Abstract
Thrombosis, the localized clotting of blood, occurs in both the arterial and venous circulation, and has a major impact on health outcomes. The primary etiology of myocardial infarctions, and approximately 80% of strokes, is acute arterial thrombosis. In combination this represents the most common cause of death in the Western world, while the third leading cause of cardiovascular-associated death is venous thromboembolism. An understanding of the pathogenic changes in the vessel wall and the blood that result in thrombosis is crucial for developing safer and more effective antithrombotic drugs. Dabigatran etexilate belongs to a new class of direct thrombin inhibitors. Following oral administration, dabigatran reaches peak plasma concentrations within 2 hours, shows linear pharmacokinetics, and a limited (but important) amount of direct drug interactions. Given once daily at 150 mg or 220 mg, it has proven to be competitive with enoxaparin in the prevention of venous thromboembolism after major orthopedic surgery, with a comparable safety profile. For stroke prevention in patients suffering from atrial fibrillation, dabigatran administered at a dose of 110 mg twice daily was associated with rates of stroke and systemic embolism that were similar to those associated with warfarin, as well as lower rates of hemorrhage. Dabigatran given at a dose of 150 mg twice daily, as compared with warfarin, was associated with lower rates of stroke and systemic embolism but similar rates of major hemorrhage. Oral bioavailability of dabigatran, together with a rapid onset and offset of action and predictable anticoagulation response, makes this newly available antithrombotic drug an attractive alternative to traditional anticoagulant therapies for numerous thrombosis-related indications.
Indications for anticoagulant therapy
Thrombosis, the formation of a blood clot within a blood vessel or cavity of the heart, is a leading cause of death and disability. Up to 15% of patients hospitalized for an acute medical illness develop venous thromboembolic disease and some of them suffer from serious and life-threatening complications such as pulmonary embolism.Citation1 Thromboemboli are blood clots moving through the bloodstream, which may lodge in a vessel and block circulation. The following paragraph summarizes the major indications for anticoagulant therapy and address specific complications and common limitations of current therapeutic regimens.
Venous thromboembolic disease
Although many associate venous thrombosis with recent trauma or surgery, 50% to 70% of symptomatic cases, as well as the majority of cases of fatal pulmonary embolism (PE), occur in medical patients.Citation2 Due to the often silent nature of venous thrombosis, the first sign of a problem may be a clinically significant complication, such as PE. Cancer and other medical illness are major contributors to venous thromboembolism (VTE) risk.Citation3 Hospitalized patients, especially the ones in critical care settings, are often immobile or even bedridden. Even in the absence of medical illness, lack of mobility can lead to venous stasis and VTE, as can occur during long-distance air travel.Citation4 presents common conditions and patient-related, predisposing characteristics that are associated with hospitalization and an increased risk for VTE. Age, in particular, is one of the most important risk factors for VTE.Citation1
Table 1 Common conditions and patient-related predisposing characteristics associated with hospitalization and increased risk for VTE
Prospective studies have shown that hospitalized medical patients at high risk who do not receive preventive anticoagulant therapy develop isolated calf thrombosis in 10% to 15% of cases. The same studies revealed an incidence of proximal deep vein thrombosis (DVT) in 2% to 5% and of PE in 0.3% to 1.5%.Citation5,Citation6
Studies have also shown that anticoagulant prophylaxis reduces the risk of symptomatic VTE in hospitalized medical patients.Citation7 Despite the clear need for prophylactic care to prevent VTE in high-risk medical patients, a recent multinational, cross-sectional reportCitation3 revealed that fewer than 40% of hospitalized medical patients at risk received standard VTE prophylaxis. Therefore, timely risk assessment and preventive therapy is crucial.
In addition to the acute risk of PE, a potentially life-threatening event, venous thrombosis also poses risks of intermediate- and long-term complications that include recurrent DVT, post-thrombotic syndrome, and chronic thromboembolic pulmonary hypertension.
Recurrent DVT
The risk of recurrent DVT varies depending on the initial treatment. With no treatment, about half of the patients with symptomatic proximal DVT or PE experience a recurrence within 3 months.Citation8 When proximal DVT is treated with at least 3 months of effective anticoagulation, the recurrence rate decreases considerably to 4%. Further duration of treatment is strongly dependant on the etiology of the thrombosis (idiopathic vs secondary). Indefinite anticoagulation might be required for unexplained cases of recurrent DVT.Citation9
Post-thrombotic syndrome
Between 20% and 50% of those who develop DVT eventually develop a condition known as post-thrombotic syndrome (PTS).Citation10 The exact cause of PTS is not well understood, but it may involve damage to venous valves, ultimately leading to increased intravenous pressure.Citation11 The main symptom is chronic pain. Signs of PTS include swelling, discoloration of the affected leg, and in severe cases, skin ulceration. PTS is not reliably prevented by prompt antithrombotic therapy following the diagnosis of DVT. This is another reason why preventive therapy is the optimal approach for high-risk patients.Citation12
Chronic thromboembolic pulmonary hypertension
Pulmonary hypertension occurs as a late complication in between 3% and 4% of patients who survive pulmonary embolism.Citation13 Symptoms include progressive shortness of breath and exercise intolerance. Later in the course of the disorder, chest pain with exertion and syncope may occur. Without intervention, the 5-year survival rate once the mean pulmonary artery pressure has reached 40 mmHg is about 30%.Citation14
Atrial fibrillation and stroke prevention
Atrial fibrillation (AF) is the most common sustained arrhythmia seen in clinical practice, affecting an estimated 4.5 million people in the European Union and 2.2 million Americans.Citation15 AF is associated with a major risk of stroke, caused by thrombus formation within the left atrium and embolization to the cerebral arteries. The degree of stroke risk and the need for anticoagulant therapy to lower this risk varies among patients with AF.
The prevalence of this arrhythmia increases sharply with older age. AF is uncommon among individuals ≤50 years old.Citation16 In the Framingham Heart Study, the percentage risk of stroke ascribable to AF rose from 1.5% in the age group 50 to 59 years, to 23.5% in the age group 80 to 89 years. The median age of patients with AF is 72 years.Citation17 Worldwide population trends of increasing life expectancy and increasing prevalence of selected risk factors for AF indicate a worsening epidemic.Citation18 Overall, AF accounts for about 15% of all strokes in the United States.Citation16 The rate of ischemic stroke among AF patients included in clinical primary prevention trials and not treated with antithrombotic therapy averaged 4.5% per year, similar to estimates of stroke risk from the Framingham Heart Study. Further analyses from these studies indicate that the lifetime risk of AF for an individual age 40 years is about 25%.Citation19 AF is more prevalent in men than in women at all ages. The prevalence of AF may actually be even higher, given the potential for AF to remain undiagnosed.Citation20
AF raises the risk of ischemic stroke by a factor of four to five, thought to be predominately the result of cardiogenic thomboembolism.Citation21 This is based on clinical assessments, on operative findings of intracardiac thrombus in patients with rheumatic mitral valve disease, and more recently, on transesophageal echocardiography imaging of thrombus in the left atrium of patients with AF, mainly in the left atrial appendage.Citation16
Given the epidemiologic characteristics of AF and the importance of stroke as a leading cause of death and disability, multiple large-scale, randomized trials have been completed and are under way to find efficacious and relatively safe ways to reduce the risk of ischemic stroke and other systemic thromboembolic events related to AF.
Acute coronary syndrome
Acute coronary syndrome (ACS) occurs when an atherosclerotic plaque ruptures, leading to thrombus formation within a coronary artery. Patients who develop symptoms consistent with ACS, such as chest pain and diaphoresis, require timely evaluation to determine the cause. When ACS is diagnosed, further stratification into categories of ST-elevation myocardial infarction (STEMI), non-ST-elevation myocardial infarction (NSTEMI), and unstable angina guides therapeutic decision-making.Citation22 Following recovery from an episode of ACS, patients continue to be at heightened risk of heart attack and stroke, for which a range of secondary preventive treatments are available.Citation23
Mechanical heart valve recipients
Optimal anticoagulation management in patients after mechanical heart valve replacement is still an unresolved issue. Vitamin K antagonists (VKAs) represent the standard of care for long-term prophylaxis after mechanical heart valve replacement. Nevertheless, thromboembolic events occur in approximately 2% to 5% of these patients per year despite oral anticoagulation (OAC).Citation24 The incidence of bleeding complications correlates with VKA dosage, and such complications have been observed within the range of 2% to 9% annually.Citation25 Thromboembolism and anticoagulant-related bleeding account for ≈75% of all complications experienced by heart valve recipients.Citation26 They occur in particular in patients with mechanical heart valves in need of invasive or surgical procedures when the antithrombotic therapy is switched from VKAs to heparins or vice versa.Citation26,Citation27 Therefore, it is important to find alternative approaches for the prophylaxis of thromboembolic complications after mechanical heart valve replacement that are associated with fewer bleeding events.
Benefits and limitations of current anticoagulation regimen
While most current anticoagulant drugs () have been mainstays of antithrombotic therapy for decades, many clinicians find these medications challenging to use. This, when combined with underappreciation of the degree of VTE risk in certain patients, has led to considerable underuse of preventive antithrombotic therapy in some countries. Observational studies reveal that fewer than half of the patients at high risk of VTE receive prophylactic treatment.Citation2,Citation5
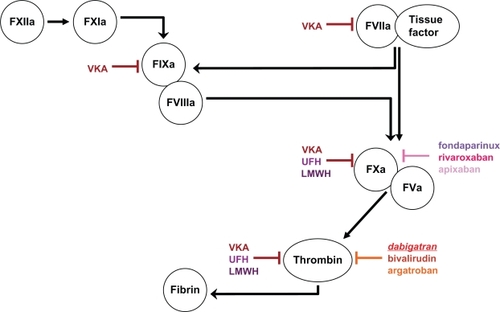
Figure 1 Targets of different anticoagulant agents (indicated in colored blocking arrows) in the coagulation cascade.
A new anticoagulant that more closely meets the criteria for optimal antithrombotic efficacy could improve the quality of care. Such an advance also might help overcome the gaps between evidence-based treatment recommendations and clinical practice. Ideally, an anticoagulant should be administered orally. It should be highly effective in reducing venous thromboembolism, inhibiting both free and clot-bound coagulation factors, have a predictable dose response and kinetics, and show low, nonspecific plasma protein binding, resulting in a low rate of bleeding events. Coagulation monitoring and dose adjustment should not be routinely required, thus creating a wide therapeutic window. Furthermore, there should be only little interaction with food or other drugs.
Vitamin K antagonists
Antagonists of vitamin K have been used as anticoagulants for over 50 years. Warfarin, a synthetic derivative of coumarin, is the most commonly used VKA in the US. In some European countries, other coumarin derivatives (phenprocoumon and acenocoumarol) are used instead.Citation28
With appropriate dosing, these medications effectively inhibit coagulation and have been shown to substantially reduce the risk of stroke in AF and the likelihood of recurrence in VTE.Citation29 However, VKAs are limited by a narrow therapeutic window, with a resultant need for frequent monitoring and dosage adjustments. Other drawbacks of this class include drug and food interactions (eg, vitamin-K-rich foods), a well-documented incidence of major bleeding of 1% to 3%, and delayed onset and offset of anticoagulant effect.Citation28 Bleeding is the most common adverse event with VKAs. The incidence of major bleeding varies from less than 2% a year with care in an anticoagulation clinic to 4% to 5% a year with usual medical care.Citation19,Citation27
Heparins
Unfractionated heparin (UFH) has been used for the prevention and treatment of thrombosis since the 1930s. Low-molecular-weight heparins (LMWHs), derived from UFH by depolymerization, were introduced in Europe in the 1980s.Citation29 Because of several clinical advantages, LMWHs have gradually replaced UFH for most indications. However, UFH continues to be used during cardiovascular surgery and catheter-based interventional procedures.Citation30
Heparins and heparinoids are parenteral agents, administered either intravenously or subcutaneously. The need for parenteral administration makes these agents both inconvenient and costly for long-term use, especially outside the hospital setting.Citation15
Each LMWH product has a specific molecular weight distribution. This distribution determines its anticoagulant activity, duration of action, and renal clearance, so each agent is considered a unique drug. Indications for LMWHs vary – one product cannot always be substituted for another. LMWHs in current use globally include enoxaparin, dalteparin, nadroparin, tinzaparin, certoparin, reviparin, parnaparin and bemiparin.Citation31
Bleeding is the most common adverse event with heparin therapy. Major bleeding occurs in 0.8% of patients receiving full-dose UFH, but is less frequent with low-dose subcutaneous heparin. LMWH has been reported to cause bleeding less frequently, but this finding has not been consistent across trials. Major bleeding occurs in less than 3% of patients and varies with product, indication, patient population, and dose.Citation32
Although, hemorrhage is the most common and best recognized complication of heparin treatment, potentially more dangerous is the development of heparin-induced thrombocytopenia (HIT), especially HIT complicated by thrombosis syndrome (HITTS). All patients exposed to heparin, irrespective of the dose and route of administration, are at risk of developing HIT. This condition develops as the result of the formation of antibodies to the heparin-platelet factor 4 complex, which causes secondary activation of platelets, coagulation, and ultimately increased thrombin production.Citation33
Danaparoid, available in several countries, is classified as a heparinoid. It is composed of sulfated glycosaminoglycans and can be used as an alternative to heparin in patients suffering from HIT.Citation31
Factor Xa inhibitors
Fondaparinux, a pentasaccharide, is a synthetic indirect inhibitor of Factor Xa (FXa). Unlike heparin, fondaparinux does not inactivate thrombin or inhibit FXa bound in the prothrombinase complex and therefore does not completely inhibit FXa. Long-term use is limited by the requirement of subcutaneous injection.Citation34
Bleeding is the most common adverse event with fondaparinux, with major bleeding occurring at about the same rate as seen with patients treated with LMWHs. Episodes of excessive bleeding due to fondaparinux may be treated effectively with Novoseven (recombinant coagulation factor VIIa).Citation34
Orally available FXa-inhibitors, such as rivaroxaban and apixaban, are currently being investigated in large Phase II and III trials. Rivaroxaban (Xarelto®; Bayer Schering Pharma) is already approved for the primary prevention of VTE after orthopedic surgery in adults in Canada as well as the European Union.
Direct thrombin inhibitors
Parenteral direct thrombin inhibitors are used during percutaneous coronary interventions (PCIs), and to treat or prevent thrombosis in patients with HIT. Three such medications are in current clinical use – lepirudin, bivalirudin, and argatroban. These drugs differ with respect to thrombin binding sites, reversibility, pharmacology, and specific indications.Citation35
The first oral direct thrombin inhibitor available for clinical use was ximelagatran. This medication represented a major advance over existing oral anticoagulants (eg, VKAs) because it did not require anticoagulant monitoring or dose adjustments. In clinical VTE prevention and treatment, ximelagatran was either more effective than or comparable to warfarin. However, safety monitoring revealed liver toxicity in 6% of patients. For this reason, use of the drug was discontinued in 2006.Citation36
Advantages and disadvantages of the oral direct thrombin inhibitor dabigatran etexilate will be described in the following sections.
Dabigatran etexilate- pharmacology, pharmacokinetics, and safety
Dabigatran etexilate (Pradaxa® in Europe, Pradax® in Canada; Boehringer Ingelheim) is a small molecule prodrug which does not exhibit any pharmacological activity. After oral administration, dabigatran etexilate is rapidly absorbed and converted to dabigatran by esterase-catalyzed hydrolysis in plasma and in the liver. The prodrug contains micropellets with dabigatran etexilate around a tartaric acid core, since a low pH is necessary for optimal drug absorption.Citation37
Dabigatran is a potent, competitive, reversible direct thrombin inhibitor. Since thrombin (serine protease) enables the conversion of fibrinogen into fibrin during the coagulation cascade, its inhibition prevents the development of thrombus. Dabigatran also inhibits free thrombin, fibrin-bound thrombin and thrombin-induced platelet aggregation.Citation38
Dabigatran prolongs the activated partial thromboplastin time (aPTT). In patients who are bleeding, aPTT tests may be useful in identifying excessive anticoagulant activity, despite the aPTT being less sensitive to the activity of dabigatran at supratherapeutic levels. If available, thrombin time and ecarin clotting time may be more sensitive tests to evaluate the anticoagulant effects of dabigatran. Prothrombin time (INR, international normalized ratio) is prolonged by dabigatran but is less sensitive than thrombin time and ecarin clotting time.Citation39
After oral administration of dabigatran etexilate in healthy volunteers, the pharmacokinetic profile of dabigatran in plasma is characterized by a rapid increase in plasma concentration with maximum concentration (Cmax) attained between 0.5 and 2.0 hours post-administration. After Cmax, plasma concentrations of dabigatran show a biexponential decline with a mean terminal half-life of 14 to 17 hours in young healthy volunteers, and 12–14 hours in elderly subjects. The half-life is independent of dose. Food does not affect the bioavailability of dabigatran but delays the time to peak plasma concentrations by 2 hours. The absolute bioavailability of dabigatran following oral administration of dabigatran etexilate is approximately 6.5%.Citation40
Dabigatran is eliminated largely unchanged in the urine, at a rate of approximately 100 mL/min corresponding to the glomerular filtration rate. Low (34% to 35%) concentration independent binding of dabigatran to human plasma proteins was observed. The exposure (area under the curve = AUC) of dabigatran after the oral administration of dabigatran etexilate is approximately 2.7-fold higher in volunteers with moderate renal insufficiency (creatinine clearance = CrCL between 30 to 50 mL/min) than in those without renal insufficiency. In a small number of volunteers with severe renal insufficiency (CrCL 10 to 30 mL/min), the exposure (AUC) to dabigatran was approximately 6 times higher and the half-life approximately 2 times longer than that observed in a population without renal insufficiency.Citation41 Specific pharmacokinetic studies with elderly subjects showed increases of 40% to 60% in the exposure (AUC) and of more than 25% in Cmax compared to young subjects. Population-based pharmacokinetic studies have evaluated the pharmacokinetics of dabigatran after repeated doses in patients (up to 88 years). The observed increase in dabigatran exposure (AUC) correlated with age-related reductions in CrCL.Citation41
No change in dabigatran exposure (AUC) was seen in 12 subjects with moderate hepatic insufficiency (Child-Pugh B) compared to 12 controls. Body weight had a minor effect on plasma clearance of dabigatran resulting in higher exposure (AUC) in patients with low body weight.Citation42 There were no differences in the phase 3 clinical studies for efficacy and safety data between men and women. Drug exposure (AUC) in female patients is about 40% to 50% higher than in male patients, but no dose adjustment is recommended. Ethnic origin does not appear to affect the pharmacokinetics of dabigatran in a clinically relevant manner. However, no pharmacokinetic data in black patients are available.Citation43
In vitro interaction studies did not show any inhibition or induction of the principal isoenzymes of cytochrome P450.Citation44 This has been confirmed by in vivo studies with healthy volunteers, who did not show any interaction between this treatment and atorvastatin (CYP3A4), digoxin (P-gp transporter interaction) or diclofenac (CYP2C9). However, dabigatran is not without important drug interactions. P-glycoprotein inhibitors (including verapamil, amiodarone, and especially quinidine) raise dabigatran serum concentrations considerably. For example, dabigatran exposure in healthy subjects was increased by 60% in the presence of amiodarone.Citation42
The population pharmacokinetic analysis of co-medication effects supports the use of antacids and gastric acids suppressants without dose adjustment of dabigatran etexilate in patients, and revealed the absence of dabigatran drug interactions with the most commonly used drugs in the study population.Citation43
Dabigatran etexilate in the prevention of deep vein thrombosis
For more than 20 years, routine preventive anticoagulant therapy has been the standard of care for major orthopedic surgery. Despite the well-recognized risks of VTE in hospitalized patients, there remains a low rate of appropriate prophylaxis.Citation5
Major orthopedic surgery involving the lower extremity – hip or knee replacement surgery or hip fracture surgery – is associated with a high risk of VTE. Without prophylaxis, rates of DVT range from 40% to 60% when assessed by venography 7 to 14 days after surgery. Routine ventilation-perfusion scans in patients following hip or knee arthroplasty revealed pulmonary emboli in 3% to 28% of patients.Citation3 Most cases of symptomatic VTE manifest after discharge from the hospital, and are the most common reason for readmission following orthopedic procedures.Citation1,Citation5
Patients who have had total hip replacement and no VTE by venography at discharge continue to be at risk of late-onset VTE up to 35 days after surgery.Citation2 Current recommendations regarding the duration of anticoagulation treatment following hip and knee surgery are based on this understanding of the chronology of VTE.Citation7
In 2 large randomized, parallel group, double-blind, dose-confirmatory trials,Citation45,Citation46 patients undergoing elective major orthopedic surgery (one for knee replacement surgery and one for hip replacement surgery) received dabigatran etexilate 75 mg or 110 mg within 1 to 4 hours of surgery followed by 150 or 220 mg daily thereafter, hemostasis having been secured, or enoxaparin 40 mg on the day prior to surgery and daily thereafter. In the RE-MODEL trial (knee replacement) treatment was for 6 to 10 days and in the RE-NOVATE trial (hip replacement) for 28 to 35 days. Totals of 2076 patients (knee) and 3494 (hip) were treated respectively. The results of RE-MODEL with respect to the primary end-point, total VTE including asymptomatic DVT plus all-cause mortality, showed that the antithrombotic effect of both doses of dabigatran etexilate were statistically non-inferior to that of enoxaparin. Similarly, total VTE including asymptomatic DVT and all-cause mortality constituted the primary endpoint for RE-NOVATE. Again dabigatran etexilate at both daily doses was statistically non-inferior to enoxaparin 40 mg daily.
However, non-inferiority was not established in a third randomized, parallel group, double-blind trial (RE-MOBILIZE), in which patients undergoing elective total knee surgery received dabigatran etexilate 75 mg or 110 mg within 6 to 12 hours of surgery followed by 150 mg and 220 mg daily thereafter. The treatment duration was 12 to 15 days. In total 2615 patients were randomized and 2596 were treated. The comparator dosage of enoxaparin was 30 mg twice daily according to common recommendations in the US. There were no statistical differences in bleeding between the comparators.Citation47 Mostly due to these findings dabigatran etexilate did not get approved for treatment in North America at this point by the US Food and Drug Administration.
A randomized, parallel group, double-blind, placebo-controlled phase II study in Japanese patientsCitation48 in which dabigatran etexilate was administered at 110 mg, 150 mg, and 220 mg the day after elective total knee replacement surgery, showed a clear dose response relationship for the efficacy of dabigatran etexilate and a placebo like bleeding profile. In RE-MODEL and RENOVATE the randomization to the respective study medication was done pre-surgery, and in the RE-MOBILIZE and the Japanese trial the randomization was performed post-surgery. This is of note especially in the safety evaluation of these trials.
In the recently published RE-COVER trial, dabigatran etexilate (150 mg twice daily) was as effective and safe as warfarin (adjusted INR of 2.0 to 3.0) in patients suffering from acute VTE.Citation49 Further studies are currently recruiting patients to investigate the efficacy and safety of dabigatran in the prevention of secondary VTE (RE-MEDY and RE-SONATE).
Dabigatran etexilate in stroke prevention and management of atrial fibrillation
Cardioembolic stroke is one of the main complications of AF, and occurs when stagnant blood in the fibrillating atrium forms a thrombus that then embolizes to the cerebral circulation, blocking arterial blood flow and causing ischemic injury. The incidence of stroke in patients with nonvalvular AF is between 2- and 7-fold greater than in the general population. For patients with AF caused by valvular disease, the risk of stroke increases 17-fold.Citation50
A systematic review of 6 cohorts of AF patients identified three other independent risk factors in addition to age: prior history of stroke or transient ischemic attack, history of hypertension, and diabetes.Citation51 Several scoring systems are available to help clinicians estimate the stroke risk in AF. One popular, well-validated risk assessment tool is the CHADS2-Score ().Citation52
Table 2 CHADS2 score
The recently presented RE-LY trial,Citation53 which compared two fixed doses of dabigatran etexilate (110 mg and 150 mg) administered twice daily to warfarin, has major implications for prevention of stroke, thromboembolic complications, and life-threatening hemorrhagic complications. The trial randomly assigned 18113 patients who had AF and a concomitant risk of stroke. Rates of the primary outcome (stroke or systemic embolism) were 1.69% per year in the warfarin group compared with 1.53% per year in the group that received 110 mg of dabigatran (relative risk with dabigatran, 0.91; 95% confidence interval [CI] 0.74 to 1.11; P < 0.001 for non-inferiority), and 1.11% per year in the group that received 150 mg of dabigatran (relative risk, 0.66; 95% CI 0.53 to 0.82; P < 0.001 for superiority).
The rate of major bleeding was 3.36% per year in the warfarin group, as compared with 2.71% per year in the group receiving 110 mg of dabigatran (P = 0.003) and 3.11% per year in the group receiving 150 mg of dabigatran (P = 0.31). Further, the rate of hemorrhagic stroke was 0.38% per year in the warfarin group, compared with 0.12% per year with 110 mg of dabigatran (P < 0.001) and 0.10% per year with 150 mg of dabigatran (P < 0.001).
No real advantage was seen in mortality rate, which was 4.13% per year in the warfarin group, 3.75% per year with 110 mg of dabigatran (P = 0.13) and 3.64% per year with 150 mg of dabigatran (P = 0.051).
In sum, dabigatran administered at a dose of 110 mg twice daily was associated with rates of stroke and systemic embolism that were similar to those seen with warfarin, but with lower rates of hemorrhage, while dabigatran at 150 mg twice daily was associated with lower rates of stroke and systemic embolism but similar rates of major hemorrhage.
Likely due to the controlled trial setting, the rate of bleeding in the warfarin group was slightly lower (3.36% per year) than is usually seen in real-world ambulatory care of anticoagulated patients. It is possible that, if used in patients outside of a clinical trial, bleeding complications will occur even more infrequently with dabigatran than with warfarin.
Surprisingly, the annualized rates for myocardial infarction (MI) were 0.72% for low-dose dabigatran, 0.74% for high-dose dabigatran, and 0.53% for warfarin. The risk trended higher for low-dose dabigatran at 1.35 (95% CI 0.98 to 1.87; P = 0.07) and was significantly higher for in the high-dose group at 1.38 (95% CI 1.00 to 1.91; P = 0.048). This somewhat unexpected finding leads to the hypothesis that warfarin is more effective in reducing MI than dabigatran at this particular aspect of antithrombotic therapy. However, the absolute rates of MI were quite low, and the effect of dabigatran in reducing stroke and intracerebral bleedings far outweighed the small increase in MI rate.
Rates of dyspepsia (including abdominal pain) were increased with dabigatran (11.8% in the 110-mg group and 11.3% in the 150-mg group) as compared with warfarin (5.8%), and it may have contributed to the greater second-year rate of dropout in patients taking dabigatran (approximately 21%) as compared with warfarin (16.6%).Citation54
Prospective indications for dabigatran etexilate
Mechanical heart valve thrombosis
Lifelong OAC therapy is required for the prevention of thromboembolic events after implantation of an artificial heart valve. Thromboembolism and anticoagulant-related bleedings account for ≈75% of all complications experienced by heart valve recipients (2% to 9% of patients per year). In preparation for surgical procedures, OAC treatment must be interrupted. The gold standard for adjusting oral to parenteral anticoagulation treatment in patients at a high risk for developing thromboembolic complications is intravenous administration of UFH,Citation25,Citation26 which needs to be continuously infused to ensure an adequate effect. However, anticoagulation with UFH is associated with an increased rate of complications. These complications are related to low bioavailability, short half-life, platelet activation, and inter-individual differences regarding optimal dosage of UFH.Citation27 Although most guidelines favor intravenous administration of UFH, LMWH (eg, enoxaparin, dalteparin, and tinzaparin) represent an additional option for bridging therapy.Citation25,Citation26
A new anticoagulant that more closely meets the criteria for optimal antithrombotic efficacy could improve the quality of care. Such an advance also might help overcome gaps between evidence-based treatment recommendations and clinical practice.
Studies in patients with a strong indication for anticoagulant therapy because of high thromboembolic risk without adequate protection, such as patients with a mechanical heart valve, are not scheduled in the early phase of development of new antithrombotics. Inappropriate dosing would lead to unacceptable outcomes in this high-risk population. A new agent such as dabigatran etexilate could be a welcome addition for improving care in these patients. Future prospective and randomized studies in humans should address the question of whether orally administered dabigatran etexilate is as effective as UFH, LMWH, and VKAs in preventing thrombus formation on mechanical heart valves. Notably, large, randomized, prospective trials are also lacking for LMWH as regards prevention of mechanical heart valve thrombosis.
Less thrombogenic materials and improved valve and hinge designs may reduce the propensity for thrombus formation and the need for aggressive anticoagulation. This might reverse the present trend to increased use of bioprosthetic valves.Citation55 The step from preclinical in vitro and in vivo testing to widespread clinical use is hampered by the lack of good predictive animal models and always entails a certain risk.
Acute coronary syndrome and percutaneous coronary intervention
Risk assessment is a key step in the emergency management of patients with ACS. Stratifying patients by likelihood of morbidity and mortality guides management decisions. A range of risk-scoring systems have been devised to enable clinicians to select the appropriate antithrombotic, antiplatelet and/or fibrinolytic therapy.Citation27
Patients with complete occlusion of a coronary artery can often be identified by ST-segment elevation on electrocardiogram. This group, representing approximately one in three patients presenting with ACS, should receive prompt reperfusion treatment with fibrinolytic therapy or PCI. The remaining two-thirds of ACS patients do not have ST-segment elevation on initial ECG, and require further risk stratification.Citation22
Because atherosclerotic plaque is often present throughout the arterial tree, patients who survive an episode of ACS live with an ongoing risk of a recurrent acute cardiovascular event, such as MI, sudden cardiac death, or stroke.Citation56 For patients who receive a stent during revascularization, there is an additional risk of in-stent thrombosis.Citation22
A wide range of treatments are available to protect the heart and to decrease the propensity for recurrent atherothrombosis in survivors of ACS. Antiplatelet agents such as ASA and clopidogrel are used for up to 12 months after ACS to prevent a recurrent event.Citation22 For immediate antithrombotic therapy a wide range of agents are available. So far all of them need to be administered intravenously. DTIs currently available for intravenous administration that are successfully and primarily used in the treatment of HIT as well as PCI are lepirudin, bivalirudin, and argatroban.Citation57 DTIs are potentially ideal agents for PCI and ACS patients due to their antithrombotic and antiplatelet properties.
Dabigatran is currently being studied in a randomized, open-label phase-II trial in patients undergoing elective PCI (ClinicalTrials.gov Identifier: NCT00818753). The purpose of the study is to assess whether two doses of dabigatran etexilate (110 mg twice daily and 150 mg twice daily) compared with UFH, both in addition to a standard dual antiplatelet regimen, provide sufficient anticoagulation in the setting of elective PCI.
Currently usage of VKAs in patients after ACS has very limited indications as an add-on therapy to antiplatelet drugs such as clopidogrel and aspirin. These indications include patients with AF and at high risk for stroke, mechanical heart valve recipients, and patients with a left ventricular aneurysm and/or thrombus formation in the left ventricular cavity. Triple therapy with antiplatelet drugs and VKAs is associated with a high risk of bleeding. The frequency of such events in reported series varies, with up to 21% of patients needing a transfusion. Bleeding events typically involve the gastrointestinal tract.Citation58 Evidence suggests that this frequency increases with longer duration of triple therapy, which directly correlates with bleeding risk and might influence mortality in follow-up after PCI. In particular, the relative risk of major bleeding in patients receiving triple therapy is 3- to 5-fold higher than that observed in patients receiving dual antiplatelet therapy alone. The increase in bleeding events is confounded by the fact that patients receiving triple therapy are typically older and have multiple co-morbidities. Limited use of triple therapy (for 1 month) is associated with at least a 2-fold lower risk of major bleeding compared with prolonged use (≥6 months).Citation58 Dabigatran etexilate may have a role as an acceptable substitute for VKAs in these high risk patients, but this has not yet been studied.
Conclusions
Recent advances in antithrombotic therapy have the potential to significantly affect the management of patients with thromboembolic disease and disease risk. The development of new orally available agents has already changed the field of anticoagulation beyond the once gold standard of VKAs, and will undoubtedly result in a paradigm shift in the management of these diseases. Warfarin has proven to be very effective for the primary prevention of stroke and AF, as well as for the long-term management of patients with a whole spectrum of thromboembolic-related illnesses. However, its significant limitations have been discussed throughout the review.
These limitations have led to a search for new anticoagulant drugs, a quest made easier by improved understanding of coagulation and targeted inhibition of specific coagulation factors. Not surprisingly, since FXa is the key coagulation factor lying at the crossroads of intrinsic and extrinsic coagulation, a significant interest exists in developing drugs which specifically target activated FXa. Moreover, the inhibition of thrombin may be the most efficient way of inhibiting coagulation, giving rise to the development of drugs which specifically target it.Citation59 Although it is currently not clear which mechanism will give rise to better clinical outcomes, both FXa and thrombin are likely to be excellent targets for inhibition with new anticoagulant drugs.
FXa inhibition appears to be the more promising avenue, as Factor X has fewer functions outside coagulation compared with thrombin. Also, Factor X is associated with a shallower dose response curve, suggesting that Xa inhibitors may have a wider therapeutic window compared to thrombin inhibitors. In contrast, thrombin inhibitors may allow other actions of thrombin to occur, such as activation of the anti-coagulant protein C.Citation60
New oral anticoagulants that are currently in advanced stages of clinical trials offer the potential to revolutionize long-term anticoagulant therapy. Besides dabigatran etexilate these agents are rivaroxaban, apixaban, and edoxaban, all of which inhibit FXa.
Dabigatran etexilate has proven to be a competitive antithrombotic. Potential drawbacks of the drug include the higher occurrence of MIs in the RELY study (in comparison to warfarin), the inferiority compared to the North American enoxaparin regime in the RE-MOBILIZE study, as well as the lack of a readily available antidote or an established anticoagulant monitoring for the detection of a potential non-compliance in standard clinical practice. So far recommendations for dabigatran use in special populations, like renal impairment or failure and application during pregnancy, are also missing. One has to be cautious to only use dabigatran etexilate in the currently approved indication in the European Union and Canada, the primary prevention of VTEs in adults after elective total hip or knee replacement surgery. Further approvals for other countries as well as other indications are pending.
A drug that will prevent coagulation without promoting bleeding has yet to be found. However, molecules that contribute to thrombosis continue to be identified, and these could be new targets for the next generation of antithrombotic therapy. More immediately, recent studies of new antiplatelet drugs (such as prasugrel) and new anticoagulant drugs (such as dabigatran etexilate) suggest that more options will soon be available for the treatment of thrombosis. Furthermore, the ability to identify patients at increased risk of thrombosis by measuring the concentrations of circulating factors, such as tissue factor, might allow more effective use of prophylaxis. Finally, “personalized medicine” is on the horizon, which could allow customized dosing of antithrombotic drugs rather than the current “one dose fits all” strategy.
Disclosures
The authors have no conflicts of interest to declare.
References
- GeertsWHBergqvistDPineoGFPrevention of Venous Thromboembolism: American College of Chest Physicians (ACCP) Evidence-Based Clinical Practice Guidelines (8th Edition)Chest2008381S453S18574271
- MollSMackmanNVenous thromboembolism: a need for more public awareness and research into mechanismsArterioscler Thromb Vasc Biol20082836736918296590
- CohenATTapsonVFBergmannJFENDORSE InvestigatorsVenous thromboembolism risk and prophylaxis in the acute hospital care setting (ENDORSE study): a multinational cross-sectional studyLancet200837138739418242412
- LapostolleFSurgetVBorronSWSevere pulmonary embolism associated with air travelN Engl J Med200134577978311556296
- FrancisCWClinical practice. Prophylaxis for thromboembolism in hospitalized medical patientsN Engl J Med20073561438144417409325
- HeitJASilversteinMDMohrDNPettersonTMO’FallonWMMeltonLJ3rdRisk factors for deep vein thrombosis and pulmonary embolism: a population-based case-control studyArch Intern Med200016080981510737280
- WhiteRHThe epidemiology of venous thromboembolismCirculation2003107I4I812814979
- KearonCNatural history of venous thromboembolismCirculation2003107I22I3012814982
- RodgerMAKahnSRWellsPSIdentifying unprovoked thromboembolism patients at low risk for recurrence who can discontinue anticoagulant therapyCMAJ200817941742618725614
- KahnSRThe post-thrombotic syndrome: the forgotten morbidity of deep venous thrombosisJ Thromb Thrombolysis200621414816475040
- HaenenJHJanssenMCvan LangenHThe postthrombotic syndrome in relation to venous hemodynamics, as measured by means of duplex scanning and strain-gauge plethysmographyJ Vasc Surg1999291071107610359941
- PrandoniPLensingAWCogoAThe long-term clinical course of acute deep venous thrombosisAnn Intern Med1996125178644983
- PengoVLensingAWPrinsMHIncidence of chronic thromboembolic pulmonary hypertension after pulmonary embolismN Engl J Med20043502257226415163775
- FedulloPFAugerWRKerrKMRubinLJChronic thromboembolic pulmonary hypertensionN Engl J Med20013451465147211794196
- SingerDEAlbersGWDalenJEAmerican College of Chest PhysiciansAntithrombotic therapy in atrial fibrillation: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition)Chest200813354659218252921
- LipGNieuwlaatRPistersRLaneDCrijnsHRefining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor based approach: The Euro Heart Survey on Atrial FibrillationChest201013726327219762550
- SchnabelRBSullivanLMLevyDDevelopment of a risk score for atrial fibrillation (Framingham Heart Study): a community-based cohort studyLancet200937373974519249635
- HylekEMAntithrombotic prophylaxis in elderly patients with atrial fibrillationSemin Thromb Hemost20093554855319787558
- LeviMHobbsFDJacobsonAKImproving antithrombotic management in patients with atrial fibrillation: current status and perspectivesSemin Thromb Hemost20093552754219787556
- PistersRde VosCBNieuwlaatRCrijnsHJUse and underuse of oral anticoagulation for stroke prevention in atrial fibrillation: old and new paradigmsSemin Thromb Hemost20093555455919787559
- LeviMde PeuterORKamphuisenPWManagement strategies for optimal control of anticoagulation in patients with atrial fibrillationSemin Thromb Hemost20093556056719787560
- AndersonJLAdamsCDAntmanEMAmerican College of CardiologyAmerican Heart Association Task Force on Practice GuidelinesACC/AHA 2007 guidelines for the management of patients with unstable angina/non-ST-Elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice GuidelinesJ Am Coll Cardiol200750115717601538
- VickreyBGRectorTSWickstromSLOccurrence of secondary ischemic events among persons with atherosclerotic vascular diseaseStroke20023390190611935034
- CannegieterSCTornMRosendaalFROral anticoagulant treatment in patients with mechanical heart valves: how to reduce the risk of thromboembolic and bleeding complicationsJ Intern Med199924536937410356599
- American College of Cardiology/American Heart Association Task Force on Practice GuidelinesSociety of Cardiovascular AnesthesiologistsSociety for Cardiovascular Angiography and InterventionsSociety of Thoracic SurgeonsBonowROCarabelloBAKanuCACC/AHA guidelines for the management of patients with valvular heart disease. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (writing committee to revise the 1998 Guidelines for the Management of Patients With Valvular Heart DiseaseCirculation200611484231
- VahanianABaumgartnerHBaxJTask Force on the Management of Valvular Hearth Disease of the European Society of CardiologyESC Committee for Practice GuidelinesGuidelines on the management of valvular heart diseaseEur Heart J20072823026817259184
- HirshJGuyattGAlbersGWHarringtonRSchünemannHJAmerican College of Chest PhysicianAntithrombotic and thrombolytic therapy: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition)Chest2008133110112
- EikelboomJWWeitzJIA replacement for warfarin: the search continuesCirculation200711613113317576860
- HirshJO’DonnellMEikelboomJWBeyond unfractionated heparin and warfarin: current and future advancesCirculation200711655256017664384
- FrydmanALow-molecular-weight heparins: an overview of their pharmacodynamics, pharmacokinetics and metabolism in humansHaemostasis19962624388707165
- BickRLFrenkelEPWalengaJFareedJHoppensteadtDAUnfractionated heparin, low molecular weight heparins, and pentasaccharide: basic mechanism of actions, pharmacology, and clinical useHematol Oncol Clin North Am20051915115639107
- VeselyMRKelemenMDCardiac risk assessment: matching intensity of therapy to riskCardiol Clin200624677816326257
- WarkentinTEGreinacherAKosterALincoffAMTreatment and Prevention of Heparin-Induced Thrombocytopenia: American College of Chest Physicians (ACCP) Evidence-Based Clinical Practice Guidelines (8th Edition)Chest2008340S380S18574270
- ChaturvediVKarthikeyanGFondaparinux in acute coronary syndromesExpert Opin Drug Metab Toxicol200951615162319929450
- HarenbergJWehlingMCurrent and future prospects for anticoagulant therapy: inhibitors of factor Xa and factor IIaSemin Thromb Hemost200834395718393142
- HaasSNew anticoagulants – towards the development of an “ideal” anticoagulantVasa200938132919229800
- WienenWStassenJMPriepkeHRiesUJHauelNAntithrombotic and anticoagulant effects of the direct thrombin inhibitor dabigatran, and its oral prodrug, dabigatran etexilate, in a rabbit model of venous thrombosisJ Thromb Haemost200751237124217362226
- StangierJRathgenKStähleHGansserDRothWThe pharmacokinetics, pharmacodynamics and tolerability of dabigatran etexilate, a new oral direct thrombin inhibitor, in healthy male subjectsBr J Clin Pharmacol20076429230317506785
- ErikssonBISmithHYasothanUKirkpatrickPDabigatran etexilateNat Rev Drug Discov2008755755818591978
- HaasSNew oral Xa and IIa inhibitors: updates on clinical trial resultsJ Thromb Thrombolysis200825526017965837
- WolowaczSERoskellNSPlumbJMEconomic evaluation of dabigatran etexilate for the preventionof venous thromboembolism in patients aged over 75 years or with moderate renal impairment undergoing total knee or hip replacementThromb Haemost201010336037120024501
- StangierJClemensAPharmacology, pharmacokinetics, and pharmacodynamics of dabigatran etexilate, an oral direct thrombin inhibitorClin Appl Thromb Hemost2009819 [Epub ahead of print]
- DahlOEDabigatran etexilate: A new oral thrombin inhibitortherapy20085111
- WienenWStassenJMPriepkeHRiesUJHauelNIn-vitro profile and ex-vivo anticoagulant activity of the direct thrombin inhibitor dabigatran and its orally active prodrug, dabigatran etexilateThromb Haemost20079815516217598008
- ErikssonBIDahlOERosencherNRE-MODEL Study GroupOral dabigatran etexilate vs subcutaneous enoxaparin for the prevention of venous thromboembolism after total knee replacement: the REMODEL randomized trialJ thromb Haemost200752178218517764540
- ErikssonBIDahlOERosencherNRE-NOVATE Study GroupDabigatran etexilate versus enoxaparin for prevention of venous thromboembolism after total hip replacement: a randomised, double-blind, non-inferiority trialLancet200737094995617869635
- GinsbergJSDavidsonBLCompPCRE-MOBILIZE Writing CommitteeOral thrombin inhibitor dabigatran etexilate vs North American enoxaparin regimen for prevention of venous thromboembolism after knee arthroplasty surgeryJ Arthroplasty2009241918534438
- FujiTFuijitaSUjihiraTSatoTDabigatran etexilate prevents venous thromboembolism after total knee arthroplasty in Japanese patients, with a safety profile comparable to placeboJ Arthroplasty20091024 [Epub ahead of print].
- SchulmanSKearonCKakkarAKDabigatran versus warfarin in the treatment of acute venous thromboembolismN Engl J Med20093612342235219966341
- QureshiAIFeldmannEGomezCRIntracranial atherosclerotic disease: an updateAnn Neurol20096673073820035502
- HartRGPearceLAAguilarMIMeta-analysis: antithrombotic therapy to prevent stroke in patients who have nonvalvular atrial fibrillationAnn Intern Med200714685786717577005
- GageBFWatermanADShannonWBoechlerMRichMWRadfordMJValidation of clinical classification schemes for predicting stroke: results from the National Registry of Atrial FibrillationJAMA20012852864287011401607
- ConnollySJEzekowitzMDYusufSRE-LY Steering Committee and Investigators. Dabigatran versus Warfarin in Patients with Atrial FibrillationN Engl J Med20093611139115119717844
- GageBFCan we rely on RE-LY?N Engl J Med20093611200120219717843
- HerijgersPVerhammePImproving the quality of anticoagulant therapy in patients with mechanical heart valves: what are we waiting for?Eur Heart J2007282424242617890728
- Viles-GonzalezJFFusterVBadimonJJAtherothrombosis: a widespread disease with unpredictable and life-threatening consequencesEur Heart J2004251197120715246637
- TurpieAGDirect Factor Xa and direct thrombin inhibitors: a clinical trial updateCurr Opin Drug Discov Devel200912497508
- HolmesDRJrKereiakesDJKleimanNSCombining antiplatelet and anticoagulant therapiesJ Am Coll Cardiol2009549510919573725
- WeitzJIFactor Xa or thrombin: is thrombin a better target?J Thromb Haemost20075656717635711
- MackmanNTriggers, targets and treatments for thrombosisNature200845191491818288180