

Abstract
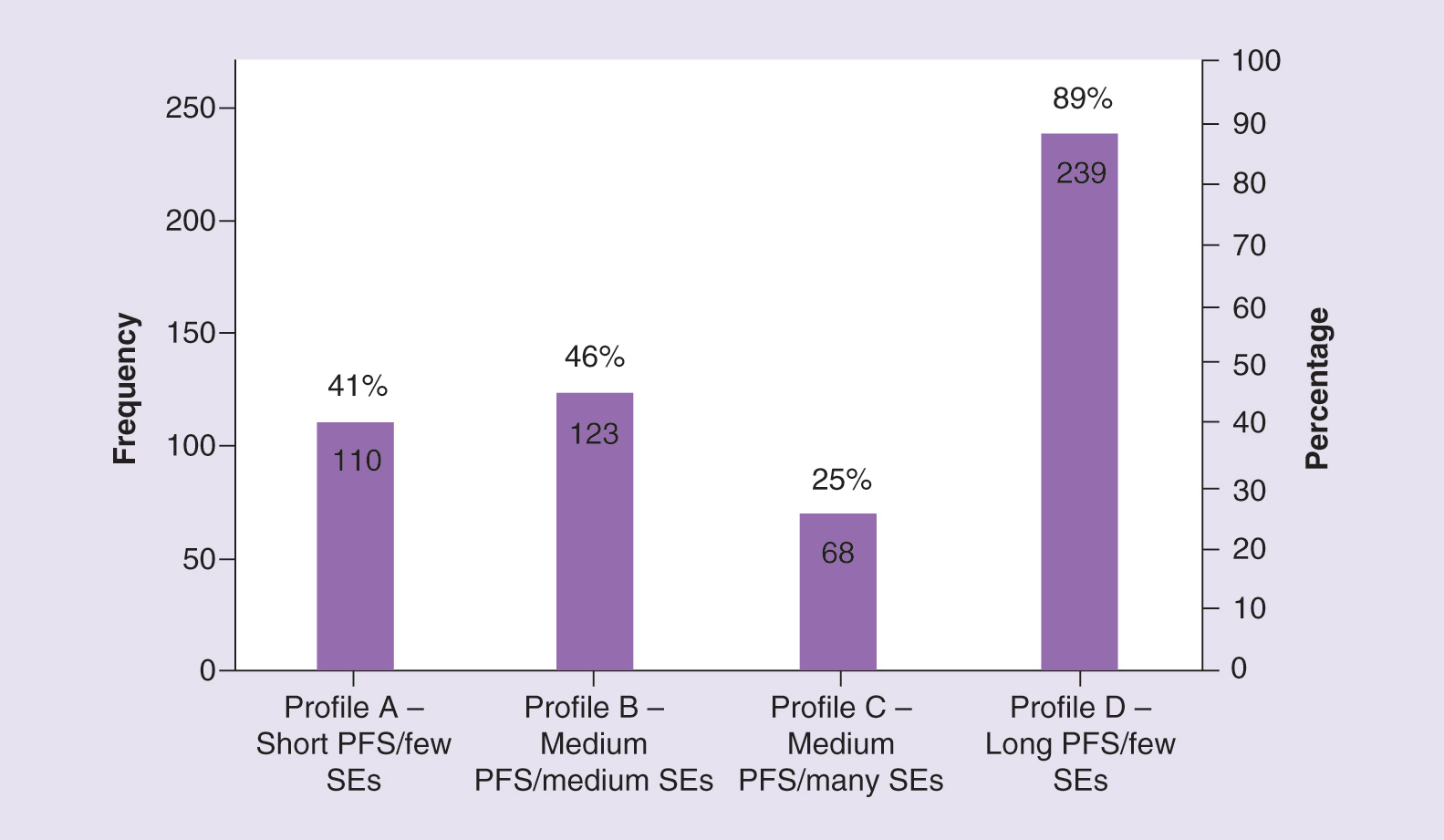
Aim: EGFR-tyrosine kinase inhibitors (TKIs) vary in efficacy, side effects (SEs) and dosing regimen. We explored EGFR-TKI treatment attribute preferences in EGFR mutation-positive metastatic non-small-cell lung cancer. Materials & methods: Patients completed a survey utilizing preference elicitation methods: direct elicitation of four EGFR-TKI profiles describing progression-free survival (PFS), severe SE risk, administration; discrete choice experiment involving 12 choice tasks. Results: 90 participated. The preferred profile (selected 89% of times) had the longest PFS (18 months) and the lowest severe SE risk (5%). Patients would need compensation with ≥three-times longer PFS for severe SEs. Patients would accept ≤7 months PFS reduction for oral treatments versus intravenous. Conclusion: Patients preferred longer PFS but were willing to accept reduced PFS for more favorable SEs and dosing convenience.
Lay abstract
EGFR-TKIs are drugs used to treat a type of non-small-cell lung cancer with a change (mutation) in a gene called EGFR. The way the drug is taken by patients, its effectiveness and side effects are different for each EGFR-TKI. 90 patients with non-small-cell lung cancer containing the EGFR mutation took part in our study. Patients completed an online survey to choose which EGFR-TKI treatment traits are most important to them. We found that patients prefer treatments that offer them longer lengths of time before their cancer worsens; however, patients are willing to accept shorter lengths of time before their cancer worsens if the treatment has fewer side effects and is easier to take.
Graphical abstract
Data sharing statement
Data underlying the findings described in this manuscript may be obtained in accordance with AstraZeneca’s data sharing policy described at https://astrazenecagrouptrials.pharmacm.com/ST/Submission/Disclosure
Financial and competing interests disclosure
This research was funded by AstraZeneca US. JFP Bridges has acted as a consultant for ICON, received research grants from LUNGevity Foundation and received personal fees from Bayer, Boehringer Ingelheim and AstraZeneca. M de la Cruz and EM Janssen are employees of ICON. N Chehab is an employee of AstraZeneca. E Flood was an employee of ICON at the time of study, and is an employee of AstraZeneca. M Pavilack and AW Fernandes are employees of, and shareholders in, AstraZeneca. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
The authors acknowledge Natasha Cary of iMed Comms, Macclesfield, UK, an Ashfield Company, part of UDG Healthcare plc, for technical editing support that was funded by AstraZeneca in accordance with Good Publications Practice (GPP3) guidelines (http://www.ismpp.org/gpp3).
Ethical conduct of research
The study protocol was approved by an institutional review board (Salus IRB, TX, USA). An Informed Consent Form (ICF) was sent to the participants to review, sign and return prior to the interview.