Abstract
Coronary artery calcium (CAC) is an integral part of atherosclerotic coronary heart disease (CHD). CHD is the leading cause of death in industrialized nations and there is a constant effort to develop preventative strategies. The emphasis is on risk stratification and primary risk prevention in asymptomatic patients to decrease cardiovascular mortality and morbidity. The Framingham Risk Score predicts CHD events only moderately well where family history is not included as a risk factor. There has been an exploration for new tests for better risk stratification and risk factor modification. While the Framingham Risk Score, European Systematic Coronary Risk Evaluation Project, and European Prospective Cardiovascular Munster study remain excellent tools for risk factor modification, the CAC score may have additional benefit in risk assessment. There have been several studies supporting the role of CAC score for prediction of myocardial infarction and cardiovascular mortality. It has been shown to have great scope in risk stratification of asymptomatic patients in the emergency room. Additionally, it may help in assessment of progression or regression of coronary artery disease. Furthermore, the CAC score may help differentiate ischemic from nonischemic cardiomyopathy.
Background
Coronary heart disease (CHD) is the leading cause of death in industrialized countries. Cardiovascular mortality in the US alone is close to a million per year. This problem is on the rise, in view of the increasing number of elderly people in the US and worldwide. By 2020, there will be more than 50 million people aged older than 65 years in the US alone. Continuous efforts are being made to develop preventative strategies for CHD. Cardiovascular risk stratification by primary risk assessment is a key step towards this goal. Traditional risk assessment is based on the Framingham Risk Score (FRS) which was developed based on clinical research in men and women from Framingham, Massachusetts, followed over three generations. This evaluation was done to understand better the causes of cardiovascular disease. There have been at least 1973 publications in peer-reviewed journals up until 2008. This has led to risk factor stratification and modification measures in cardiovascular practice. This risk stratification is based on the Framingham Heart Study (FHS, see http://www.framinghamheartstudy.org) in the US, the European Systematic Coronary Risk Evaluation (SCORE) study,Citation1 and the Prospective Cardiovascular Munster (PROCAM) study in Germany.Citation2 Each of these studies documents a 10-year risk for cardiovascular events which dictates public policies, and the intensity of treatment generally depends upon the risk stratification.
Cardiac risk assessment
Unfortunately, traditional risk factor assessment has a very poor sensitivity and specificity to predict coronary events. In the past, exercise stress testing was performed to diagnose coronary artery disease (CAD) in asymptomatic patients and it is not currently recommended as a screening test.Citation3 At least 25% of patients with CHD have asymptomatic presentation with nonfatal myocardial infarction (MI) or sudden death, and therefore there is a constant need for improvement of risk stratification measures.Citation4 The American Heart Association (AHA) Prevention V Conference emphasized going beyond secondary prevention and addressed ways to identify risk in asymptomatic patients to justify more intensive risk reduction.Citation5
It is common to address this clinical risk assessment as an initial step and also recognize CHD risk equivalents, as shown in and . National Cholesterol Education Program (NCEP) guidelines have classified patients into different categories, depending upon the presence of CHD or risk factors for 10-year risk of fatal CHD or nonfatal MI, as illustrated in .
Table 1 Risk factors contributing to 10-year risk of CHD
Table 2 Coronary heart risk equivalents
Table 3 Framingham risk score
The NCEP targets high-risk groups for risk factor modification, and intermediate-risk groups may need further risk stratification. Furthermore, intermediate-risk groups may be deemed to be high-risk based on the presence of coronary artery calcium (CAC) requiring aggressive intervention. Several investigators have investigated use of the CAC score to risk stratify patients further. Current clinical practice for risk stratification is based on several clinical guidelines.Citation6,Citation7
Each risk factor has points, and based on their accumulated points, patients fall into categories of low-, moderate-, to high-risk groups for CHD. The risk score was developed based on risk factors such as total cholesterol, high-density lipoprotein cholesterol (HDL-C), blood pressure, age, smoking, and gender. Based on these risk factor scores, the risk for CHD can be classified from low- to high-risk, and one can estimate the 10-year likelihood of developing a major cardiac event, as shown in . Low-risk CHD correlates with 10% mortality at 10 years, moderate-risk with 10%–20%, and high-risk with greater than 20% risk of mortality. This can readily be calculated by using an online Framingham risk calculator at http://hp2010.nhlbihin.net/ATPiii/calculator.asp?usertype=prof; http://www.framinghamheartstudy.org/risk/hrdcoronary.html.
Framingham heart study
The FRS uses traditional risk factors to predict risk of coronary events in people without known CAD.Citation8,Citation9 This cardiac risk assessment is based on the FHS, which is an ongoing study for more than 50 years leading to several publications. This historical study has participation of three generations, and a careful analysis of the initial cohort and subsequent two generations has led to identification of major cardiovascular risk factors. This had led to the achievement of several milestones in the management of cardiovascular disease. One of the milestones achieved in 1998 was risk prediction, with an algorithm based on the presence of various risk factors. There have been numerous discussions on FRS calculation on risk assessment in asymptomatic patients which can be found on the Framingham website and the National Heart Lung and Blood Institute websites. The risk score classifies patients into high-risk, intermediate-risk, and low-risk for CHD, as shown in .
European PROCAM study
In the US, the FHS provides the extensively validated risk assessment by a multivariable scoring system for major cardiovascular endpoints. This scoring system includes major risk factors such as age, gender, total cholesterol, HDL-C, hypertension (or on treatment for hypertension), and cigarette smoking. While family history was not included as a risk factor in FHS, other studies, ie, SCORE and PROCAM,Citation1,Citation2 have included age, gender, low-density lipoprotein cholesterol (LDL-C), HDL-C, triglycerides, systolic blood pressure (BP), cigarette smoking, family history of premature CHD, and presence or absence of diabetes mellitus. PROCAM was a large epidemiological cohort study, developed from data for more than 26,000 subjects in Germany over a period of 25 yearsCitation2 which helped to develop a cardiovascular risk calculator. Risk can be calculated on the PROCAM website by a simplified version of the PROCAM risk calculator, which is an International Task Force for Prevention of Coronary Heart disease (http://www.chd-taskforce.com/procam_interactive.html).
European SCORE study
SCORE was developed for cardiovascular risk stratification in European clinical practice to calculate the 10-year risk for CHD and noncoronary cardiovascular disease. This score system was based on data collected from a large cohort of 205,178 subjects from 12 European countries.Citation1
WHO MONICA project
The concept of risk stratification was born after the FHS. There was a need for long-term monitoring of mortality, morbidity, and risk factors in clinical practice. The Multinational Monitoring of Trends and Determinants in Cardiovascular Diseases (MONICA)Citation10 project was established to monitor trends in cardiovascular disease around the world. This project showed major changes in survival, driven by changes in coronary event rates, which further emphasize the need for risk factor modification tools.
Incremental risk stratification by CAC score
While the FRS and PROCAM remain excellent tools for risk factor modification, the CAC score may have additional benefit in risk assessment. Atherosclerotic plaque passes through several stages of plaque rupture and healing, followed by calcification. Thus, the presence of calcium can be considered an advanced marker of CHD. There have been numerous studies supporting the role of CAC score for prediction of MI and cardiovascular death. CAC clearly adds to the predictive value of traditional risk factors. While spotty calcification has been considered a marker of vulnerable plaque,Citation11 the relationship between the presence and amount of calcium in an individual coronary artery found on coronary angiography to predict cardiovascular events is uncertain.Citation12 It is most likely that the co-occurrence of calcified and non-calcified plaques may determine progression of CHD.Citation13
Role of CAC score in primary prevention
In 1996 and subsequently in 2000, AHA consensus documentsCitation14,Citation15 have stated that “CAC is a part of development of CAD and occurs exclusively in atherosclerotic CAD and is absent in normal arteries”. CAC plaque documents the presence of CAD in an individual patient as compared with just the presence of risk factors. Detection of asymptomatic CAD has been of great interest since the publication of the Screening for Heart Attack Prevention and Education (SHAPE).Citation16 Moreover, detection of vulnerable plaque leading to coronary events is of paramount importance. The role of CAC in identification of vulnerable plaque is unknown.Citation17 Spotty calcification has been shown to identify patients with vulnerable plaque.Citation11 This may be due to noncalcified plaque on the shoulders of calcified plaque.
CHD risk assessment with CAC score in asymptomatic patients
The important risk factor, ie, positive family history, is not included in risk stratification by the FRS. Because FRS predicts CHD events only moderately well, there has been an exploration for better risk stratification tests so that patients may benefit from aggressive risk factor modification.Citation5–Citation7 This can be accomplished by CAC scoring. There have been a large number of studies showing the prognostic value of the CAC score in 2000–2009,Citation18–Citation24 leading to great interest in this score.
While initially there were conflicting data about the prognostic value of the CAC score, this was addressed by Arad et al in 2000 in 1172 subjects by multivariate analysis.Citation25 The purpose of this study was to evaluate the prognostic accuracy of a high CAC score with electron-beam computed tomography (CT). During an average 3.6 year follow-up in this study, 39 subjects had coronary events, which included nonfatal MI in 15, coronary artery revascularization in 21, and coronary death in three. Based on these data, it was concluded that electron-beam CT predicts coronary events. Kondos et alCitation26 also demonstrated the added value of CAC score in a largest retrospective study of 8855 self-referred men and women without prior cardiovascular events. Follow-up was available in 5634 (64%) at 37 ± 13 months for 4151 men and 1484 women, and showed incremental prognostic information in addition to conventional risk factors.
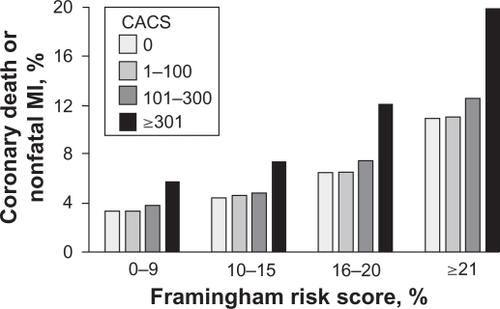
Greenland et alCitation20 examined the incremental prognostic value of the CAC score in addition to traditional risk factors in a prospective observational study. This was a population-based study of 1461 asymptomatic adults with traditional coronary risk factors assessed by FRS. These participants were screened from 1990–1992 and had initial FRS and CAC scores. They were contacted yearly up to 8.5 years after the initial CAC test for nonfatal MI and/or CHD-related death. This study evaluated whether FRS and CAC score predicted all-cause mortality, which was stratified by four levels of FRS and four levels of CAC score, as illustrated in . FRS categories are the estimated 10-year risk of CHD (death or nonfatal MI) events based on FRS. In this study, CAC score alone was able to predict CHD risk independently of FRS. Moreover, CAC score significantly modified the risk prediction in all categories of FRS category with risk >10% (ie, 10-year risk of CHD events >10%).
Figure 1 Predicted seven-year event rate from Cox regression model for CHD death or nonfatal MI for different categories of FRS or CAC score. The event rates are stratified by four levels of FRS and four different levels of calcium score. Analysis showed a statistically significant difference between and calcium >300 and other groups for FRS categories >10% CHD risk. Copyright © 2004, American Medical Association. All rights reserved. Adapted with permission from Greenland P, LaBree L, Azen SP, Doherty TM, Detrano RC. Coronary artery calcium score combined with Framingham score for risk prediction in asymptomatic individuals. JAMA. 2004;291(2):210–215.
Another large study by Lamont et alCitation24 reported a follow-up on 11,000 patients who underwent screening medical examination including CAC score during 1995–2000. In a mean follow-up of 3.5 years in asymptomatic men and women, CHD events (nonfatal MI and CHD-related deaths) were higher with a CAC score >400. The Prospective Army Coronary Calcium Project (PACC)Citation22 showed the independent prognostic value of CAC score in young asymptomatic men and women of mean age 43 years. This study showed that the presence of CAC was associated with an 11.8-fold increased risk of coronary events in a three-year follow-up of men aged 40–45 years.
The Rotterdam Coronary Calcification StudyCitation23 addressed the role of the CAC score in elderly patients. This was a prospective, population-based study in 1795 patients comparing patients with CAC <100 with those having CAC of 101–400, CAC 401–1000, and CAC >1000. CAC score was found to be a strong and independent predictor of future events, as illustrated in and . Different CAC score categories also predicted survival free of a CHD event and cardiovascular disease events, as shown in .
Figure 2 Event rate according to calcium score category. Copyright © 2005, American Heart Association. All rights reserved. Adapted with permission from Vliegenthart R, Oudkerk M, Hotman A, et al. Coronary calcification improves cardiovascular risk prediction in the elderly. Circulation. 2005;112(4):572–577.
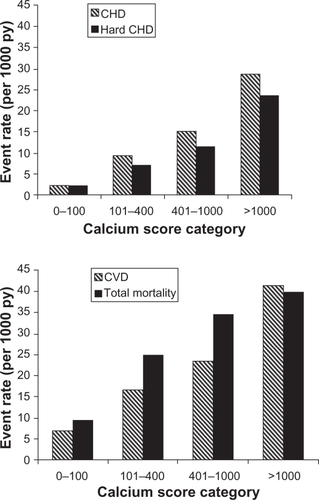
Figure 3 Survival curves, free of CHD A) and CVD B) events, according to calcium score. Copyright © 2005, American Heart Association. All rights reserved. Adapted with permission from Ehara S, Kobayashi Y, Yoshiyama M, et al. Circulation. 2005;112: 572–577.
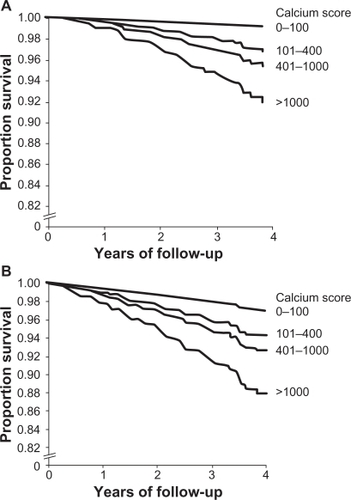
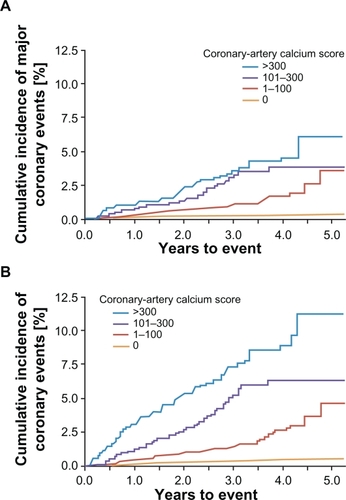
Bild et alCitation27 showed that CAC is influenced by age, gender, and ethnicity. The role of CAC score in different ethnic groups for incremental risk prediction was examined in the Multi-Ethnic Study of Atherosclerosis (MESA).Citation28 MESA was a population-based study which enrolled subjects of four different ethnic groups from six sites across the US. Data on CHD risk factors and CAC scores in different ethnic groups were followed for an average period of 3.8 years. Patients had comprehensive risk assessment with every possible test and were followed from 2000 onwards. This study showed that doubling of CAC score increased the risk of a major cardiovascular event, such as death and MI. Risk of any coronary events or major events was independent of other risk factors. CAC score was found to be highly predictive of cardiovascular risk in all the four ethnic groups and it contributed to the risk of both major coronary events (, Panel A) and any coronary events (, Panel B). CAC score alone was better than all the other risk factors combined for risk prediction.
Figure 4 Unadjusted Kaplan–Meier cumulative event curve for coronary events among participants with calcium score 0, 1–100, 101–300, and >300. Panel A shows the rate of major coronary events (MI and death from CHD); Panel B shows the rates for any coronary event. Differences between all curves are statistically significant. Copyright © 2008, Massachusetts Medical Society. All right reserved. Adapted with permission from Detrano R, Guerci AD, Carr JJ, et al. N Engl J Med. 2008:358: 1336–1345.
This clearly demonstrated that CAC score is a strong predictor for the risk of developing clinical CHD. It provides a risk prediction beyond the standard risk prediction of the FRS. This risk prediction by CAC scoring was also demonstrated in different ethnic groups, including white, black, Hispanic, and Chinese in the MESA trial. Based on this study, there is a risk calculator based on age, gender, ethnicity and other risk factors, known as the MESA risk calculator, where an individual’s CAD risk can be calculated relative to that of peers (http://www.mesa-nhlbi.org/Calcium/input.aspx).
Role of CAC in symptomatic patients
In symptomatic patients, the CAC score has been evaluated as a noninvasive tool to diagnose obstructive CAD, and this was published as an ACC/AHA consensus document.Citation29,Citation30 This document examined 3683 symptomatic patients in 16 studies for evaluation of diagnostic accuracy of CAC scoring in patients referred for cardiac catheterization. Higher CAC score increased the likelihood of detecting significant CAD with greater than 50% stenosis. Guerci et alCitation31 showed the relationship of CAC score to CAD in 290 symptomatic patients undergoing cardiac catheterization for approved clinical indications. A CAC score of 80 was not associated with any likelihood of CAD, regardless of number of risk factors and a CAC of 170 or more was associated with an increased likelihood of obstructive CAD (P < 0.001). Similarly, Kennedy et al have shown that CAC score had a correlation with the extent of CAD, and was found be a better discriminator than other risk factors. A substudy from the MESA cohort analyzed the relationship between extent of CAC and severity of stenosis, and showed a significant association between the extent of CAC and mean degree of stenosis in individual coronary vessels.Citation32 Schmermund et alCitation33 also showed the CAC score to be a better discriminator which improved diagnostic accuracy over conventional risk factors. A multicenter trial in 1851 patients reported the role of ultrafast CT for diagnosis of CAD in symptomatic patients who underwent cardiac catheterization. In this study, a CAC score of 80 or more had a sensitivity of 79% and specificity of 72%,Citation34 whereas the other large studyCitation35 used a cutoff CAC score of 100, leading to improved sensitivity of 95% and specificity of 79%.Citation35 Nieman et alCitation36 investigated the value of CAC detection on CT coronary angiography in comparison with exercise testing and CT coronary angiography to detect obstructive CAD. This study showed that lack of coronary calcium was a reliable means to exclude obstructive CAD.Citation36
Role of CAC score in the emergency room
Absence of CAC or minimal CAC predicted a very low incidence of future cardiac events in asymptomatic patients,Citation18,Citation25,Citation37,Citation38 symptomatic patients, and symptomatic patients undergoing cardiac catheterization.Citation39,Citation40 Several studies have shown the value of the CAC score in emergency room (ER) patients with a negative electrocardiogram (ECG) and negative cardiac enzymes as a triage tool with a very high negative predictive value.Citation41,Citation42 Georgiou et alCitation42 performed electron beam CT in 192 patients with chest pain and then followed them up for 50 ± 10 months. Among this cohort, 30% showed a graded relationship between all cardiac events and CAC score. This study showed that CAC score used as a triage test had a sensitivity of 97% and a negative predictive value of 99%. Patients without CAC (zero score) had a 0.6/year future cardiovascular event rate. Furthermore, recent studies have shown that CAC score may be a useful tool in the ER for risk stratification of patients with an acute coronary syndrome. Several other studies have demonstrated a significant correlation between CAC score and overall coronary artery atherosclerotic plaque, with a high sensitivity >95% and a high negative predictive value of >95%.Citation13,Citation43–Citation45
Role of CAC score in triage of chest pain
Several studies have shown that CAC score may be a rapid and effective triage tool in ER patients with chest pain and nonspecific ECG abnormalities.Citation41,Citation42 The high sensitivity and high negative predictive value of the CAC score may allow early discharge of such patients. One study with long-term follow-up showed that a CAC of zero represented a very low risk for cardiovascular events.Citation42 Therefore, absence of CAC may be used as an effective screening tool before undertaking invasive coronary angiography. A CAC score of less than 100 predicts a low risk, with a less than 2% chance of an abnormal perfusion nuclear study,Citation46,Citation47 and a less than 3% probability of obstructive CAD.Citation34,Citation35
CAC score to evaluate progression or regression
Does modulation of cardiac risk factors translate into regression of CAC score? Pathological studies have showed that a positive CAC score represents calcium in plaque which is an end result of healing of ruptured plaque. The process is complex, and drug therapy may have the potential to alter this fundamental process of calcification in the progression of atherosclerotic plaque. There are several factors in the progression of CAD, and the CAC score may be of biologic relevance. Serial CAC scoring may help monitor plaque regression by medical therapy.Citation48 One needs to be mindful about the intertest variability in CAC score and have confidence in this to monitor regression or progression. Many studies have shown interscan variability of CAC score by 25%–50%,Citation49–Citation51 but using the same protocol this can be reduced to 10%–15%.Citation51,Citation52 Given that the annual progression of CAC is about 20%,Citation49–Citation51 the standard protocol will allow the detection of progression. This may have a bearing on management of the intermediate-risk group category with a high CAC score.
Several reports have shown CAC progression associated with increased risk of cardiovascular events and a stable CAC score associated with lower risk of cardiovascular events.Citation19,Citation53,Citation54 In the presence of definite CAC score progression (>15%) there was a significant relative risk of MI compared with patients having a stable score. Based on these findings, a serial CAC score is an attractive strategy for monitoring progression or regression of CAD. CAC regression has been demonstrated with pharmacologic interventions such as statins.Citation55 Due to both cost issues and radiation concerns, serial monitoring of progression or regression of CAD using CAC scoring is not recommended at this time.
CAC score in diagnosis of cardiomyopathy
Technical ease and standardization of CAC score may play a role in the evaluation of the etiology of cardiomyopathy. Clinical manifestations of ischemic and nonischemic cardiomyopathy are similar and often require invasive testing, such as cardiac catheterization for final diagnosis. The role of electron beam CT was tested in a prospective, double-blind studyCitation56 with a 99% sensitivity for ischemic cardiomyopathy. The specificity for nonischemic cardiomyopathy was 92% for a CAC score of <80% and 83% for a CAC score of zero.
Technique and radiation issues
Radiographically, CAC provides an estimate of CAD burden. The most frequently used measure of CAC in the literature is the Agatston scoreCitation57 which measures the amount of calcium in each lesion. Total CAC is the sum of the scores of all the calcified lesions in all the vessels.
This could be done with electron-beam CT or multi-detector CT available in most hospitals. There is no difference in CAC measured by electron-beam CT or multi-detector CT.Citation58 A stack of cardiac images are obtained in an axial mode and calcified plaque is identified. This calcified plaque image is seen as white dots which are picture elements or pixels with an underlying number called Hounsfield Units (HU). Based on the HU numbers assigned to a pixel and its volume, we arrive at a CAC score. Just like a value for hypertension, a HU value above 129 is considered dense enough to call it calcified and a weight factor is assigned, based on this number, to quantify the density. It is a simple procedure whereby the patient is brought into the room, placed in the scanner, and the whole heart is scanned. The patient goes through few breathing exercises and there is no need to have heart rate control for the test. Images with a slice thickness of 2.5 mm are obtained with either triggered or prospective ECG gating. With the prospective gating the radiation is as low as 1 milliSievert (mSv).
Radiation exposure
Radiation exposure during CAC scoring is as low as 1.0–1.3 mSv with electron-beam CTCitation59 and 3 mSv with multi-detector CT using retrospective gated scanning, which could be reduced to 1 mSv in prospective gating by multi-detector CT.Citation60 Any amount of radiation should be a concern and the “as low as reasonably achievable” (ALARA) principle should be used. This fact is underscored by a recent publication whereby current CT scan use for various studies is expected to contribute to a large number of future malignancies, which were estimated to be up to 29,000 on the basis of all the CT scans done in 2007.Citation61 Given the carcinogenic potential of radiation, health care workers who prescribe it must be fully aware of radiation risks. They should have a full understanding of the effective dose concept which is a standard of measure of exposure expressed in mSv. Effective dose is the sum of weighted equivalent doses in all the organs and tissues during a particular scan. Due to higher doses delivered to lungs and female breast in coronary CT angiography, there is a higher carcinogenic effect on these organs. This risk is higher in younger patients and more in women than in men.
Summary
CAC is an integral part of development of CAD. Therefore, CAC scoring may be a valuable noninvasive imaging modality to do cardiac risk stratification in asymptomatic patients for cardiovascular risk. It is uncertain if CAC scoring will be cost-effective in a population-based strategy. However, it certainly helps clinicians in the aggressive management of CAD in asymptomatic patients. The CAC score is a strong predictor of CHD incidence, and provides predictive information beyond the traditional risk factors in different ethnic groups.
Disclosure
The authors report no conflicts of interest in this work.
References
- ConroyRMPyoralaKFitzgeraldAPEstimation of ten-year risk of fatal cardiovascular disease in Europe: The SCORE projectEur Heart J20032411987100312788299
- AssmannGSchulteHThe Prospective Cardiovascular Munster (PROCAM) study: Prevalence of hyperlipidemia in persons with hypertension and/or diabetes mellitus and the relationship to coronary heart diseaseAm Heart J19881166 Pt 2171317243202078
- GibbonsRJBaladyGJBeasleyJWACC/AHA Guidelines for Exercise Testing A report of the American College of Cardiology/American Heart AssociationTask Force on Practice Guidelines (Committee on Exercise Testing)J Am Coll Cardiol19973012603119207652
- GreenlandPSmithSCJrGrundySMImproving coronary heart disease risk assessment in asymptomatic people: Role of traditional risk factors and noninvasive cardiovascular testsCirculation2001104151863186711591627
- SmithSCJrGreenlandPGrundySMAHA Conference Proceedings Prevention conference V: Beyond secondary prevention: Identifying the high-risk patient for primary prevention: Executive summary. American Heart AssociationCirculation2000101111111610618313
- Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III)JAMA2001285192486249711368702
- ChobanianAVBakrisGLBlackHRThe Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: The JNC 7 reportJAMA2003289192560257212748199
- WilsonPWD’AgostinoRBLevyDBelangerAMSilbershatzHKannelWBPrediction of coronary heart disease using risk factor categoriesCirculation19989718183718479603539
- D’AgostinoRBSrGrundySSullivanLMWilsonPValidation of the Framingham coronary heart disease prediction scores: Results of a multiple ethnic groups investigationJAMA2001286218018711448281
- Tunstall-PedoeHKuulasmaaKMahonenMTolonenHRuokokoskiEAmouyelPContribution of trends in survival and coronary-event rates to changes in coronary heart disease mortality: 10-year results from 37 WHO MONICA project populations. Monitoring trends and determinants in cardiovascular diseaseLancet199935391641547155710334252
- EharaSKobayashiYYoshiyamaMSpotty calcification typifies the culprit plaque in patients with acute myocardial infarction: An intravascular ultrasound studyCirculation2004110223424342915557374
- BeckmanJAGanzJCreagerMAGanzPKinlaySRelationship of clinical presentation and calcification of culprit coronary artery stenosesArterioscler Thromb Vasc Biol200121101618162211597935
- RumbergerJASimonsDBFitzpatrickLASheedyPFSchwartzRSCoronary artery calcium area by electron-beam computed tomography and coronary atherosclerotic plaque area. A histopathologic correlative studyCirculation1995928215721627554196
- GreenlandPBonowROBrundageBHACCF/AHA 2007 clinical expert consensus document on coronary artery calcium scoring by computed tomography in global cardiovascular risk assessment and in evaluation of patients with chest pain: A report of the American College of Cardiology Foundation Clinical Expert Consensus Task Force (ACCF/AHA Writing Committee to Update the 2000 Expert Consensus Document on Electron Beam Computed Tomography) developed in collaboration with the Society of Atherosclerosis Imaging and Prevention and the Society of Cardiovascular Computed TomographyJ Am Coll Cardiol200749337840217239724
- GreenlandPBonowROBrundageBHACCF/AHA 2007 clinical expert consensus document on coronary artery calcium scoring by computed tomography in global cardiovascular risk assessment and in evaluation of patients with chest pain: A report of the American College of Cardiology Foundation Clinical Expert Consensus Task Force (ACCF/AHA Writing Committee to Update the 2000 Expert Consensus Document on Electron Beam Computed Tomography)Circulation2007115340242617220398
- NaghaviMFalkEHechtHSFrom vulnerable plaque to vulnerable patient – Part III: Executive summary of the Screening for Heart Attack Prevention and Education (SHAPE) Task Force reportAm J Cardiol2006982A2H15H
- FalkEShahPKFusterVCoronary plaque disruptionCirculation19959236576717634481
- O’MalleyPGTaylorAJJacksonJLDohertyTMDetranoRCPrognostic value of coronary electron-beam computed tomography for coronary heart disease events in asymptomatic populationsAm J Cardiol200085894594810760331
- RaggiPCallisterTQShawLJProgression of coronary artery calcium and risk of first myocardial infarction in patients receiving cholesterol-lowering therapyArterioscler Thromb Vasc Biol20042471272127715059806
- GreenlandPLaBreeLAzenSPDohertyTMDetranoRCCoronary artery calcium score combined with Framingham score for risk prediction in asymptomatic individualsJAMA2004291221021514722147
- AradYGoodmanKJRothMNewsteinDGuerciADCoronary calcification, coronary disease risk factors, C-reactive protein, and atherosclerotic cardiovascular disease events: The St Francis Heart StudyJ Am Coll Cardiol200546115816515992651
- TaylorAJBindemanJFeuersteinICaoFBrazaitisMO’MalleyPGCoronary calcium independently predicts incident premature coronary heart disease over measured cardiovascular risk factors: Mean three-year outcomes in the Prospective Army Coronary Calcium (PACC) projectJ Am Coll Cardiol200546580781416139129
- VliegenthartROudkerkMHofmanACoronary calcification improves cardiovascular risk prediction in the elderlyCirculation2005112457257716009800
- LaMonteMJFitzGeraldSJChurchTSCoronary artery calcium score and coronary heart disease events in a large cohort of asymptomatic men and womenAm J Epidemiol2005162542142916076829
- AradYSpadaroLAGoodmanKNewsteinDGuerciADPrediction of coronary events with electron beam computed tomographyJ Am Coll Cardiol20003641253126011028480
- KondosGTHoffJASevrukovAElectron-beam tomography coronary artery calcium and cardiac events: A 37-month follow-up of 5635 initially asymptomatic low- to intermediate-risk adultsCirculation2003107202571257612743005
- BildDEDetranoRPetersonDEthnic differences in coronary calcification: The Multi-Ethnic Study of Atherosclerosis (MESA)Circulation2005111101313132015769774
- DetranoRGuerciADCarrJJCoronary calcium as a predictor of coronary events in four racial or ethnic groupsN Engl J Med2008358131336134518367736
- O’RourkeRABrundageBHFroelicherVFAmerican College of Cardiology/American Heart AssociationExpert Consensus document on electron-beam computed tomography for the diagnosis and prognosis of coronary artery diseaseCirculation2000102112614010880426
- O’RourkeRABrundageBHFroelicherVFAmerican College of Cardiology/American Heart AssociationExpert Consensus Document on electron-beam computed tomography for the diagnosis and prognosis of coronary artery diseaseJ Am Coll Cardiol200036132634010898458
- GuerciADSpadaroLAGoodmanKJComparison of electron beam computed tomography scanning and conventional risk factor assessment for the prediction of angiographic coronary artery diseaseJ Am Coll Cardiol19983236736799741510
- RosenBDFernandesVMcClellandRLRelationship between baseline coronary calcium score and demonstration of coronary artery stenoses during follow-up MESA (Multi-Ethnic Study of Atherosclerosis)JACC Cardiovasc Imaging20092101175118319833306
- SchmermundABaileyKRRumbergerJAReedJESheedyPF2ndSchwartzRSAn algorithm for noninvasive identification of angiographic three-vessel and/or left main coronary artery disease in symptomatic patients on the basis of cardiac risk and electron-beam computed tomographic calcium scoresJ Am Coll Cardiol19993324444529973025
- BudoffMJDiamondGARaggiPContinuous probabilistic prediction of angiographically significant coronary artery disease using electron beam tomographyCirculation2002105151791179611956121
- HaberlRBeckerALeberACorrelation of coronary calcification and angiographically documented stenoses in patients with suspected coronary artery disease: Results of 1,764 patientsJ Am Coll Cardiol200137245145711216962
- NiemanKGalemaTWNeefjesLAComparison of the value of coronary calcium detection to computed tomographic angiography and exercise testing in patients with chest painAm J Cardiol2009104111499150419932782
- RaggiPCallisterTQCooilBIdentification of patients at increased risk of first unheralded acute myocardial infarction by electron-beam computed tomographyCirculation2000101885085510694523
- WongNDHsuJCDetranoRCDiamondGEisenbergHGardinJMCoronary artery calcium evaluation by electron beam computed tomography and its relation to new cardiovascular eventsAm J Cardiol200086549549811009264
- TatumJLJesseRLKontosMCComprehensive strategy for the evaluation and triage of the chest pain patientAnn Emerg Med19972911161258998090
- ReillyBMEvansATSchaiderJJImpact of a clinical decision rule on hospital triage of patients with suspected acute cardiac ischemia in the emergency departmentJAMA2002288334235012117399
- McLaughlinVVBaloghTRichSUtility of electron beam computed tomography to stratify patients presenting to the emergency room with chest painAm J Cardiol1999843327328A32810496445
- GeorgiouDBudoffMJKauferEKennedyJMLuBBrundageBHScreening patients with chest pain in the emergency department using electron beam tomography: A follow-up studyJ Am Coll Cardiol200138110511011451257
- SimonsDBSchwartzRSEdwardsWDSheedyPFBreenJFRumbergerJANoninvasive definition of anatomic coronary artery disease by ultrafast computed tomographic scanning: A quantitative pathologic comparison studyJ Am Coll Cardiol1992205111811261401612
- RumbergerJASchwartzRSSimonsDBSheedyPF3rdEdwardsWDFitzpatrickLARelation of coronary calcium determined by electron beam computed tomography and lumen narrowing determined by autopsyAm J Cardiol19947316116911738203333
- KaufmannRBPeyserPASheedyPFRumbergerJASchwartzRSQuantification of coronary artery calcium by electron beam computed tomography for determination of severity of angiographic coronary artery disease in younger patientsJ Am Coll Cardiol19952536266327860906
- HeZXHedrickTDPrattCMSeverity of coronary artery calcification by electron beam computed tomography predicts silent myocardial ischemiaCirculation2000101324425110645919
- BermanDSWongNDGransarHRelationship between stress-induced myocardial ischemia and atherosclerosis measured by coronary calcium tomographyJ Am Coll Cardiol200444492393015312881
- WatersDHigginsonLGladstonePEffects of monotherapy with an HMG-CoA reductase inhibitor on the progression of coronary atherosclerosis as assessed by serial quantitative arteriography. The Canadian Coronary Atherosclerosis Intervention TrialCirculation19948939599688124836
- SchmermundABaumgartDMohlenkampSNatural history and topographic pattern of progression of coronary calcification in symptomatic patients: An electron-beam CT studyArterioscler Thromb Vasc Biol200121342142611231923
- BudoffMJLaneKLBakhsheshiHRates of progression of coronary calcium by electron beam tomographyAm J Cardiol200086181110867084
- MaherJEBielakLFRazJASheedyPF2ndSchwartzRSPeyserPAProgression of coronary artery calcification: A pilot studyMayo Clin Proc199974434735510221462
- MaoSBakhsheshiHLuBLiuSCOudizRJBudoffMJEffect of electrocardiogram triggering on reproducibility of coronary artery calcium scoringRadiology2001220370771111526270
- RaggiPCooilBShawLJProgression of coronary calcium on serial electron beam tomographic scanning is greater in patients with future myocardial infarctionAm J Cardiol200392782782914516885
- RaggiPCooilBRattiCCallisterTQBudoffMProgression of coronary artery calcium and occurrence of myocardial infarction in patients with and without diabetes mellitusHypertension200546123824315851627
- CallisterTQRaggiPCooilBLippolisNJRussoDJEffect of HMG-CoA reductase inhibitors on coronary artery disease as assessed by electron-beam computed tomographyN Engl J Med199833927197219789869668
- BudoffMJShavelleDMLamontDHUsefulness of electron beam computed tomography scanning for distinguishing ischemic from nonischemic cardiomyopathyJ Am Coll Cardiol1998325117311789809922
- AgatstonASJanowitzWRHildnerFJZusmerNRViamonteMJrDetranoRQuantification of coronary artery calcium using ultrafast computed tomographyJ Am Coll Cardiol19901548278322407762
- McClellandRLChungHDetranoRPostWKronmalRADistribution of coronary artery calcium by race, gender, and age: Results from the Multi-Ethnic Study of Atherosclerosis (MESA)Circulation20061131303716365194
- HunoldPVogtFMSchmermundARadiation exposure during cardiac CT: Effective doses at multi-detector row CT and electron-beam CTRadiology2003226114515212511683
- GerberTCCarrJJAraiAEIonizing Radiation in Cardiac Imaging: A Science Advisory From the American Heart AssociationCommittee on Cardiac Imaging of the Council on Clinical Cardiology and Committee on Cardiovascular Imaging and Intervention of the Council on Cardiovascular Radiology and InterventionCirculation200911971056106519188512
- Berrington de GonzalezAMaheshMKimKPProjected cancer risks from computed tomographic scans performed in the United States in 2007Arch Intern Med2009169222071207720008689