Abstract
Coronary computed tomographic angiography (CCTA) is a rapidly evolving test for diagnosis of coronary artery disease. Although invasive coronary angiography is the gold standard for coronary artery disease (CAD), CCTA is an excellent noninvasive tool for evaluation of chest pain. There is ample evidence to support the cost-effective use of CCTA in the early triage process of patients presenting with chest pain in the emergency room. CCTA plays a critical role in the diagnosis of chest pain etiology as one of potentially fatal conditions, aortic dissection, pulmonary embolism, and myocardial infarction. This ‘triple rule out’ protocol is becoming an increasingly practicable and popular diagnostic tool in ERs across the country. In addition to a quick triage of chest pain patients, it may improve quality of care, decrease cost, and prevent medico-legal risk for missing potentially lethal conditions presenting as chest pain. CCTA is also helpful in the detection of subclinical and vulnerable coronary plaques. The major limitations for wide spread acceptance of this test include radiation exposure, motion artifacts, and its suboptimal imaging with increased body mass index.
Background
Coronary computer tomographic angiography (CCTA) has been playing an incremental role in the diagnosis of coronary artery disease (CAD). CCTA has been especially useful in the triage of patients with acute chest pain. These patients are frequent visitors of emergency rooms posing an immediate diagnostic and therapeutic challenge. Chest pain patients present with potentially fatal conditions such as acute coronary syndrome (ACS), aortic dissection (AD), and pulmonary embolism (PE). Efficient evaluation of these chest pain patients with CCTA prevents complications, death, and disability. Evaluation and triage of more than 6,392,000 patientsCitation1 presenting with chest pain nationwide poses a significant challenge to the health care system and CCTA evaluation of these patients may alleviate this challenge and save not only lives, but also the cost and complications of invasive procedures such as cardiac catheterization. This becomes an important issue in small community hospitals where limited resources have to be efficiently used.
Evolution of CCTA
Since the pioneering work of Sir Godfrey N Hounsfield in 1972, CT technology has developed at a fast pace. Electron beam computed tomography (EBCT), otherwise called ultrafast CT or cine CT, was first introduced in 1980, followed by the 4-slice CT in the year 2000, 16-slice in 2002, and 64-slice in 2004. Initially cardiac CT, performed on 4-slice multidetector computed tomography (MDCT), examinations were confined to the evaluation of only proximal coronary arteries. There was poor spatial and temporal resolution with long acquisition time requiring intolerably long breath hold periods. This was revolutionized by the 16-slice MDCT, where for the first time a complete examination of coronary arteries was performed with a breath hold of just 20 seconds. Then the 64-slice MDCT scan became widely available. These scanners have much higher spatial and temporal resolution with a scan time of 12–15 seconds compared to 20 seconds with the 16-slice coronary CTA. This enables medical staff to perform a rapid screen for CAD in community hospitals.
The CT has undergone a dramatic improvement in imaging with evolution from a single-slice/detector to a multi-slice/detector leading to the commonly used terminology, MDCT or multi-slice computed tomography (MSCT). In this manuscript, for coronary imaging, the term CCTA will be used interchangeably with MDCT or MSCT.
This modality employs a rotating source of X-rays with circular and stationary detector arrays. X-ray photons are generated within a specialized X-ray tube mounted on a rotating gantry which pass through the patient’s body and are detected by fixed rows of detector arrays, thus producing images of coronary arteries in seconds after the patient is scanned with current scanners as shown in and .
Figure 1 Illustration of thin MIP reconstruction of left coronary artery.
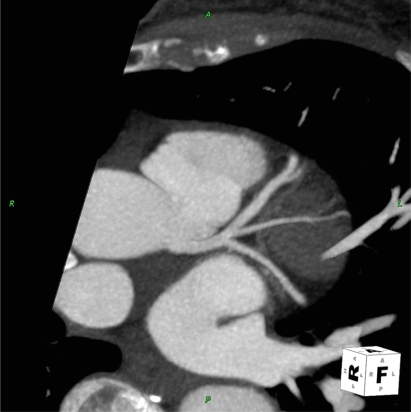
Figure 2 Illustration of soft and calcified plaque in proximal and mid LAD.

Most recently, 256-slice and 320-slice scanners have been introduced. With this new generation of scanners, there has been a progressive improvement in spatial and temporal resolution. Similarly, dual-source CT (DSCT) scanners incorporate two tubes and two corresponding detectors which offer considerable advantage with temporal resolution as low as 83 ms,Citation2 leading to elimination of a majority of artifacts.Citation3 Its role is also evolving in the detection of subclinical atherosclerosis and vulnerable plaque, the most common cause of ACS.
Scope of CCTA in patients with chest pain
Chest pain is a frequent complaint among emergency room (ER) patients in this country. In many of these patients, basic evaluation by the ER physician including history, physical examination, electrocardiography (ECG), and initial cardiac biomarkers does not exhibit evidence of active myocardial ischemia. Inappropriate numbers of these patients are admitted to hospitals with suspected ACS leading to long hospital stays especially over the weekends. Extensive efforts have been made over the past decade to create chest pain centers with protocols in place for early detection, risk stratification, and timely discharge of chest pain patients. While this concept is helpful, there has been a continued practice of expensive evaluation and prolonged hospitalization for a majority of these patients presenting with chest pain.
More than 50% of ER admissions to the hospital are for observation to collect preliminary data to exclude ACS, PE, and AD. Unfortunately, positive yield of this large number of admissions is as low as 2%–5%,Citation4,Citation5 and a majority of these patients (55%) are found to have noncardiac pathology.Citation6 Conversely, 2% of patients with chest pain are discharged inappropriately with missed diagnosis of ACS, PE, and AD.Citation6–Citation8
The underlying reason for this practice is to exclude any potentially fatal etiologies of chest pain such as MI, PE, and AD. Therefore, physicians are reluctant to send these patients home from the ER because of the risk of 2% missed diagnosis of acute myocardial infarction (AMI)Citation6,Citation9,Citation10 in these patients. This type of ER practice is fraught with a tremendous cost of more than 12 billion dollars a year.Citation11 In community hospitals, the wide spread availability of CCTA as an important test may expedite early diagnosis and discharge of chest pain patients. Furthermore, unnecessary transfer of some of these patients to tertiary care hospitals may be avoided and significant health care savings may be achieved.
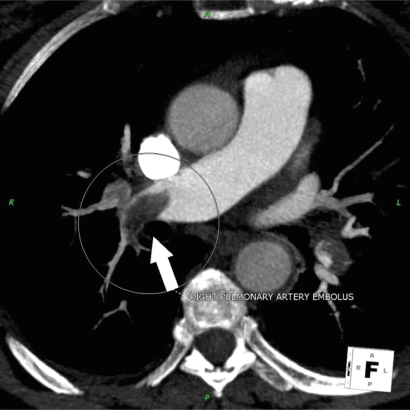
The gold standard for visualization of coronary arteries has been invasive coronary angiography. The use of this technique has increased many fold over the past three decades leading to exorbitant cost and inconvenience to the patients.Citation12 Furthermore, it is plagued with the issue of operator dependent variability in coronary lesion assessment for percent stenosis.Citation13 Consequently, there has been an increasing interest to develop a less invasive and cost effective technique for evaluation of coronary arteries. Out of many exciting technologies, CCTA is emerging as the most promising tool for the diagnosis of CAD, while excluding other potentially fatal conditions such as AD () and PE () which may also present with chest pain. Therefore, there is a great need for a noninvasive tool such as CCTA for definitive early diagnosis of the cause of chest pain in the ER.
Figure 3 Patient presenting with acute chest pain; CCTA image showing large aortic root dissection.

Figure 4 Patient presenting with acute chest pain; CCTA image showing large right pulmonary artery embolism.
Current indications
There is a definite role for CCTA in patients with chest pain who have low to intermediate probability of CAD and other cardiac conditions as listed in . There has been an emerging role for this test in the ‘triple rule out’ protocol for chest pain patients in the ER.
Table 1 Indications for CCTA
Emerging indications
The crucial role of CCTA for evaluation of chest pain and early triage of patients in the ER is evolving very fast. The feature of three dimensional volumetric acquisitions virtually allows unlimited views for image projection after processing. There has been intense interest in ‘triple rule out’ protocol for chest pain by a single acquisition that results in simultaneous opacification of coronary arteries, aorta, and arterial phase opacification of pulmonary arteries. This examination may need 110 cc of contrast, a specialized post-processing with routine reconstruction for coronaries, wide field of view (FOV) coronal reconstruction of lungs, and oblique sagittal reconstruction for thoracic aorta. The major disadvantage of ‘triple rule out’ protocol is an increase in the radiation dose due to the large area of coverage and an increase in contrast use. CCTA has the advantage of faster acquisition in a single breath hold with excellent imaging resolution. More importantly, widespread availability makes its usage feasible in community hospitals.
Triage tools for chest pain
There are several tools available in the ER for early triage of chest pain patients. The basic practice is to obtain history and physical examination (H&P) with cardiac markers, chest X-ray, and ECG. H&P is a crucial part, and therefore a majority of ERs have developed protocols to elicit all the pertinent history and physical findings. This basic practice helps to risk stratify the patients by TIMI score as illustrated in . The majority of these low to intermediate patients,Citation14 with TIMI score less than three, do not have CAD, and due to very low yield in this group they end up getting admitted to the hospitals for observation and sequential cardiac biomarkers assessment prior to definite evaluation with a stress test and/or cardiac catheterization. Cardiac biomarkers are the standard of care and typically take 6–12 hours to become positive in the blood test and therefore many patients with active ischemia and/or injury may be missed by cardiac biomarkers criteria. CCTA in the ER as a triage tool provides a new paradigm shift, and its role is clearly and rapidly emerging.
Table 2 TIMI score
There are many objective tests used in setting of the ER such as echocardiography, nuclear studies, magnetic resonance imaging (MRI), and coronary artery calcium (CAC) scoring. Echocardiography has a very limited role in chest pain evaluation due to its limited sensitivity for AMI in patients with ACS when pain has already resolved.Citation15,Citation16 In late 1990, many chest pain centers developed the use of the radionuclide stress test using single photo emission computed tomography (SPECT) to help risk stratification and early discharge of chest pain patients in the ER. Myocardial imaging studies with Tc-99m-based radioisotope have shown an excellent negative predictive value (NPV) as a screening test,Citation17,Citation18 though the positive predictive value may be limited due to suboptimal imaging resolution and artifacts. MRI has the ability to diagnose CAD and other potentially fatal conditions such as PE and AD.Citation19,Citation20 However, its use as a first line test is limited by multiple factors such as technical expertise, physician availability on site, and contraindications to MRI due to metallic implants.
Absence of CAC or minimal CAC predicted a very low incidence of future cardiac events in asymptomatic patientsCitation21–Citation24 and symptomatic patients undergoing coronary angiography.Citation6,Citation9,Citation10 Several studies have shown the value of CAC in ER patients with negative ECG and cardiac enzymes as a triage tool with a very high negative predictive value (NPV).Citation25,Citation26 Georgiou et al performed EBCT in 192 patients with chest pain and had an average follow up of 50 ± 10 months. Among this cohort, 30% showed a graded relationship between all cardiac events and CAC score.Citation26 This study showed CAC as a triage test with sensitivity of 97% and NPV of 99%. Patients without CAC (CAC score = 0) had 0.6/year future cardiovascular events. Recent studies have shown that CAC may be a useful tool in the ER for risk stratification of patients with ACS. Several other studies have demonstrated a significant correlation between CAC and the overall coronary artery atherosclerotic plaque burden.Citation27–Citation31 These studies have shown high sensitivity >95% and high NPV of >95%.
CCTA as a triage tool
CCTA may become an attractive option as a triage tool in the ER due to its widespread availability and noninvasive approach. Several CCTA studies have shown an excellent correlation of CCTA with coronary angiography with sensitivities ranging from 92%–95% and NPV of 97%–98% for the diagnosis of significant CAD.Citation32–Citation36 Two published meta-analyses have shown excellent sensitivity and specificity of CCTA for CAD as compared to coronary angiography.Citation37,Citation38 Moreover, CCTA has shown a promise in detecting noncalcified plaque,Citation39 and an evaluation global left ventricular function comparable to MRI.Citation40
As early as 1996, many studies have investigated its use as a triage tool in ER patients with chest pain, negative ECG, and cardiac enzymes.Citation41 The NPV of CCTA in such patients has been reported to be 97%–100%. Gallagher et al reported their experience with CCTA in low risk patients with negative ECG and cardiac markers in the ERCitation42 where all patients had nuclear sestamibi scan and CCTA. This study reflected the accuracy of CCTA comparable to well established nuclear tests in these low risk patients.
Initial evaluation of ACS patients in the ER was performed using 16-slice CCTA by Kimura et al.Citation43 A total of 74 consecutive patients with ACS (non-ST elevation) patients with ACS/non-ST elevation myocardial infarction (NSTEMI) underwent CCTA within 24 hours. Significant coronary lesions were correctly identified in 56 out of 57 patients. Similarly, 11 out of 13 patients without significant disease were correctly diagnosed. Lida et al have reported similar findings in 28 patients with ACS.Citation44 Subsequently, there have been many studies using 64-slice CCTA. A single center experience in 70 patients using 64-slice CCTA showed sensitivity of 95%, specificity of 90%, and NPV of 93%.Citation36
A recent study, Rule Out Myocardial Infarction using Computer Assisted Tomography (ROMICAT)Citation45 evaluated the value of CCTA in the triage of ER patients with ACS. This was an observational cohort study of 368 patients presenting to the ER with chest pain, normal troponin, and nonischemic ECG. 64-slice CCTA was performed in these patients before index hospitalization and results were not disclosed to treating physicians. End points were ACS during index hospitalization and major adverse cardiac events (MACE) in six months. Among this cohort, 50% of patients had no CAD on CCTA, 31% had nonobstructive CAD, and only 19% had more than 50% stenosis or inconclusive considered as positive study. Moreover, door to CCTA was only 16 minutes in ROMICAT compared to 40.5 hours of an average hospital stay.Citation46 Given these findings, a large number of patients did not need hospitalization and could have been triaged in the ER by CCTA.
This study and several other studies may support the use of CCTA in the ER. The ROMICAT studyCitation45 also demonstrated sensitivity and NPV of 100% for ACS. Several other studies have showed higher sensitivity, specificity, and NPV in evaluation of ACS in the ER.Citation47–Citation50 A recent presentation at the American Heart scientific session (2009)Citation51 looked at the role of CCTA as a triage tool in the ER in patients presenting with chest pain in Computed Tomography for Systematic Triage of Acute chest pain and Treatment (CT-STAT) trial. In this trial, investigators included 749 patients presenting to the ER with acute chest pain within 12 hours of onset of symptoms with normal ECG and normal cardiac biomarkers. These patients were randomized to the CCTA arm or to the conventional standard of care treatment arm with myocardial perfusion imaging to expedite early diagnosis. In the CCTA arm, 82.3% had no significant disease leading to early discharge. Among the cohort undergoing conventional management, 90% had a normal myocardial perfusion study as part of standard work up. Early diagnosis (door to diagnosis) was much faster in the CCTA arm with mean diagnosis time 2.9 hours in the CCTA arm compared to 6.2 hours in the conventional standard of care arm with myocardial perfusion imaging. Moreover, the radiation exposure in the CCTA arm was 10.8 mSv compared to 15 mSv in the conventional arm. Overall cost in the CCTA arm was $2,138 compared to $3,458 in the conventional arm. This trial demonstrated the feasibility of effective triage of a chest pain patient with early door to diagnosis leading to early discharge with lesser radiation exposure. CCTA has great promise in detection of CAD in patients with a low pre-test probability and these constitute a large number of patients coming to the ER of community hospitals.
It may also be very useful in patients with atypical chest pain with left bundle branch block (LBBB) where frequent coronary angiography is performed to exclude CAD. Caussin et alCitation52 evaluated the role of 64-slice CCTA in 66 patients with LBBB and found a sensitivity of 97%, specificity of 95%, and NPV of 97% for detection of CAD with 50% stenosis. Similarly, it showed a 100% sensitivity and 92% specificity for detection of CAD in subsets of aortic stenosis (AS).Citation53 Frequently, these patients with equivocal stress test or new onset of congestive heart failure (CHF) are admitted to the hospital for exclusion of significant CAD. CCTA combined with myocardial perfusion imaging has been increasingly used in intermediate risk patients. This allows simultaneous functional and anatomic assessment of CAD.Citation54 Its role in assessing myocardial viability is being investigated to identify acute and old MI.Citation55 With its spatial resolution, CCTA’s emerging role is being explored in the assessment of aortic valve anatomy and pathology.Citation56,Citation57 Other applications of CCTA include evaluation of pericardial and myocardial diseases as listed in .
Role of CCTA in subclinical atherosclerosis (SCA)
A recent study by Pundzuite et al showed that nonobstructive coronary disease on CCTA can lead to higher cardiovascular events as compared to patients without atherosclerotic plaque.Citation58 Therefore, detection of sub-clinical atherosclerosis may lead to aggressive risk factor modification and a reduction in CAD burden of the general population. While this approach may save lives and money in the long term, immediate concerns are the expense of CCTA and the radiation issue. Meanwhile, CAC appears to be an excellent screening test for detection of sub-clinical CAD.
Detection of vulnerable plaque
The detection of vulnerable plaque leading to coronary events is of great interest. Detection of asymptomatic CAD has been debated since the publication of the Screening for Heart Attack Prevention and Education (SHAPE) Task Force report.Citation59 Although invasive coronary angiography can grossly identify morphologic features such as luminal thrombosis, calcification, and plaque disruption, it fails to delineate qualitative features of the plaque predictive of rupture.Citation60 While calcified plaque may be detected by CAC, the role of CCTA is evolving into the evaluation of soft plaque which may be the vulnerable plaque.
Small numbers of validation studies have demonstrated the accuracy of CCTA for imaging noncalcified plaque with sensitivity ranging from 80%–90%.Citation61–Citation65 Certain indicators of vulnerable plaque, such as vessel remodeling or a high plaque volume noted on CCTA, may help predict ischemic events.Citation65,Citation66 Several small studies in ACS have found have a higher percentage of noncalcified plaque and positive remodeling in patients with ACS compared to stable angina.Citation67–Citation69 In most patients, AMI may be the first clinical manifestation of sub-clinical plaque rupture or erosion.Citation70
There has been great debate in regard to imaging of this vulnerable plaque. Major technologies which can help image this plaque include intravascular ultrasound (IVUS), MRI, positron emission tomography (PET) imaging, and CCTA or MDCT.Citation71 Increased carotid artery intimal thickness noted in ultrasound studies has been a marker of cardiovascular and cerebral atherosclerosis.Citation72 Molecular imaging techniques have used radio-labeled molecules to detect the biological activity of plaques such as radioactive-labeled lipoproteins.Citation73 IVUS of coronary plaques is useful in the evaluation of vulnerable plaques. CCTA has also been compared favorably with IVUS in the measurement of atherosclerotic plaque and lumen area.Citation74 CCTA certainly appears to be promising in the evaluation of plaque characteristics and associated arterial remodeling.Citation75 Recently a prospective study demonstrated that patients with positively remodeled arteries with low attenuation plaques on CT angiography were at a higher risk of developing ACS in the subsequent follow up period.Citation76
Radiation issues
With emerging indications of CCTA, there is concern about the long term effect of radiation. Current CT scan use for various studies is expected to contribute to a large number of future malignancies and it is estimated that 29,000 future cancers are possibly related to all CT scans done in 2007.Citation77 Therefore, any radiation exposure should always be a concern for risk. One should familiarize oneself with the background radiation and the radiation associated with the commonly used tests in cardiology practiceCitation78–Citation81 as shown in . Given this carcinogenic potential of radiation, health care workers who prescribe this radiation must be fully aware of radiation risks. They should have a full understanding of effective dose concept which is a standard of measure of exposure expressed in millisievert (mSv). Effective dose is the sum of weighted equivalent doses in all the organs and tissues during a particular scan. Due to higher doses delivered to lungs and female breast in CCTA, there is a higher carcinogenic effect on these organs. This risk is higher in younger patients and more in women than in men. It is conceivable that in the near future patients may carry an “imaging card” reflecting the cumulative dose of radiation received by an individual patient which may be a factor to consider while ordering additional imaging studies requiring more radiation exposure.
Table 3 Dose of radiation in different cardiac procedures
Better scanners and software have contributed significantly to reduction in radiation exposure. Many dose reducing technical advances are available on 64-slice scans. These include cardiac filter modes, bowtie filters, and newer protocols such as ECG-triggered dose modulation and prospective gating. Quality control of scanners regarding the radiation issue is also very important. Recording of radiation dose for every patient in mSv should be mandatory and if there is a significant deviation from the published data, individual protocols in a given CCTA program should be reviewed. Government regulations via Environmental Protection Agency (EPA) require monitoring of credentials of ordering personnel, justified indications, and regular equipment check for minimum exposure and stringent indications for pregnant patients. For example, federal standards state that the radiation dose to an unborn child cannot exceed 5 mSv over a nine-month period. This is because unborn children have rapidly growing cells and are therefore most sensitive to radiation.
Preparation for CCTA program
Meticulous preparation of the patient for CCTA is the key to obtaining a diagnostic image which would aid the management of patients with acute or chronic cardiac problems. Guidelines are listed in and these may vary depending upon capabilities of the scanner such as single source or dual sources.Citation82 As part of starting a CCTA program appropriate guidelines for documentation of competenceCitation83 should be delineated as a part of a quality control program. A scanner must be staffed by highly skilled and qualified technologists. Staff and physicians should be knowledgeable in the issues of radiation exposure, CT scan collimation, temporal resolution, and spatial resolution. Achieving a target heart rate of 60–70 is important for adequate images by a single source system.Citation84 Pre-scan use of nitroglycerine is helpful for visualization of distal coronary arteries due to a 20% increase in the resultant diameter of coronary arteries.Citation85
Table 4 General guidelines
Quality control during acquisition of images is very important and staff should be knowledgeable of all the technical parameters such as table speed (pitch), window setting, level setting, reconstructions, post-processing, and image manipulations. A thorough understanding of contrast injection methods, adverse reactions, and contrast kinetics is critical. It is very important to understand how to overcome challenges of contrast-enhanced imaging of the left heart and surrounding structures. In high risk patients an iso-osmolar contrast such as Visipaque® should be selected as its viscosity is the same as blood, 290 m osmols/kg H20. All other contrast media have an osmolality of more than 600 m osmols/kg H20.
Instruction and education of the patient regarding CCTA is crucial in obtaining adequate images. Occasionally, simple obstacles such as the patient’s inability to raise the arm above the head to move arms out the FOV or inability to hold their breath may be a relative contraindication for coronary imaging by CCTA. It is also crucial to exclude patients with known levels of high CAC score as CCTA images may be nonevaluable.Citation86
Conclusion
The revolution of noninvasive imaging of the heart has taken a giant leap forward with widespread availability of the 64-slice CT, and now 256 and 320-slice CT scanners. The resultant superior spatial resolution, with improved temporal resolution with faster gantry rotation and dual source heads, offer the potential for remarkable improvement in sensitivity, specificity, and NPV in the diagnosis of CAD. Future generation scanners may provide an opportunity for first line imaging of CAD. Thus in patients presenting with chest pain, CCTA may be able to assess coronary lumen of calcified or noncalcified plaque and further evaluate other life threatening conditions such as AD and PE. The ‘triple rule out’ examination holds promise for revolutionizing the imaging of patients with acute chest pain in the ER. With wide spread availability in community hospitals, CCTA is likely to be embraced as the noninvasive triage tool of choice in the ER. Furthermore, a significant improvement in quality of care, cost-effectiveness, and medico-legal liability may be accomplished with future CCTA use in the ER. The key to implementation of such CCTA programs will be ‘central reading stations’ for expert reading and advice to the ER physicians, available 24 hours a day, year round for all the remote community hospitals just like night hawk radiology (Teleradiology).
Disclosure
The authors report no conflicts of interest in this work.
References
- PittsSRNiskaRWXuJBurtCWNational Hospital Ambulatory Medical Care Survey: 2006 emergency department summaryNational Health Statistics Reports2008720
- FlohrTGMcColloughCHBruderHFirst performance evaluation of a dual-source CT (DSCT) systemEur Radiol200616225626816341833
- DeyDLeeCJOhbaMImage quality and artifacts in coronary CT angiography with dual-source CT: initial clinical experienceJ Cardiovasc Comput Tomogr20082210511419083930
- FinebergHVScaddenDGoldmanLCare of patients with a low probability of acute myocardial infarction. Cost effectiveness of alternatives to coronary-care-unit admissionN Engl J Med198431020130113076425687
- McCarthyBDWongJBSelkerHPDetecting acute cardiac ischemia in the emergency department: a review of the literatureJ Gen Intern Med1990543653732197378
- PopeJHAufderheideTPRuthazerRMissed diagnoses of acute cardiac ischemia in the emergency departmentN Engl J Med2000342161163117010770981
- LeeTHRouanGWWeisbergMCClinical characteristics and natural history of patients with acute myocardial infarction sent home from the emergency roomAm J Cardiol19876042192243618483
- McCarthyBDBeshanskyJRD’AgostinoRBSelkerHPMissed diagnoses of acute myocardial infarction in the emergency department: results from a multicenter studyAnn Emerg Med19932235795828442548
- TatumJLJesseRLKontosMCComprehensive strategy for the evaluation and triage of the chest pain patientAnn Emerg Med19972911161258998090
- ReillyBMEvansATSchaiderJJImpact of a clinical decision rule on hospital triage of patients with suspected acute cardiac ischemia in the emergency departmentJAMA2002288334235012117399
- SelkerHPZalenskiRJAntmanEMAn evaluation of technologies for identifying acute cardiac ischemia in the emergency department: a report from a National Heart Attack Alert Program Working GroupAnn Emerg Med199729113878998086
- GershlickAHde BelderMChambersJRole of non-invasive imaging in the management of coronary artery disease: an assessment of likely change over the next 10 years. A report from the British Cardiovascular Society Working GroupHeart200793442343117401065
- FlemingRMKirkeeideRLSmallingRWGouldKLPatterns in visual interpretation of coronary arteriograms as detected by quantitative coronary arteriographyJ Am Coll Cardiol19911849459511894868
- AntmanEMCohenMBerninkPJThe TIMI risk score for unstable angina/non-ST elevation MI: A method for prognostication and therapeutic decision makingJAMA2000284783584210938172
- PeelsCHVisserCAKupperAJVisserFCRoosJPUsefulness of two-dimensional echocardiography for immediate detection of myocardial ischemia in the emergency roomAm J Cardiol199065116876912316447
- SabiaPAfrooktehATouchstoneDAKellerMWEsquivelLKaulSValue of regional wall motion abnormality in the emergency room diagnosis of acute myocardial infarction. A prospective study using two-dimensional echocardiographyCirculation1991843 SupplI85921884510
- HellerGVStowersSAHendelRCClinical value of acute rest technetium-99m tetrofosmin tomographic myocardial perfusion imaging in patients with acute chest pain and non-diagnostic electrocardiogramsJ Am Coll Cardiol1998315101110179562001
- UdelsonJEBeshanskyJRBallinDSMyocardial perfusion imaging for evaluation and triage of patients with suspected acute cardiac ischemia: a randomized controlled trialJAMA2002288212693270012460092
- ArpasiPJBisKGShettyANWhiteRDSimonettiOPMR angiography of the thoracic aorta with an electrocardiographically triggered breath-hold contrast-enhanced sequenceRadiographics200020110712010682776
- KwongRYSchussheimAERekhrajSDetecting acute coronary syndrome in the emergency department with cardiac magnetic resonance imagingCirculation2003107453153712566362
- O’MalleyPGTaylorAJJacksonJLDohertyTMDetranoRCPrognostic value of coronary electron-beam computed tomography for coronary heart disease events in asymptomatic populationsAm J Cardiol200085894594810760331
- RaggiPCallisterTQCooilBIdentification of patients at increased risk of first unheralded acute myocardial infarction by electron-beam computed tomographyCirculation2000101885085510694523
- WongNDHsuJCDetranoRCDiamondGEisenbergHGardinJMCoronary artery calcium evaluation by electron beam computed tomography and its relation to new cardiovascular eventsAm J Cardiol200086549549811009264
- AradYSpadaroLAGoodmanKNewsteinDGuerciADPrediction of coronary events with electron beam computed tomographyJ Am Coll Cardiol20003641253126011028480
- McLaughlinVVBaloghTRichSUtility of electron beam computed tomography to stratify patients presenting to the emergency room with chest painAm J Cardiol1999843327328A32810496445
- GeorgiouDBudoffMJKauferEKennedyJMLuBBrundageBHScreening patients with chest pain in the emergency department using electron beam tomography: a follow-up studyJ Am Coll Cardiol200138110511011451257
- SimonsDBSchwartzRSEdwardsWDSheedyPFBreenJFRumbergerJANoninvasive definition of anatomic coronary artery disease by ultrafast computed tomographic scanning: a quantitative pathologic comparison studyJ Am Coll Cardiol1992205111811261401612
- RumbergerJASchwartzRSSimonsDBSheedyPF3rdEdwardsWDFitzpatrickLARelation of coronary calcium determined by electron beam computed tomography and lumen narrowing determined by autopsyAm J Cardiol19947316116911738203333
- KaufmannRBPeyserPASheedyPFRumbergerJASchwartzRSQuantification of coronary artery calcium by electron beam computed tomography for determination of severity of angiographic coronary artery disease in younger patientsJ Am Coll Cardiol19952536266327860906
- RumbergerJASimonsDBFitzpatrickLASheedyPFSchwartzRSCoronary artery calcium area by electron-beam computed tomography and coronary atherosclerotic plaque area. A histopathologic correlative studyCirculation1995928215721627554196
- RumbergerJASheedyPF3rdBreenJFSchwartzRSCoronary calcium, as determined by electron beam computed tomography, and coronary disease on arteriogram. Effect of patient’s sex on diagnosisCirculation1995915136313677867174
- MolletNRCademartiriFNiemanKMultislice spiral computed tomography coronary angiography in patients with stable angina pectorisJ Am Coll Cardiol200443122265227015193691
- NiemanKCademartiriFLemosPARaaijmakersRPattynamaPMde FeyterPJReliable noninvasive coronary angiography with fast submillimeter multislice spiral computed tomographyCirculation2002106162051205412379572
- RopersDBaumUPohleKDetection of coronary artery stenoses with thin-slice multi-detector row spiral computed tomography and multiplanar reconstructionCirculation2003107566466612578863
- MartuscelliERomagnoliAD’EliseoAAccuracy of thin-slice computed tomography in the detection of coronary stenosesEur Heart J200425121043104815191775
- RaffGLGallagherMJO’NeillWWGoldsteinJADiagnostic accuracy of noninvasive coronary angiography using 64-slice spiral computed tomographyJ Am Coll Cardiol200546355255716053973
- VanhoenackerPKHeijenbrok–KalMHVan HesteRDiagnostic performance of multi-detector CT angiography for assessment of coronary artery disease: meta-analysisRadiology2007244241942817641365
- SunZDiagnostic accuracy of multislice CT angiography in peripheral arterial diseaseJ Vasc Interv Radiol200617121915192117185686
- SchoenhagenPWhiteRDNissenSETuzcuEMCoronary imaging: angiography shows the stenosis, but IVUS, CT, and MRI show the plaqueCleve Clin J Med200370871371912959398
- HalliburtonSSPetersilkaMSchvartzmanPRObuchowskiNWhiteRDEvaluation of left ventricular dysfunction using multiphasic reconstructions of coronary multi-slice computed tomography data in patients with chronic ischemic heart disease: validation against cine magnetic resonance imagingInt J Cardiovasc Imaging2003191738312602485
- BudoffMJGeorgiouDBrodyAUltrafast computed tomography as a diagnostic modality in the detection of coronary artery disease: a multicenter studyCirculation19969358989048598080
- GallagherMJRossMARaffGLGoldsteinJAO’NeillWWO’NeilBThe diagnostic accuracy of 64-slice computed tomography coronary angiography compared with stress nuclear imaging in emergency department low-risk chest pain patientsAnn Emerg Med200749212513616978738
- KimuraSKakutaTKuboyamaOMultisclice computed tomography for risk stratification in patients with suspected Non ST elevation acute coronary syndrome [abstract]Circulation2004110Supp III
- LidaKSataYMatsumotoNUsefulness of multislice computed tomography to identify acute coronary in the emergency department [abstract]Circulation2004110Supp III
- HoffmannUBambergFChaeCUCoronary computed tomography angiography for early triage of patients with acute chest pain: the ROMICAT (Rule Out Myocardial Infarction using Computer Assisted Tomography) trialJ Am Coll Cardiol200953181642165019406338
- HlatkyMAEvaluating use of coronary computed tomography angiography in the emergency departmentJ Am Coll Cardiol200953181651165219406339
- WhiteCSKuoDKelemenMChest pain evaluation in the emergency department: can MDCT provide a comprehensive evaluation?AJR Am J Roentgenol2005185253354016037533
- SatoYMatsumotoNIchikawaMEfficacy of multislice computed tomography for the detection of acute coronary syndrome in the emergency departmentCirc J20056991047105116127184
- HoffmannUNagurneyJTMoselewskiFCoronary multidetector computed tomography in the assessment of patients with acute chest painCirculation2006114212251226017075011
- WhiteCReadKKuoDAssessment of chest pain in the emergency room: what is the role of multidetector CT?Eur J Radiol200657336837216434159
- American Heart Association newsroom [online]. [cited 2009, Nov 18]. Available from: http://americanheart.mediaroom.com/index.php?s=54&item=217
- CaussinCLarchezCGhostineSComparison of coronary minimal lumen area quantification by 64-slice computed tomography versus intravascular ultrasound for intermediate stenosisAm J Cardiol200698787187616996865
- MeijboomWBMolletNRVan MieghemCAPre-operative computed tomography coronary angiography to detect significant coronary artery disease in patients referred for cardiac valve surgeryJ Am Coll Cardiol20064881658166517045904
- DanciuSCHerreraCJStecyPJCarellESaltielFHinesJLUsefulness of multislice computed tomographic coronary angiography to identify patients with abnormal myocardial perfusion stress in whom diagnostic catheterization may be safely avoidedAm J Cardiol2007100111605160818036355
- LardoACCordeiroMASilvaCContrast-enhanced multidetector computed tomography viability imaging after myocardial infarction: characterization of myocyte death, microvascular obstruction, and chronic scarCirculation2006113339440416432071
- PannuHKJacobsJELaiSFishmanEKGated cardiac imaging of the aortic valve on 64-slice multidetector row computed tomography: preliminary observationsJ Comput Assist Tomogr200630344344616778619
- GilkesonRCMarkowitzAHBalgudeASachsPBMDCT evaluation of aortic valvular diseaseAJR Am J Roentgenol2006186235036016423937
- PundziuteGSchuijfJDJukemaJWPrognostic value of multislice computed tomography coronary angiography in patients with known or suspected coronary artery diseaseJ Am Coll Cardiol2007491627017207724
- NaghaviMFalkEHechtHSFrom vulnerable plaque to vulnerable patient – part III: executive summary of the Screening for Heart Attack Prevention and Education (SHAPE) Task Force reportAm J Cardiol2006982A2H15H
- FalkEShahPKFusterVCoronary plaque disruptionCirculation19959236576717634481
- BeckerCRKnezAOhnesorgeBSchoepfUJReiserMFImaging of noncalcified coronary plaques using helical CT with retrospective ECG gatingAJR Am J Roentgenol2000175242342410915687
- SchoenhagenPTuzcuEMStillmanAENon-invasive assessment of plaque morphology and remodeling in mildly stenotic coronary segments: comparison of 16-slice computed tomography and intravascular ultrasoundCoron Artery Dis200314645946212966267
- LeberAWKnezABeckerAAccuracy of multi-detector spiral computed tomography in identifying and differentiating the composition of coronary atherosclerotic plaques: a comparative study with intracoronary ultrasoundJ Am Coll Cardiol20044371241124715063437
- AchenbachSMoselewskiFRopersDDetection of calcified and noncalcified coronary atherosclerotic plaque by contrast-enhanced, submillimeter multi-detector spiral computed tomography: a segment-based comparison with intravascular ultrasoundCirculation20041091141714691045
- AchenbachSRopersDHoffmannUAssessment of coronary remodeling in stenotic and nonstenotic coronary atherosclerotic lesions by multi-detector spiral computed tomographyJ Am Coll Cardiol200443584284714998627
- LeberAWBeckerAKnezAAccuracy of 64-slice computed tomography to classify and quantify plaque volumes in the proximal coronary system: a comparative study using intravascular ultrasoundJ Am Coll Cardiol200647367267716458154
- LeberAWKnezAWhiteCWComposition of coronary atherosclerotic plaques in patients with acute myocardial infarction and stable angina pectoris determined by contrast-enhanced multislice computed tomographyAm J Cardiol200391671471812633805
- InoueFSatoYMatsumotoNTaniSUchiyamaTEvaluation of plaque texture by means of multislice computed tomography in patients with acute coronary syndrome and stable anginaCirc J200468984084415329505
- HoffmannUMoselewskiFNiemanKNoninvasive assessment of plaque morphology and composition in culprit and stable lesions in acute coronary syndrome and stable lesions in stable angina by multidetector computed tomographyJ Am Coll Cardiol20064781655166216631006
- VirmaniRBurkeAPFarbAKolodgieFDPathology of the vulnerable plaqueJ Am Coll Cardiol2006478 SupplC13C1816631505
- ChenJWWassermanBAVulnerable plaque imagingNeuroimaging Clin N Am2005153609621xi16360592
- O’LearyDHPolakJFIntima-media thickness: a tool for atherosclerosis imaging and event predictionAm J Cardiol20029010C18L21L
- LangerHFHaubnerRPichlerBJGawazMRadionuclide imaging: a molecular key to the atherosclerotic plaqueJ Am Coll Cardiol200852111218582628
- LeberAWKnezAvon ZieglerFQuantification of obstructive and non-obstructive coronary lesions by 64-slice computed tomography: a comparative study with quantitative coronary angiography and intravascular ultrasoundJ Am Coll Cardiol200546114715415992649
- AchenbachSCan CT detect the vulnerable coronary plaque?Int J Cardiovasc Imaging200824331131218026848
- MotoyamaSSaraiMHarigayaHComputed tomographic angiography characteristics of atherosclerotic plaques subsequently resulting in acute coronary syndromeJ Am Coll Cardiol2009541495719555840
- Berrington de GonzalezAMaheshMKimKPProjected cancer risks from computed tomographic scans performed in the United States in 2007Arch Intern Med2009169222071207720008689
- HunoldPVogtFMSchmermundARadiation exposure during cardiac CT: effective doses at multi-detector row CT and electron-beam CTRadiology2003226114515212511683
- CuryRCFeutchnerGPenaCSJanowitzWRKatzenBTZifferJAAcute chest pain imaging in the emergency department with cardiac computed tomography angiographyJ Nucl Cardiol200815456457518674724
- BetsouSEfstathopoulosEPKatritsisDFaulknerKPanayiotakisGPatient radiation doses during cardiac catheterization proceduresBr J Radiol1998718466346399849387
- MorinRLGerberTCMcColloughCHRadiation dose in computed tomography of the heartCirculation2003107691792212591765
- HalliburtonSSAbbaraSPractical tips and tricks in cardiovascular computed tomography: patient preparation for optimization of cardiovascular CT data acquisitionJ Cardiovasc Comput Tomogr200711626519083880
- BudoffMJCohenMCGarciaMJACCF/AHA clinical competence statement on cardiac imaging with computed tomography and magnetic resonance: a report of the American College of Cardiology Foundation/American Heart Association/American College of Physicians Task Force on Clinical Competence and TrainingJ Am Coll Cardiol200546238340216022977
- GieslerTBaumURopersDNoninvasive visualization of coronary arteries using contrast-enhanced multidetector CT: influence of heart rate on image quality and stenosis detectionAJR Am J Roentgenol2002179491191612239036
- DeweyMHoffmannHHammBMultislice CT coronary angiography: effect of sublingual nitroglycerine on the diameter of coronary arteriesRofo2006178660060416703495
- OngTKChinSPLiewCKAccuracy of 64-row multidetector computed tomography in detecting coronary artery disease in 134 symptomatic patients: influence of calcificationAm Heart J200615161323e1321e132616781246