
Abstract
Aim: Real-world data on outcomes for early-stage non-small-cell lung cancer (NSCLC) are needed to better understand the benefits of new therapies. Methods: In this retrospective study using the ConcertAI Patient360™ database, overall survival and healthcare resource utilization were compared among patients with recurrent and non-recurrent completely resected stage IB-IIIA NSCLC. Results: Recurrence was associated with a shorter median overall survival compared with non-recurrence (31.5 months vs 75.6 months, respectively), lower survival probability 5-years post-resection, and higher healthcare resource utilization. Patients with late recurrence had a longer restricted mean survival time versus patients with early recurrence. Conclusion: Results from this real-world study highlight the potential value of preventing or delaying recurrence in patients with early-stage NSCLC.
Plain language summary
This study looked at how people with early-stage non-small-cell lung cancer did after surgery to completely remove the disease. It compared two groups of patients: those whose disease came back after surgery and those whose disease did not come back after surgery. The group of people whose disease came back after surgery did not live as long as those whose disease did not come back after surgery (31.5 months vs 75.6 months). Patients whose disease came back had a lower chance of living at least 5 years after surgery and they had more hospital visits and doctor’s office visits. In addition, those whose disease came back within 1 year did not live as long as those whose disease came back between 1 and 5 years after surgery. Preventing or delaying the return of disease after surgery is important for improving the lives of patients with early-stage non-small-cell lung cancer.
Tweetable abstract
A real-world study reported that lung cancer recurrence after surgery leads to shorter lifespans and higher healthcare utilization, emphasizing the need for recurrence prevention to improve survival and economic benefits.
There are expected to be more than 230,000 new cases of lung cancer and over 130,000 deaths in the USA in 2022 [Citation1], of which 80–85% will be non-small-cell lung cancer (NSCLC) [Citation2]. Of these, 25–30% will likely be diagnosed with localized or regional early-stage disease [Citation3,Citation4].
Despite complete resection with microscopically negative margins (R0), 30–50% of patients with early-stage disease will experience a recurrence, even with pre- and/or post-operative chemotherapy [Citation5–8]. In one retrospective study of patients with stage I to II NSCLC, 26% of patients experienced disease recurrence during a median follow-up of 33 months [Citation9]. In another study, 45.2% of patients with stage II to IIIB disease experienced a recurrence within a median follow-up of 13.7 months post-resection [Citation10].
In addition to having a high rate of recurrence, patients with early-stage NSCLC with complete resection also have poor overall survival (OS). Based on National Cancer Institute data between 2012 and 2018, the 5-year survival rate of patients with localized NSCLC is 61.2%. For patients with regional disease, it is only 33.5% [Citation11]. Predictors of OS after resection include type of resection surgery (wedge resection and segmentectomy were associated with higher risk), more advanced stage of disease [Citation12], poor histological grade, older age, male sex [Citation13–16] and prior recurrence [Citation10].
Previous studies have investigated the relationship between recurrence and OS in patients with early-stage NSCLC. A study by Cai and colleagues that examined electronic health records for patients in the USA with stage II–IIIB NSCLC who were at high risk of relapse with adjuvant chemotherapy between June 2008 and April 2017 found that patients with a recurrence had three-times the risk of death in the follow-up period compared with patients without recurrence [Citation10]. Findings from this study, however, do not take into account the potential immortal time bias that may be present in evaluating OS. Additionally, the timing of recurrence after resection was reported to impact survival time post-resection in a prospective, observational, multi-center study in Japan. The study reported that recurrence within 1 year of resection was associated with decreased survival time compared with recurrence more than 1 year post-resection (hazard ratio [HR] = 1.566; p < 0.001) [Citation17].
These studies are limited, however, in that they do not address the relationship between recurrence and OS among all patients who were eligible for resection (stage IB-IIIA) regardless of adjuvant chemotherapy status or risk of relapse. Additionally, the impact of delaying time to recurrence is also not fully elucidated, and methods to address potential immortal time bias, such as landmark analysis, to our knowledge, have not been previously utilized. Further research that addresses these gaps is warranted, particularly using more recent and inclusive high-quality data.
Recurrence after resection can also be associated with increased healthcare resource utilization (HCRU) in this population. An observational study in the USA of 456 patients with early-stage NSCLC reported that only 25% of patients who experienced a recurrence visited an emergency department (ED) prior to recurrence, but 40% had at least one ED visit after recurrence [Citation10]. However, this study did not address the differences between patients who experienced a recurrence and patients who did not, and only included patients at a high risk of recurrence. In addition, a burden of illness study conducted by Andreas and colleagues in France, Germany, and the UK found increased utilization of physician visits, receipt of radiology, ED visits and hospitalizations after recurrence, particularly for patients with distant metastatic recurrence compared with patients with locoregional recurrence [Citation18]. However, as above, this study did not evaluate the differences in HCRU between patients who experience a recurrence and patients who did not, and instead was limited to patients whose disease recurred.
New therapy options are emerging for patients with early-stage NSCLC in the adjuvant setting. The ADAURA [Citation19] and IMpower010 [Citation20] phase III clinical trial results demonstrated the efficacy of osimertinib and atezolizumab. These pivotal trials led to the approval of both agents by the US FDA [Citation21,Citation22] and European Medicines Agency [Citation23,Citation24]. Pembrolizumab has also shown efficacy in the adjuvant setting in the KEYNOTE-091 phase III clinical trial [Citation25].
While there has been research regarding OS and recurrence in patients with early-stage NSCLC who have received adjuvant treatment, studies in the broader population of patients with completely resected early-stage NSCLC are more limited [Citation10,Citation17,Citation18]. More research is needed that examines recurrence rate, impact of recurrence rate on OS, impact of delaying time to recurrence on OS, and the association of recurrence with HCRU, among patients with completely resected early-stage NSCLC regardless of receipt of adjuvant chemotherapy.
The aim of this study was to report the clinical and economic impact of recurrence in patients with completely resected stage IB-IIIA NSCLC with and without recurrence, and to examine how the timing of the recurrence impacts post-recurrence OS, using recent real-world data from a US-based population. The study also sought to control for the immortal time bias introduced by the latency to recurrence after complete resection by using landmark analysis and through index date matching between patients who experience a recurrence and those who do not experience a recurrence.
Materials & methods
Study design & patients
This was a retrospective, non-interventional cohort study using electronic medical record (EMR) data from the ConcertAI Patient360™ database, which consists of de-identified data including structured and unstructured data (text and image documents, e.g., physician notes) from selected patient cohorts. Experienced Clinical Research Nurses (CRN) curated the information directly from the unstructured documents. An independent quality control review was conducted on the data curated in the ConcertAI Patient360™ database to evaluate for consistency, completeness, and outlier values. Data were drawn from geographically diverse practice locations within the USA, primarily community oncology practices (80–90%) from both rural and urban centers (Supplemental Figure 1). Any unique identifying patient information was fully removed from the analytical dataset, and only de-identified data were used in the analysis. As this was a retrospective study that utilized secondary data and involved no direct contact with individual patients, informed consent of patients was not applicable. This research project was reviewed by an institutional review board (IRB; Advarra, MD, USA) and found to be exempt from IRB oversight.
Patients with a primary diagnosis of stage IB-IIIA NSCLC were eligible if they had undergone complete resection prior to 1 March 2016, to allow a minimum 5-year theoretical follow-up through 1 March 2021, the end of data availability – a date that was later extended to 1 July 2021. Complete resection for this study was defined as having a documented residual tumor stage of R0 post-resection. Case eligibility regarding diagnosis, staging, complete resection and disease recurrence was verified through manual review of EMR data by trained CRNs, who participated in study-specific training to reduce potential bias in the curation process. Patients with prior neoadjuvant chemotherapy or radiotherapy, or record of participation in an interventional clinical trial at any time were excluded from the study.
Patients with an Eastern Cooperative Oncology Group (ECOG) status of 0 or 1 at initial diagnosis were included to match the underlying target population of the KEYNOTE-091 clinical trial (mentioned above) [Citation25]. Although ECOG performance status may affect survival and may have economic implications, the ECOG 0 or 1 population was the primary population of interest. Including patients with an ECOG 2+ status would also have required more complex models with increased risk of overfitting. Accordingly, patients with an ECOG performance status of 2 or above were also excluded from the study cohort. In addition, patients without a formal ECOG indication, but with text evidence on manual review of impaired performance status, were also excluded.
To compare patients with and without recurrence, patients were assigned to a Recurrence Cohort or a Non-Recurrence Cohort. Disease recurrence and timing of recurrence were verified through manual review of the EMR data by CRNs. The Recurrence Cohort included patients with any recurrence event (locoregional recurrence or distant recurrence, based on provider documentation) or new diagnosis of another primary cancer other than non-melanoma skin cancer after complete resection. Patients with a new diagnosis of another primary cancer were included because it may be difficult at times to distinguish between a recurrence and new primary cancer. This helps ensure all recurrences were included and accounts for the fact that patients with a new primary cancer diagnosis would likely have poorer outcomes and increased HCRU. The recurrence event was considered the index date in this cohort. The Non-Recurrence Cohort included all other eligible patients and had a randomly assigned index date based on the distribution of the interval between complete resection and index date among patients in the Recurrence Cohort.
Statistical analysis
Comparison of baseline characteristics: recurrence versus non-recurrence cohorts
Descriptive statistics were used to summarize patient characteristics and to evaluate the differences between patients in the Recurrence Cohort and Non-Recurrence Cohort. Patient demographic and clinical characteristics, including age, gender, race, region, comorbidities, stage, histology and performance status, were assessed at the time of initial diagnosis. The date and type of surgery were captured at the time of resection. HCRU (number of monthly hospitalizations and offices visits) was assessed during the pre-index time period, defined as 12 months prior to index date or initial NSCLC diagnosis date to index date if the patient had a recurrence within 12 months after initial diagnosis. Adjuvant therapy use was assessed from date of resection to end of record. The descriptive statistics included means, standard deviations, medians, range for continuous variables and frequencies and percentages for categorical variables. Comparisons across groups for basic descriptive statistics were conducted using t-tests for continuous variables and Chi-square tests or Fisher’s Exact tests for categorical variables.
Overall survival comparisons: recurrence versus non-recurrence cohorts
Survival time in the Recurrence Cohort was measured from an index date defined as the date of the earliest recurrence event (locoregional recurrence or distant recurrence) or new diagnosis of another primary cancer other than non-melanoma skin cancer. Survival time in the Non-Recurrence Cohort was measured from an index date that was randomly assigned, based on the distribution of the interval between complete resection and index date among patients in the Recurrence Cohort. This approach was adopted to control for the immortal time bias associated with time to recurrence in the Recurrence Cohort. OS in this analysis was defined as the interval from the index date until the date of death. Patients were censored at the date of the last medical record if there was no evidence of death.
Landmark analyses of overall survival by recurrence status at 1, 3 & 5 year timepoints
Survival was also measured from defined landmarks. The landmark timepoints used in these analyses were 1, 3 and 5 years after complete resection. Patients were classified to the Recurrence and Non-Recurrence Cohorts in the landmark analyses based on recurrence status at the landmark timepoints, and patients were not included if they had experienced the terminal event, i.e. death, prior to the landmark timepoint. OS in this analysis was defined as the interval from the landmark timepoint until the date of death.
Kaplan-Meier method and Cox regression were utilized to compare patients in the Recurrence and Non-Recurrence Cohorts for analysis of OS from recurrence and from the landmarks. Statistical comparisons were performed using the log-rank test. Cox proportional hazards regression analyses controlled for stage at diagnosis, age at index date, gender, race, comorbid conditions with a frequency >5% of total patients, pre-index HCRU, disease histology and use of adjuvant chemotherapy. Monthly pre-index number of office visits and hospitalizations were examined as a proxy for baseline health status. The monthly pre-index number of office visits and hospitalizations were examined during the 12-month period prior to the index date, or from initial diagnosis to the index date if the patient had a recurrence within 12 months after initial diagnosis. All control variables were selected a priori.
Overall survival post recurrence in the recurrence cohort
The study also examined the effect on OS of the timing of recurrence. Patients who experienced a recurrence within 1 year after resection (early) were compared with patients who experienced a recurrence between 1 and 5 years after resection (late). OS in this analysis was defined as the interval from recurrence until the date of death. Restricted mean survival time (RMST) regression was used to compare survival through 5 years post-recurrence among patients with early versus late recurrence. RMST analysis did not include patients with recurrence later than 5 years post-resection due to the competing risks associated with other changes in clinical characteristics, such as comorbidities. RMST regression analyses controlled for stage at diagnosis, age at recurrence, gender, race, pre-index HCRU, use of adjuvant therapy and disease histology, all of which were selected for inclusion a priori.
Healthcare resource utilization in the recurrence versus non-recurrence cohorts
The study also evaluated HCRU from index date to end of record (post-index time period) in the Recurrence and Non-Recurrence Cohorts, where cohort membership and the index date were defined using the same criteria as for the OS analysis. HCRU events included the number of hospitalizations and number of medical office visits. These events were intended to serve as proxy indicators of cost and an indirect measure of economic impact, as utilization, and hospitalizations in particular, are a primary driver of overall healthcare costs. Incidence rates of HCRU were assessed as events per patient-month to account for different lengths of follow-up between patients. The total number of visits, either hospitalization or office visits, were divided by the total available time in months for each patient. Unadjusted HCRU was described as Incidence Rate Ratios (IRR) and compared between the Recurrence and Non-Recurrence Cohorts using univariable generalized linear models with a negative binomial distribution and a log-link function. Multivariate regression models were also conducted to calculate the adjusted IRR comparing the two cohorts to determine the impact of recurrence on the incidence rate of HCRU. The regression analyses controlled for recurrence status, stage at diagnosis, age at index date, gender, race, comorbid conditions with a frequency >5% of total patients, disease histology, pre-index HCRU and use of adjuvant chemotherapy. All control variables were selected a priori.
All analyses were conducted using SAS version 9.4 (SAS Institute Inc., NC, USA). All statistical tests were 2-sided, and p-values less than 0.05 were considered statistically significant.
Results
Patient characteristics
After applying all eligibility criteria, a total of 441 patients were included in this study, with 240 (54.4%) patients in the Recurrence Cohort and 201 (45.6%) patients in the Non-Recurrence Cohort (Supplemental Figure 2, ). Of note, only one patient had a new primary cancer as a recurrence event, a diagnosis of multiple myeloma. The remaining 239 patients in the Recurrence Cohort did not have any indication of a new primary cancer. The overall median follow-up time was 74.2 months (Interquartile range = 45.7 months, 94.9 months). Half of the patients in the Recurrence Cohort had a recurrence between 1 and 5 years after complete resection (49.6%), while 34.2% had a recurrence within 1 year after complete resection, and 16.2% had a recurrence more than 5 years after complete resection. The median age at index date was 69 years old for patients in both the Recurrence and Non-Recurrence Cohorts. The Recurrence Cohort had similar rates of patients at stage IB (32.9 vs 36.8%), stage II (38.3 vs 44.2%), and stage IIIA (22.9 vs 24.9%) disease compared with the Non-Recurrence Cohort. The Recurrence Cohort had a higher percentage of patients diagnosed with adenocarcinoma than the Non-Recurrence Cohort (41.7 vs 34.8%, p = 0.054). No statistically significant differences between these two groups were observed in HCRU in the baseline period or adjuvant therapy usage post-resection.
Table 1. Demographic and clinical characteristics of patients with non-small-cell lung cancer.
Overall survival from index date in recurrence versus non-recurrence cohorts
Unadjusted Kaplan-Meier analysis showed that among patients in the Recurrence Cohort, median OS from the index date was significantly shorter (31.5 months [95% CI: 27.4, 37.8]) compared with patients in the Non-Recurrence Cohort (75.6 months [95% CI: 58.4, 88.3]; p < 0.0001; ). The 5-year survival probability from the index date for those with a recurrence was much lower than that for those without any recurrence (28.5 vs 58.1%, respectively). After adjusting for key baseline characteristics using a Cox proportional hazards model, patients in the Recurrence Cohort had a risk of death 2.47-times as high as those in the Non-Recurrence Cohort (95% CI: 1.81, 3.37; p < 0.001; ).
†Recurrence cohort index date was defined as the date of the earliest recurrence event (locoregional recurrence or distance recurrence) or new diagnosis of another primary cancer other than non-melanoma skin cancer. Non-recurrence cohort index date was randomly assigned based on the distribution of time between complete resection and index date among patients in the recurrence cohort.
OS: Overall survival.
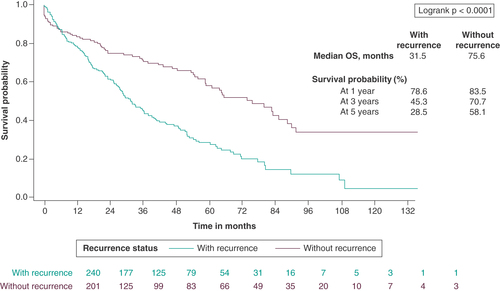
Table 2. Cox regression analysis of overall survival from index dateTable Footnote†: recurrence versus non-recurrence cohort.
Landmark analyses of overall survival by recurrence status
Recurrence was observed to be strongly associated with shorter OS from landmark points at 1, 3 and 5 years following complete resection (, Supplemental Figure 3). As measured from each timepoint, median OS for those without a recurrence by the landmark was more than double what was observed for those with a recurrence by the landmark (83.4 vs 29.1 months from 1 year, 75.6 vs 35.7 months from 3 years, and 64.7 vs 31.3 months from 5 years following complete resection). After adjusting for patient characteristics in the Cox models, patients with recurrence by each landmark had a risk of death three to four-times as high as patients without any recurrence up to the landmark (HR = 4.23 from 1 year, HR = 4.63 from 3 years, and HR = 2.97 from 5 years; all p < 0.001).
Table 3. Cox proportional hazard model results of overall survival between patients with and without recurrence by each landmark point after 1, 3 and 5 years following complete resection.
Overall survival post recurrence in recurrent patients
Although no statistically significant difference was observed in post-recurrence OS between patients who developed recurrence within 1 year and those who developed recurrence between 1 and 5 years after complete resection (p = 0.132; , ), a trend toward decreasing median OS post-recurrence was observed for patients who developed recurrence within 1 year of complete resection compared with those who developed recurrence between 1 and 5 years post-resection (24.1 months vs 39.1 months). In RMST models restricted to 5 years post-recurrence, after adjusting for baseline characteristics, the average survival time was 21.14 versus 25.79 months for patients who recurred within 1 year and patients who recurred between 1 and 5 years following surgery (p = 0.069). Older age at recurrence, more baseline hospitalizations, and diagnosis with squamous cell carcinoma were all associated with shorter OS through 5 years post-recurrence.
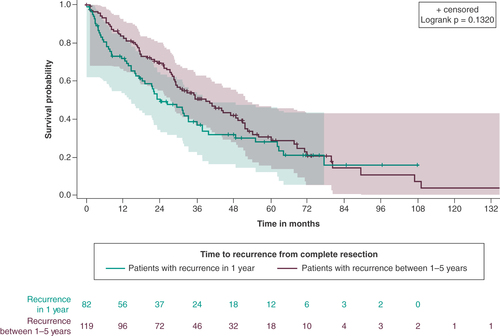
Table 4. Restricted mean survival time regression analysis of overall survival post recurrence.
Healthcare resource utilization by recurrence status
The incidence rate (visits/person-months) for hospitalizations and office visits were nominally higher in the unadjusted analysis among patients in the Recurrence Cohort compared with patients in the Non-Recurrence Cohort (0.05 vs 0.02; and 0.69 vs 0.35, respectively). In adjusted generalized linear models, patients in the Recurrence Cohort had statistically significantly more follow-up office visits (IRR = 2.17) and hospitalizations (IRR = 3.76; all p < 0.0001), indicating an incidence rate of office visits two-times as high as patients in the Non-Recurrence Cohort, and an incidence rate of hospitalization almost four-times as high as patients in the Non-Recurrence Cohort (Supplemental Table 1).
Discussion
This study aimed to describe the survival outcomes and HCRU associated with recurrence among patients with completely resected stage IB-IIIA NSCLC to highlight the potential clinical and economic value of preventing or delaying recurrence in this patient population. In this study, 54% of patients experienced a recurrence. This rate of recurrence is higher than the 45% reported by Cai and colleagues, which could be due to the longer follow-up in our study (74.2 months of follow-up in our study vs a median of 41 months in the Cai and colleagues study) [Citation10]. Multiple survival analyses were conducted to assess and quantify the impact of recurrence and of the timing of recurrence on patient survival.
This study adds to the literature by examining the impact of recurrence on OS in patients with completely resected early-stage NSCLC, and did so using multiple methods to manage immortal time bias. First, our study utilized a landmark analysis approach, which to our knowledge has not previously been used to examine this question, and it evaluated outcomes from several different landmarks, to evaluate the sensitivity of the findings to the selection of the landmark. This approach sought to control immortal time bias introduced by the timing of recurrence and assigned index date. Second, we used index date matching to further evaluate the magnitude of the effect of recurrence in the patient population in the real-world setting. This provided an alternative way of defining a comparator cohort and helped to assess the robustness of the findings from the landmark analysis. Additionally, the patients included in the study were required to have at least 5 years of available theoretical follow-up with an observed median follow-up of more than 6 years, which allowed for the reporting of long-term survival outcomes. Together, these methods strengthen the evidence of the impact that recurrence has on outcomes in this patient population.
Findings from this study show the importance of preventing and delaying recurrence in several ways. First, compared with patients who did not develop recurrence during follow-up, patients who had at least one recurrence event suffered a substantially lower 5-year survival rate (28.5 vs 58.1%). The study by Takenaka and colleagues, which included patients in Japan with and without adjuvant treatment post-resection, had a 5-year survival rate of 32%, which closely aligns with what was reported in our study [Citation17]. Second, recurrence was strongly associated with shorter OS from landmark points at 1, 3 and 5 years following complete resection (HR = 4.23 from 1 year, 4.63 from 3 years and 2.97 from 5 years; all p < 0.001). Cai and colleagues indicated that there was more than a threefold increase in death of patients with and without a relapse (62 vs 18%), though this is based on relapse over the total period of follow-up, rather than at pre-specified landmark timepoints [Citation10]. Our study used landmark timepoints to control for immortal time bias. Third, when we limited to patients with recurrence to understand the effect of timing of recurrence on post-recurrence survival, patients with recurrence within 1 year of complete resection had a numerically shorter post-recurrence survival compared with those who developed recurrence between 1 and 5 years after resection (24.1 vs 39.1 months; p = 0.132). These results are similar in range to those reported by Takenaka and colleagues, which showed that median post-recurrence survival was 30 months [Citation17].
Our study also illustrated the difference in HCRU between patients with and without recurrence. In the adjusted model, our study indicated that patients with recurrence have more than double the incidence rate of office visits and nearly four-times as high an incidence rate of hospitalizations, after adjusting for pertinent confounders. This finding suggests that early recurrence may function as a proxy indicator for aggressiveness of disease, in which more aggressive disease drives greater utilization as well as poorer clinical outcomes. This finding is in line with previous work that illustrated an increase in HCRU post-recurrence, versus prior to recurrence [Citation10]. However, this study adds to the earlier work in that our evaluation of HCRU was conducted in patients with and without recurrence, including patients whose recurrence may have been delayed or prevented altogether, whereas the prior study only evaluated patients with a recurrence.
Results from this study clearly provide valuable additional information regarding the outcomes of patients following complete resection in early-stage NSCLC. The study findings illustrate that the event of recurrence and the possibility of delaying or preventing recurrence have a pivotal impact on OS and total HCRU in these patients with stage IB to IIIA NSCLC. Our study also included patients with the specific stages of disease for which resection is indicated, and further limited the analyses to the sub-cohort of patients with complete resection to ensure a more defined patient population. In contrast, other previous studies employed staging inclusion criteria that extend outside the range of stages for which resection is the standard treatment modality, stage II–IIIB in the study by Cai and colleagues, and stage I–III in the study by Takenaka and colleagues [Citation10,Citation17]. Our study also evaluated the timing of recurrence among patients who had a recurrence. We compared the impact of recurrence among patients who experienced a recurrence within 1 year and between 1–5 years. This design employed RMST regression to quantify the impact of delayed recurrence on 5-year survival post-recurrence. The study by Takenaka and colleagues also examined the timing of recurrence; however, patients with recurrence between 1 and 5 years were aggregated with patients whose recurrence occurred more than 5 years after complete resection [Citation17]. This may have resulted in confounding of other longer-term covariates of survival with the timing of recurrence, an effect our approach was designed to avoid.
The findings from this real-world data study clearly illustrate the impact of recurrence on survival and HCRU in patients with completely resected early-stage NSCLC. Given the introduction of new agents that are improving outcomes in this population [Citation19,Citation20,Citation25], these data represent a valuable addition to the literature as a benchmark for expectations when calculating cost-benefit of treatments to maximize clinical outcomes in this setting.
This study has a number of strengths. These include a moderately large sample size drawn from a geographically diverse area in the USA; and study sampling was agnostic of registry participation, insurance program enrollment, or healthcare system membership. Results should therefore be reflective of outcomes in the real-world population. The study also included all eligible patients from stage IB to IIIA, with or without adjuvant treatments post-resection, and did not restrict inclusion based on risk categorization. Of note, patients diagnosed with NSCLC prior to 2010 were re-staged at data collection to align with American Joint Committee on Cancer 7th edition staging, the current edition at the time most patients were treated, to decrease the inconsistency between stage definitions over time. The study also employed data created through manual review of the entire medical record including pathology reports, progress notes, radiological scans, etc., which optimized both the accuracy and completeness of study data compared with methods that rely solely on structured data. Key variables related to case eligibility (diagnosis, staging, performance status, and complete resection) and other variables including recurrence, histology, and tumor response were manually curated to establish the greatest level of quality and completeness possible using retrospective real-world data. This allows for increased confidence in the study outcomes. Additionally, this study aimed to control for immortal time bias using landmark analysis, which we believe is a novel approach for addressing the impact of recurrence. The landmark analysis also examined end points from different landmark time points to assess whether results varied based on the selection of landmark. Finally, the study also included a minimum theoretical follow-up of 5 years after resection to more comprehensively assess long-term survival outcomes. These strengths make the study more generalizable and more useful for providers and payers in their decision-making process.
At the same time, it is important to acknowledge several limitations to this study. First, this study was retrospective, and findings should be interpreted in light of limitations associated with the retrospective design, such as the potential for missing data, and possible misclassification of patients. However, the study was conducted using data from both structured and unstructured sources, with manual review of EMR data by highly trained curators, and therefore the potential for biases was reduced. Next, patients in this study were mainly treated within community oncology practices in the USA, albeit from a large geographic range. However, findings from this study may not be as generalizable to the early-stage NSCLC population treated in academic settings or to patients treated outside of the USA Another limitation of the study was lack of incorporation of cost data into HCRU analysis; however, utilization was used as a proxy for cost. Additionally, the OS analyses conducted in this study did not control for all possible variables that may be associated with survival. An example is tumor size, which is related to high-risk status in stage IB and IIA patients, but which is generally not available in structured fields or unstructured documents. Finally, this study sought to evaluate long-term outcomes of treatment, and therefore required longer-term follow-up for inclusion. As a result, the study may therefore not generalize to the outcomes of recently approved therapies, including immunotherapy. It should be noted that the impact of avoiding recurrence or delaying recurrence was a key focus of the study and is also the main outcome associated with the emergence of these newer therapies in the early-stage setting.
Conclusion
Recurrence after complete resection is associated with worse survival outcomes and higher HCRU in patients with surgically resected stage IB-IIIA NSCLC, an effect that may be more pronounced in patients with recurrence within 1 year after resection. Results from this study highlight the potential value of preventing or delaying recurrence in this population. Further research is needed to evaluate survival outcomes, the relationship between disease-free survival and OS, and HCRU for patients receiving newer adjuvant therapies such as immuno-oncology agents and targeted therapies for early-stage NSCLC.
Previous research shows that up to 50% of patients with completely resected early-stage non-small-cell lung cancer (NSCLC) may still experience a recurrence, even with receipt of pre- and/or post-operative chemotherapy.
As new therapies are being introduced, research is needed to understand the timing and impact of recurrence in patients with early-stage NSCLC using real-world data.
Eligible patients were ≥18 years at initial NSCLC diagnosis, had a complete resection (documented residual tumor stage of R0 post-resection) prior to 1 March 2016 (to allow for a minimum 5 year follow-up), no prior neoadjuvant chemotherapy or radiotherapy, and no documentation of impaired performance status.
Patients were grouped into Recurrence and Non-Recurrence Cohorts. The Recurrence Cohort included patients with any recurrence event (locoregional recurrence or distant recurrence, based on provider documentation) or new diagnosis of another primary cancer other than non-melanoma skin cancer after complete resection; the Non-Recurrence Cohort included all other eligible patients.
Overall survival (OS) was evaluated from recurrence (or a matched index date), from three pre-specified landmark timepoints (1-, 3-, and 5-years post-resection) in Recurrence versus Non-Recurrence Cohorts, and in early versus late-recurring patients. Healthcare resource utilization (HCRU) was also compared among Recurrence versus Non-Recurrence Cohorts.
Recurrence was associated with a significantly shorter OS from date of recurrence (median OS 31.5 months) compared with OS from a matched index date in patients who did not experience a recurrence (median OS 75.6 months; HR = 2.47; p < 0.001).
Recurrence was strongly associated with shorter OS from landmark points at 1, 3, and 5 years following complete resection compared with patients who did not experience a recurrence (HR = 4.23 from 1 year, 4.63 from 3 years, and 2.97 from 5 years; all p < 0.001).
Patients with recurrence in 1–5 years tended to have longer restricted mean survival time through 5 years post-recurrence versus patients with recurrence within the first year (p = 0.069).
Patients with recurrence had higher HCRU compared with patients without a recurrence (follow-up office visits [IRR = 2.17] and hospitalizations [IRR = 3.76]; all p < 0.0001).
Patients in the Recurrence Cohort experienced worse survival outcomes compared with patients in the Non-Recurrence Cohort, even many years out from surgery. Patients who experienced a recurrence were also observed to have higher HCRU compared with those without a recurrence.
Author contributions
H West: Conceptualization, Methodology, Writing – Reviewing & Editing, Supervision. X Hu: Conceptualization, Methodology, Funding acquisition, Writing – Reviewing & Editing. D Chirovsky: Writing – Reviewing & Editing. MS Walker: Conceptualization, Methodology, Writing – Reviewing & Editing. Y Wang: Conceptualization, Methodology, Writing – Reviewing & Editing, Project administration. A Kaushiva: Writing – Original Draft, Writing – Reviewing & Editing, Project administration. J Tepsick: Writing – Original Draft, Writing – Reviewing & Editing. A Samkari: Writing – Reviewing & Editing.
Previous presentations
Part of this research was presented at the 2022 European Lung Cancer Congress (ELCC) (30 March–2 April 2022).
Financial & competing interests disclosure
H West reports financial relationships with Amgen, AstraZeneca, Eli Lilly, Genentech/Roche, Merck, Mirati Therapeutics, Pfizer, and Regeneron. X Hu, D Chirovsky, and A Samkari are employed by Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA and may hold stock or stock options in Merck & Co., Inc., Rahway, NJ, USA. MS Walker, Y Wang, A Kaushiva, and J Tepsick report research funding to their institution from Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA. Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA sponsored this study and provided financial support for the conduct of the research and preparation of the article. Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA (the sponsor) collaborated on the design of the study, interpretation of the analyses, and in the decision to submit the article for publication. The sponsor did not have a direct role in data collection, data analysis, or writing of the report. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
This retrospective chart review study involving human participants was in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. This research was reviewed and determined to be exempt from Institutional Review Board (IRB) oversight by Advarra IRB (Columbia, Maryland). This research study was conducted retrospectively from data obtained for clinical purposes.
Data sharing statement
ConcertAI does not make datasets publicly available because study data are used under license from source practices and other data providers. ConcertAI will consider requests to access study datasets on a case-by-case basis.
Supplementary Figure 1
Download PDF (563.1 KB)Supplementary Figure 2
Download PDF (440.5 KB)Supplementary Figure 3
Download PDF (418.5 KB)Acknowledgments
The authors would like to thank F Coutinho and L Lal (ConcertAI) for their contributions in reviewing and editing this manuscript as well as oversight of the project that is the basis of this manuscript. The authors would also like to thank R Parikh (consultant to ConcertAI) for his critical review and medical insights.
Supplementary data
To view the supplementary data that accompany this paper please visit the journal website at: www.futuremedicine.com/doi/suppl/10.2217/fon-2023-0024
Additional information
Funding
References
- Siegel RL , MillerKD, FuchsHE, JemalA. Cancer statistics, 2022. CA Cancer J. Clin.72(1), 7–33 (2022).
- Howlader N , ForjazG, MooradianMJet al. The effect of advances in lung-cancer treatment on population mortality. N. Engl. J. Med.383(7), 640–649 (2020).
- Cagle PT , AllenTC, OlsenRJ. Lung cancer biomarkers: present status and future developments. Arch. Pathol. Lab. Med.137(9), 1191–1198 (2013).
- Navani N , FisherDJ, TierneyJFet al. The accuracy of clinical staging of stage I–IIIa non-small-cell lung cancer: an analysis based on individual participant data. Chest155(3), 502–509 (2019).
- Burdett S , PignonJP, TierneyJet al. Adjuvant chemotherapy for resected early-stage non-small-cell lung cancer. Cochrane Database Syst. Rev. (3), DOI: 10.1002/14651858.CD011430 (2015).
- Chaft JE , RimnerA, WederW, AzzoliCG, KrisMG, CasconeT. Evolution of systemic therapy for stages I–III non-metastatic non-small-cell lung cancer. Nat. Rev. Clin. Oncol.18(9), 547–557 (2021).
- Edwards JG , ChanskyK, Van SchilPet al. The IASLC lung cancer staging project: analysis of resection margin status and proposals for residual tumor descriptors for non-small-cell lung cancer. J. Thorac. Oncol.15(3), 344–359 (2020).
- NSCLC Meta-Analysis Collaborative Group . Preoperative chemotherapy for non-small-cell lung cancer: a systematic review and meta-analysis of individual participant data. Lancet383(9928), 1561–1571 (2014).
- Boyd JA , HubbsJL, KimDW, HollisD, MarksLB, KelseyCR. Timing of local and distant failure in resected lung cancer: implications for reported rates of local failure. J. Thorac. Oncol.5(2), 211–214 (2010).
- Cai B , FulcherN, BoydM, SpiraA. Clinical outcomes and resource utilization after surgical resection with curative intent among patients with non-small-cell lung cancer treated with adjuvant therapies in a community oncology setting: a real-world retrospective observational study. Thorac. Cancer12(14), 2055–2064 (2021).
- National Cancer Institute. Surveillance, Epidemiology, and End Results Program . Cancer stat facts: lung and bronchus cancer. https://seer.cancer.gov/statfacts/html/lungb.html (Accessed 2August2022).
- Lopez Guerra JL , GomezDR, LinSHet al. Risk factors for local and regional recurrence in patients with resected N0-N1 non-small-cell lung cancer, with implications for patient selection for adjuvant radiation therapy. Ann. Oncol.24(1), 67–74 (2013).
- Ajmani GS , WangC-H, KimKW, HowingtonJA, KrantzSB. Surgical quality of wedge resection affects overall survival in patients with early stage non–small cell lung cancer. J. Thorac. Cardiovasc. Surg.156(1), 380–391.e2 (2018).
- Bugge AS , LundMB, ValbergM, BrustugunOT, SolbergS, KongerudJ. Cause-specific death after surgical resection for early-stage non-small-cell lung cancer. Eur. J. Cardiothorac. Surg.53(1), 221–227 (2018).
- Dziedzic R , ŻurekW, MarjańskiTet al. Stage I non-small-cell lung cancer: long-term results of lobectomy versus sublobar resection from the Polish National Lung Cancer Registry. Eur. J. Cardiothorac. Surg.52(2), 363–369 (2017).
- Garinet S , WangP, Mansuet-LupoA, FournelL, WislezM, BlonsH. Updated prognostic factors in localized NSCLC. Cancers (Basel)14(6), 1–20 (2022).
- Takenaka T , YanoT, YamazakiKet al. Survival after recurrence following surgical resected non-small-cell lung cancer: a multicenter, prospective cohort study. JTCVS Open10, 370–381 (2022).
- Andreas S , ChouaidC, DansonSet al. Economic burden of resected (stage IB-IIIA) non-small-cell lung cancer in France, Germany and the United Kingdom: a retrospective observational study (LuCaBIS). Lung Cancer124, 298–309 (2018).
- Wu YL , TsuboiM, HeJet al. Osimertinib in resected EGFR-mutated non-small-cell lung cancer. N. Engl. J. Med.383(18), 1711–1723 (2020).
- Felip E , AltorkiN, ZhouCet al. Adjuvant atezolizumab after adjuvant chemotherapy in resected stage IB-IIIA non-small-cell lung cancer (IMpower010): a randomised, multicentre, open-label, phase 3 trial. Lancet398(10308), 1344–1357 (2021).
- US Food and Drug Administration . FDA approves osimertinib as adjuvant therapy for non-small-cell lung cancer with EGFR mutations. https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-osimertinib-adjuvant-therapy-non-small-cell-lung-cancer-egfr-mutations (Accessed August 9, 2022).
- US Food and Drug Administration . FDA approves atezolizumab as adjuvant treatment for non-small-cell lung cancer. https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-atezolizumab-adjuvant-treatment-non-small-cell-lung-cancer (Accessed September 14, 2022).
- European Medicines Agency . Tagrisso (osimertinib). https://www.ema.europa.eu/en/medicines/human/EPAR/tagrisso (Accessed 9August2022).
- European Medicines Agency . Tecentriq (atezolizumab). https://www.ema.europa.eu/en/medicines/human/EPAR/tecentriq (Accessed 9August2022).
- O’Brien M , Paz-AresL, MarreaudSet al. Pembrolizumab versus placebo as adjuvant therapy for completely resected stage IB-IIIA non-small-cell lung cancer (PEARLS/KEYNOTE-091): an interim analysis of a randomised, triple-blind, phase 3 trial. Lancet Oncol.23(10), 1274–1286 (2022).