (http://www.r-project.org). Differences between the two groups were statistically assessed using Fisher’s exact test (for categorical variables) and the 2-sided Kolmogorov–Smirnov test (for continuous variables). The Kolmogorov–Smirnov test was applied because many variables did not fulfil, even approximately, the requirements of the t-test and the Mann–Whitney test. Multivariate analyses were performed using linear or logistic regression models, depending on the type of outcome. Statistical significance within multivariate models was assessed based on the Wald test. Overall survival was represented using Kaplan–Meier curves and the logrank test was used to compare the two groups. P-values <0.1 were marked with “ns” in –. P-values <0.05 were considered significant, whereas P-values between 0.05 and 0.1 were considered as trends.
Results
Demographic data, classic cardiovascular risk profile and comorbidities are listed in . Therapy with aspirin, GPIIb/IIIa inhibitors, ACE inhibitors, AT-I receptor blockers, calcium channel blockers, diuretics, statins, and nitrates showed an almost equal distribution among groups. Clopidogrel was administred in 35% of the patients with prior PCI and in 19% of patients without prior PCI (P = 0.016).
includes all data regarding PCI in patients of group A. Almost half of this group underwent one PCI (48%). LAD was stented in 56 patients (56%), followed by RCA in 47 patients (47%) and circumflex artery in 33%, either singly or in combination. Only 6 patients received stents in three coronary arteries. Mean duration between PCI and CABG was 321 days with a standard deviation of 502 days. This number may already show the big variance of evidence of clinical CAD symptoms.
Summarized intraoperative data for both groups are compared and listed in . All patients underwent CABG on cardiopulmonary bypass under cardioplegic hypothermic arrest. Time of extracorporeal circulation (130 vs 109 minutes; ns) revealed statistically nonsignificant differences between both groups.
The amount of blood saved by Cell Saver® was slightly lower in group B (616 ± 378 mL in group A vs 568 ± 333 mL in group B, respectively; ns). The mean number of established bypasses was 2.43 in group A vs 2.08 in group B (Fisher’s exact test: P = 0.017). Establishment of arterial bypass grafts showed the same trend: 1.26 vs 1.07 (Fisher’s exact test: P = 0.006). Left anterior descending artery was revascularized by the left interior thoracic artery (LITA) in 80% of group A patients and 89% of group B patients (ns).
Most important for outcome evaluation are postoperative parameters. Ventilation time and stay on intensive care unit did not demonstrate significant differences. Contrary to our expectation, the registered amount of bleeding 48 hours postoperatively was slightly higher in group B (1345 ± 1113 mL vs 1055 ± 842 mL in group A; ns). A mean of 2.3 units of thrombocyte concentrate was used in 34 patients of group A and 1.6 units in 22 group B patients (ns). The amount of bleeding in both groups may be related to thrombocyte dosage, especially under the circumstance of being given preoperative antiplatelet medication. Neither the amount of erythrocyte concentrate nor the amount of fresh frozen plasmas was significantly different between groups. The dosage of adrenaline was not significantly different in the two groups (0.83 vs 0.41 mg/h; ns). The difference in the mean was due to a small number of extreme values. However, the number of patients who received adrenaline was higher in group A than in group B (67 vs 47, respectively; P = 0.006). Mean noradrenaline dosage was approximately equal in the two groups (0.82 vs 0.87 mg/h; ns), and noradrenaline was administered in 46 group A vs 63 group B patients (P = 0.023). Six patients of group A were resuscitated postoperatively whereas no group B patient had to be resuscitated (P = 0.003). Myocardial markers CK and troponine I did show statistically significant differences between groups (P < 0.002; P < 0.001) with strongly higher levels in group A. Twelve group A patients needed an intraaortic balloon pump implantation postoperatively, whereas only one was implanted in patients of group B (P = 0.003).
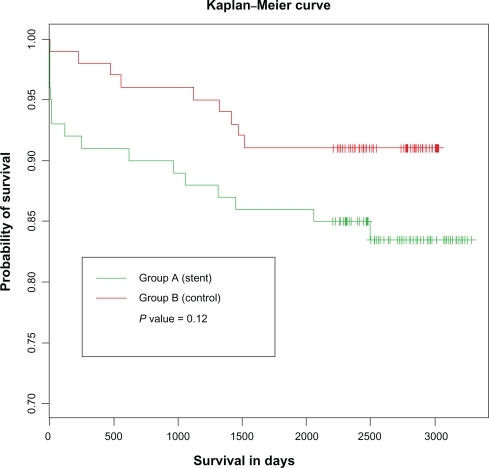
30-day mortality was 9% in group A and 1% in group B (P = 0.018). This difference may be caused by several factors that will be discussed below. The five-year mortality rate was 14% in group A vs 9% in group B (logrank-test: ns, ). Five group A patients necessitated redo-CABG vs none of group B (ns).
Figure 1 Probability of survival among study groups.
In multivariate regression analyses with age, NYHA class, ejection fraction, and CAD as adjustment factors, prior PCI was not a significant predictor of postoperative bleeding, ventilation time, stay on intensive care unit, use of thrombocyte concentrate, use of erythrocyte concentrate, or fresh frozen plasma.
Discussion
Trials comparing PCI and CABG have demonstrated that long-term survival of PCI and CABG is similar, but rates of symptom recurrence and repeated revascularization are significantly higher in patients with initial PCI.Citation10,Citation12,Citation16 With dramatic increase in PCI rates during the last decade,Citation1,Citation2 it is a consequence that the number of patients referred for CABG with a prior PCI has increased.Citation21
Kalaycioglu et alCitation22 compared 40 patients who had undergone CABG with a prior PCI with a case-matched control group of 40 patients who underwent CABG with no prior PCI. In contrast to our study, the authors found that patients with a prior PCI were younger, had a higher preoperative ejection fraction, less extensive coronary disease, and had fewer bypass grafts. After finishing this study, we agree with their results of diminished freedom from death, angina, and repeat revascularization procedure in the 36 months after surgery in patients with a prior PCI. In another study, Barakate et alCitation23 compared 361 patients who underwent CABG after initially successful PCI. Similar to the results from Hassan et alCitation24 they demonstrated that patients with a prior PCI had a higher pre-operative ejection fraction, less extensive coronary disease, and fewer bypass grafts, and were more likely to present with worsened symptoms. However, contrary to the findings from Hassan et al Barakate et al showed similar rates of in-hospital mortality between the 2 groups.
After analysis of our results, we found a stronger disease severity of CAD in group A (P < 0.0001). NYHA class distribution before surgery was significantly different among both groups (P = 0.025), 27 group A and 5 group B patients presented with unstable angina (P < 0.0001). Percentage of previous myocardial infarction differed significantly between both groups: 54% of group A and 34% of group B patients (P = 0.007). Clopidogrel was preoperatively administred in 35% of the patients with prior PCI and in 19% of patients without prior PCI (P = 0.016).
Regarding intraoperative data, statistically significant results were demonstrated for group A and group B: the mean number of established bypasses was significantly different among groups (2.43 vs 2.08, P = 0.017). The mean number of arterial bypass grafts used for revascularisation showed significant results as well (1.26 vs 1.07, P = 0.006). Left anterior descending artery was revascularized by LITA in 80% of group A patients and 89% of group B patients (ns). In search of causes for this diverse percentage of LITA graft use, we conjecture that severity of LAD calcification and placement of intracoronary stents, as well as emergency status of surgery, may be primary reasons for using this procedure.
During the postoperative course, statistically significant results could be registered for: frequency of adrenaline (P = 0.006) and noradrenaline (P = 0.023) administration, CK (P = 0.002) and troponine I (P < 0.001), and postoperative resuscitation (6 vs 0; P = 0.029). Even during perioperative duration, data leads to the supposition that the severity of disease seems to be higher and further advanced in group A. Contrary to our supposition, the amount of postoperative drainage loss was higher in group B (1345 ml) than in group A (1055 ml; ns). We expected, especially after clinical intraoperative impression, a higher bleeding rate in group A, mostly due to antiplatelet therapy. Blood product utilization, especially of thrombocyte concentrates, was higher in group A (2.3 vs 1.6 units; ns) and may be one of the reasons for limited blood loss after surgery. Rethoracotomy rates were almost equal in both groups.
Twelve patients from group A received postoperatively an intraaortic balloon pump. Only one patient of group B necessitated an intraaortic balloon pump after surgical procedure (P = 0.003).
30-day mortality was significantly lower in group B (9% vs 1%; P = 0.018). Five-year mortality was decreased in group B (14% in group A vs 9% in group B; ns). 83 patients of group A and 89 patients of group B showed NYHA class one or two after five years (ns). 16 group A patients underwent re-PCI and stent implantation vs 13 of group B (ns). 5 patients of group A and no patient of group B underwent redo-CABG (ns).
The reasons for a higher mortality in short and mid term after CABG in patients with prior PCI are not clearly understood. In our cohort, these patients had more comorbidity and increased coronary disease pathology, and presented for surgery with advanced symptoms and greater urgency. It might be that patients who had initial PCI had a more aggressive atherosclerotic onset promoting a higher rate of restenosis and/or the development of new lesions at remote coronary sites.Citation25 In addition, the application of successful PCI in these patients may have prevented the formation of protective collateral vessels, which resulted in the more acute presentation of patients who required repeated revascularization. Finally, prior PCI and, especially, stenting of a coronary lesion may have resulted in an anastomosis at a more distal site with a smaller luminal diameter and suboptimal runoff, thus compromising the degree to which the patient was completely revascularized.
Study limitations
This study has several limitations. It has been designed as a consecutive, observational, single center investigation. The number of enrolled patients limits the explanatory power of our study. Selection of patients of both groups may introduce an underlying bias.
We could not elaborate on the factors influencing the physicians’ and patients’ decisions to proceed with PCI or surgery first, noting that cardiothoracic surgeons do see patients usually after cardiologists have visited them. Even as we limited our analysis to short-term and mid-term outcomes, it is plausible that different methods of follow-up for patients treated at or outside our institution could have led to some misclassification bias. The number of enrolled patients limits the explanatory power of our investigation.
Disclosure
The authors report no conflicts of interest in this work.
References
- JamalSMShriveFMGhaliWAKnudtsonMLEisenbergMJfor Canadian Cardiovascular Outcomes Research Team (CCORT)In-hospital outcomes after percutaneous coronary intervention in Canada: 1992/93 to 2000/01Can J Cardiol20031978278912813611
- UlrichMRBrockDMZiskindAAAnalysis of trends in coronary artery bypass grafting and percutaneous coronary intervention rates in Washington state from 1987 to 2001Am J Cardiol20039283683914516888
- GhaliWAQuanHShriveFMHirschGMfor the Canadian Cardiovascular Outcomes Research Team (CCORT)Outcomes after coronary artery bypass graft surgery in Canada: 1992/93 to 2000/01Can J Cardiol20031977478112813610
- GoyJJEeckhoutEMoretCFive-year outcome in patients with isolated proximal left anterior descending coronary artery stenosis treated by angioplasty of left internal mammary artery grafting: a prospective trialCirculation1999993255325910385499
- Bypass Angioplasty Revascularization Investigation (BARI)Comparison of coronary bypass surgery with angioplasty in patients with multivessel diseaseN Engl J Med19963352172258657237
- Coronary angioplasty versus coronary artery bypass surgery: the Randomized Intervention Treatment of Angina (RITA) trialLancet19933415735808094826
- KingSBLimboNJWeintraubWSfor Emory Angioplasty versus Surgery Trial (EAST)A randomized trial comparing coronary angioplasty with coronary bypass surgeryN Engl J Med1994331104410508090163
- Coronary Angioplasty versus Bypass Revascularization Investigation Trial Participants. First-year results of CABRI (Coronary Angioplasty versus Bypass Revascularization Investigation)Lancet1995346117911847475656
- ChocronSBaillotRRouleauJLImpact of previous percutaneous transluminal coronary angioplasty and/or stenting revascularization on outcomes after surgical revascularization: insights from the imagine studyEur Heart J20082967367918285358
- HammCWReimersJIschingerTRupprechtHJBergerJBleifeldWfor German Angioplasty Bypass Surgery InvestigationA randomized study of coronary angioplasty compared with bypass surgery in patients with symptomatic multivessel coronary diseaseN Engl J Med1994331103710438090162
- MorrisonDASethiGSacksJfor Investigators of the Department of Veterans Affairs Cooperative Study #385, the Angina with Extremely Serious Operative Mortality Evaluation (AWESOME)Percutaneous coronary intervention versus coronary artery bypass graft surgery for patients with medically refractory myocardial ischemia and risk factors for adverse outcomes with bypass: a multicenter, randomized trialJ Am Coll Cardiol20013814314911451264
- RodriguezABernardiVNaviaJfor ERACI II InvestigatorsArgentine Randomized Study: Coronary Angioplasty with Stenting Versus Coronary Artery Bypass Surgery in patients with Multiple-Vessel Disease (ERACI II): 30-day and one-year follow-up resultsJ Am Coll Cardiol200137515811153772
- RodríguezAERodríguez AlemparteMCoronary stenting versus coronary bypass surgery in patients with multiple vessel disease and significant proximal LAD stenosis: results from the ERACI II studyHeart20038918418812527674
- The SoS investigatorsCoronary artery bypass surgery versus percutaneous coronary intervention with stent implantation in patients with multivessel coronary artery disease (the Stent or Surgery trial): a randomized controlled trialLancet200236096597012383664
- DrenthDJVeegerNJWinterJBA prospective randomized trial comparing stenting with off-pump coronary surgery for high-grade stenosis in the proximal left anterior descending coronary artery: three-year follow-upJ Am Coll Cardiol2002401955196012475455
- SerruysPWUngerFSousaJEfor Arterial Revascularization Therapies Study GroupComparison of coronary-artery bypass surgery and stenting for the treatment of multivessel diseaseN Engl J Med20013441117112411297702
- SalomonNWPageUSBigelowJCKrauseAHOkiesJEMetzdorffMTReoperative coronary surgery. Comparative analysis of 6591 patients undergoing primary bypass and 508 patients undergoing reoperative coronary artery bypassJ Thorac Cardiovasc Surg19901002502592385122
- ChristensonJTSchmuzigerMSimonetFReoperative coronary artery bypass procedures: risk factors for early mortality and late survivalEur J Cardiothorac Surg1997111291339030801
- SchmuzigerMChristensonJTMauriceJMosimannESimonetFVelebitVReoperative myocardial revascularization: an analysis of 458 reoperations and 2645 single operationsCardiovasc Surg199426236297820526
- YauTMBorgerMAWeiselRDIvanovJThe changing pattern of reoperative coronary surgery: trends in 1230 consecutive operationsJ Thorac Cardiovasc Surg200012015616310884669
- AbramovDTamarizMGFremesSETrends in coronary artery bypass surgery results: a recent, 9-year studyAnn Thorac Surg200070849010921687
- KalayciogluSSinciVOktarLCoronary artery bypass grafting (CABG) after successful percutaneous transluminal coronary angioplasty (PCI): is PCI a risk for CABGInt Surg1998831901939870771
- BarakateMSHemliJMHughesCFBannonPGHortonMDCoronary artery bypass grafting (CABG) after initially successful percutaneous transluminal coronary angioplasty (PCI): a review of 17 years experienceEur J Cardiothorac Surg20032317918612559340
- HassanAButhKJBaskettRJFThe association between prior percutaneous coronary intervention and short-term outcomes after coronary artery bypass graftingAmerican Heart Journal20031501026103116290991
- JohnsonRGSiroisCThurerRLPredictors of CABG within one year of successful PCI: a retrospective, case-control studyAnn Thorac Surg19974389236327