
Abstract
Poly(ADP-ribose) polymerase inhibitors in combination with androgen-receptor signaling inhibitors are a promising therapeutic option for patients with metastatic castration-sensitive prostate cancer (mCSPC) and homologous recombination repair (HRR) gene alterations. Here, we describe the design and rationale of the multinational, phase III, TALAPRO-3 study comparing talazoparib plus enzalutamide versus placebo plus enzalutamide in patients with mCSPC and HRR gene alterations. The primary end point is investigator-assessed radiographic progression-free survival (rPFS) per RECIST 1.1 in soft tissue, or per PCWG3 criteria in bone. The TALAPRO-3 study will demonstrate whether the addition of talazoparib can improve the efficacy of enzalutamide as assessed by rPFS in patients with mCSPC and HRR gene alterations undergoing androgen deprivation therapy.
Clinical Trial Registration: NCT04821622 (ClinicalTrials.gov)
Registry Name: Study of Talazoparib With Enzalutamide in Men With DDR Gene Mutated mCSPC.
Date of Registration: 29 March 2021.
Tweetable abstract
TALAPRO-3 is a phase III, randomized study that aims to evaluate the efficacy and safety of talazoparib plus enzalutamide versus placebo plus enzalutamide in men with metastatic castration-sensitive prostate cancer (mCSPC) and homologous recombination repair gene alterations.
Prostate cancer is the second leading cause of cancer-related death in men in the USA [Citation1]. Worldwide, an estimated 1,414,259 men were diagnosed with prostate cancer, and 375,304 men died from the disease in 2020 [Citation2]. Approximately 5–15% of patients are diagnosed with metastatic disease at the time of initial diagnosis of prostate cancer, and this can be up to 40% in some Asian countries. In the USA, the incidence of metastatic disease at diagnosis has been increasing in recent years. In addition, many patients who are initially diagnosed with localized disease will eventually progress to metastatic disease [Citation3–7]. While men with localized disease have a high 5-year survival rate of 99% if diagnosed at an early stage, men with metastatic disease have a poor survival of 30% at 5 years in the USA [Citation8].
Historically, metastatic castration-sensitive prostate cancer (mCSPC) was treated with androgen deprivation therapy (ADT) with either medical castration through administration of a gonadotropin-releasing hormone (GnRH) agonist or antagonist or surgical castration [Citation9,Citation10]. However, despite initial response, the vast majority of men receiving ADT therapy alone will progress to metastatic castration-resistant prostate cancer (mCRPC), within a median of 1–2 years [Citation11–14]. ADT in combination with docetaxel or an androgen-receptor signaling inhibitor (ARSI), such as enzalutamide, abiraterone acetate plus prednisone, and apalutamide, has become standard-of-care for men with mCSPC based on improvements in time-to-progression and overall survival (OS) compared with ADT alone [Citation12,Citation13,Citation15–18]. Combination therapy with ADT and an ARSI is not curative in nature and thus, many men with mCSPC will still experience disease progression to mCRPC in approximately 3 years [Citation13,Citation16], highlighting the necessity of developing novel therapeutic strategies that prolong the time-to-progression and improve OS.
Alterations in DNA damage response (DDR) genes (e.g., BRCA1/2, ATM, PALB2, CHEK2) of germline or somatic origin involved directly or indirectly in homologous recombination repair (hereafter referred to as HRR genes) have been found in 23–27% of metastatic prostate cancers [Citation19,Citation20], with some alterations (e.g., in BRCA2) associated with poor prognosis and rapid progression to mCRPC [Citation21–23]. Poly(ADP-ribose) polymerase 1 and 2 (PARP1/2) play essential roles in DNA repair by binding to single-strand breaks (SSB). When PARP1/2 are inhibited, SSBs can persist, resulting in stalled replication forks and conversion of SSBs into double-strand breaks (DSB), which in turn rely on the homologous recombination pathway for repair. Hence, alterations in HRR genes plus inhibition of PARP catalytic activity prevent DSBs from being repaired, causing cell death via synthetic lethality [Citation24,Citation25]. In preclinical models, HRR gene alterations, such as in BRCA1/2, have been shown to sensitize tumors to PARP inhibitors, such as talazoparib [Citation24,Citation26,Citation27].
Talazoparib is a potent PARP inhibitor that both inhibits PARP activity and traps PARP on SSBs, preventing DNA repair and leading to synthetic lethality in cancer cells () [Citation24,Citation28–30]. Talazoparib is currently approved for the treatment of adult patients with germline BRCA1/2-altered HER2-negative locally advanced or metastatic breast cancer [Citation31]. Talazoparib is also approved in the USA, in combination with enzalutamide, for the treatment of adult patients with HRR gene-mutated mCRPC following positive results from the phase III TALAPRO-2 study which evaluated the combination as first-line therapy in patients with mCRPC with and without alterations in HRR genes [Citation31,Citation32]. In addition, TALAPRO-1, a phase II study of talazoparib monotherapy, demonstrated robust antitumor activity in heavily pretreated men with mCRPC and HRR gene alterations [Citation33].
(A) Dual cytotoxic mechanisms of PARP inhibitors; (B) PARP inhibitor in combination with an ARSI.
Adapted with permission from Future Oncology [Citation29]. Reprinted (or adapted) from Cancer Research [Citation30].
AR: Androgen receptor; ARSI: Androgen-receptor signaling inhibitor; DDR: DNA damage response; DSB: Double-strand break; HRD: Homologous recombination deficiency; PARP: Poly(ADP-ribose) polymerase; PARPi: Poly(ADP-ribose) polymerase inhibitor; SSB: Single-strand break.
![Figure 1. Mechanistic overview of PARP inhibition. (A) Dual cytotoxic mechanisms of PARP inhibitors; (B) PARP inhibitor in combination with an ARSI.Adapted with permission from Future Oncology [Citation29]. Reprinted (or adapted) from Cancer Research [Citation30].AR: Androgen receptor; ARSI: Androgen-receptor signaling inhibitor; DDR: DNA damage response; DSB: Double-strand break; HRD: Homologous recombination deficiency; PARP: Poly(ADP-ribose) polymerase; PARPi: Poly(ADP-ribose) polymerase inhibitor; SSB: Single-strand break.](/cms/asset/5163bfeb-3e58-447e-8e10-90bbdbbdca5f/ifon_a_12367119_f0001.jpg)
Despite prior ADT treatment, androgen receptor (AR) signaling continues to be active, and so further inhibition of AR signaling pathway has also been used [Citation34]. Indeed, agents that target the AR signaling pathway, such as the ARSI enzalutamide, apalutamide, and darolutamide, and the androgen biosynthesis inhibitor abiraterone acetate, have significantly improved clinical outcomes for patients with mCSPC by slowing progression to mCRPC [Citation16,Citation35–38]. Interestingly, non-clinical models show that PARP1 activity is required for AR function; therefore, PARP inhibition may sensitize prostate cancer cells to AR-directed therapies [Citation39]. In addition, AR blockade downregulates HRR gene expression, which may induce a ‘BRCAness’ phenotype and increase sensitivity to PARP inhibitors [Citation40–42]. A non-clinical study has also showed that clinical resistance to AR blockade is sometimes associated with the deletion of BRCA2, which also confers sensitivity to PARP inhibitors [Citation43]. Therefore, there is potential for co-operative interactions between PARP inhibitors, such as talazoparib, and the AR inhibitor enzalutamide, which is an approved treatment in mCSPC [Citation44].
TALAPRO-3 study
Study design
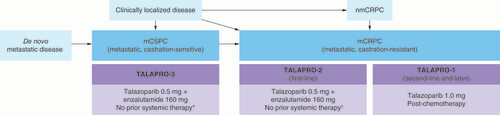
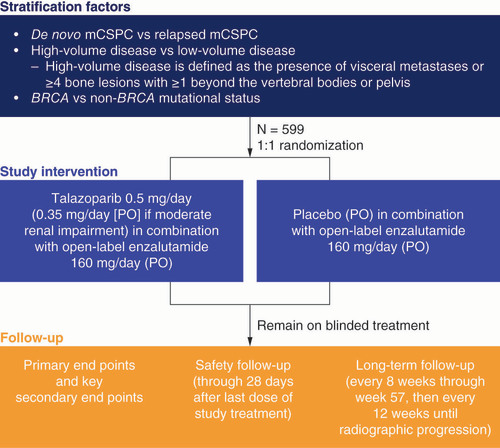
TALAPRO-3 (NCT04821622) is a phase III, multinational, double-blind, randomized study that aims to evaluate the efficacy and safety of talazoparib plus enzalutamide versus placebo plus enzalutamide in men with mCSPC and HRR gene alterations ( & ). The protocol and any protocol amendments will be reviewed and approved by the institutional review board (IRB)/ethics committee (EC) before the study or amend is initiated. Written summaries of the study status will be provided by the investigator to the IRB/EC annually.
*No prior life-prolonging systemic therapy for castration-sensitive prostate cancer, excluding ≤3 months androgen deprivation therapy with or without an approved androgen-receptor signaling inhibitor; treatment with estrogens, cyproterone acetate, or first-generation anti-androgens is allowed until randomization.
†No prior life-prolonging systemic therapy for castration-resistant prostate cancer, excluding androgen deprivation therapy and first-generation antiandrogens.
mCRPC: Metastatic castration-resistant prostate cancer; mCSPC: Metastatic castration-sensitive prostate cancer; nmCRPC: Non-metastatic castration-resistant prostate cancer.
mCSPC: Metastatic castration-sensitive prostate cancer; PO: Per oral.
Genomic screening will be performed during the prescreening period using a peripheral blood sample and/or tumor tissue if available (only tumor tissue in China) to identify alterations in HRR genes. The FoundationOne Liquid CDx test that includes a HRR12 gene panel (ATM, ATR, BRCA1, BRCA2, CDK12, CHEK2, FANCA, MLH1, MRE11A, NBN, PALB2, RAD51C) will be used to determine the presence of HRR gene alterations. Upon sponsor pre-approval, historical FoundationOne Liquid CDx results may be considered as an alternative to a blood sample, or prior testing results of tumor tissue using FoundationOne CDx may be used for eligibility in case FoundationOne Liquid fails or is negative.
Eligible patients will be randomized (1:1) to talazoparib (0.5 mg/day) in combination with enzalutamide (160 mg/day) or placebo in combination with enzalutamide (160 mg/day). Patients will be stratified according to de novo mCSPC versus relapsed mCSPC; high-volume disease, defined as the presence of visceral metastases or ≥4 bone lesions with ≥1 beyond the vertebral bodies or pelvis, versus low-volume disease and BRCA versus non-BRCA mutational status. Talazoparib and placebo will be blinded, while enzalutamide will be open label. For patients with moderate renal impairment (estimated glomerular filtration rate 30–59 ml/min/1.73 m2), the dose of talazoparib will be 0.35 mg/day to account for lower clearance in this subpopulation. All patients will receive treatment until radiographic progression determined by the investigator, unacceptable toxicity, or an adverse event (AE) leading to permanent discontinuation, withdrawal of consent, patient decision to discontinue, or death.
The safety follow-up visit will occur approximately 28 days after permanent study intervention, discontinuation or before initiation of a new antineoplastic or investigational therapy, whichever occurs first. Long-term follow-up will begin after safety follow-up.
Enrollment
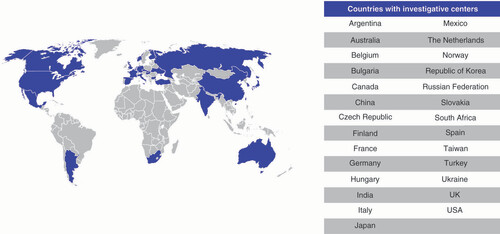
Enrollment for TALAPRO-3 began in May 2021 and the last patient was dosed in May 2023. The final number of randomized patients is 599. All patients with mCSPC harboring HRR gene alterations were enrolled and randomized 1:1 to each treatment arm. Patients were recruited across 27 countries, including the USA, Canada, South Africa and Australia, and in European, South American and Asia-Pacific countries ().
Key eligibility criteria
To be eligible to participate in the TALAPRO-3 study, patients must be male and aged ≥18 years (≥20 years in Japan; ≥19 years in the Republic of Korea) with a histologically/cytologically confirmed adenocarcinoma of the prostate without neuroendocrine differentiation, small cell, or signet cell features and with alterations in one or more HRR genes (as per HRR12 gene panel).
Eligible patients may have received ≤3 months of ADT (chemical or surgical) with or without an approved ARSI in the mCSPC setting. However, prior treatment of mCSPC with docetaxel is exclusionary due to the lack of consensus or guidelines that outlined the sequence of therapy for mCSPC at the time of the study design and the potential safety concerns due to the overlapping toxicities of talazoparib and docetaxel. In addition, patients who have not undergone bilateral orchiectomy must be receiving ongoing ADT with a GnRH agonist or antagonist, which should continue throughout the study. Patients must have metastatic disease documented by a positive bone scan for bone disease or on a CT or MRI scan for soft tissue disease. Other key inclusion criteria are listed in .
Table 1. Key inclusion and exclusion criteria of the TALAPRO-3 study.
Patients are not eligible to take part in the study if they have a history of seizures or any conditions that may predispose to a seizure, including any history of loss of consciousness or transient ischemic attack within 12 months of randomization, or known or suspected brain metastases, or active leptomeningeal disease.
Patients are also excluded if they have any history of myelodysplastic syndrome, acute myeloid leukemia, or prior malignancy except for the following: carcinoma in situ or non-melanoma skin cancer; a cancer diagnosed and treated ≥3 years before randomization with no subsequent evidence of recurrence; or a Stage 0 or Stage 1 (by American Joint Committee on Cancer) cancer <3 years before randomization that has a remote probability of recurrence in the opinion of the investigator and the sponsor. Patients with prior treatment in any setting with any ARSI, except as described in the inclusion criteria above and patients with active COVID-19 infection detected by approved tests or by clinical diagnosis are not eligible. Other key exclusion criteria are listed in .
Study end points & evaluations
In the TALAPRO-3 study, the primary end point is investigator-assessed radiographic progression-free survival (rPFS), defined as the time from the date of randomization to radiographic progression in soft tissue per Response Evaluation Criteria in Solid Tumors version 1.1 (RECIST 1.1), or in bone per Prostate Cancer Working Group 3 (PCWG3) criteria by the investigator, or death, whichever occurs first.
The key secondary end point is OS, defined as the time from randomization to the date of death due to any cause. Other secondary end points include objective response rate (ORR), defined as the proportion of patients with measurable soft-tissue disease at baseline who have confirmed objective response of complete response (CR) or partial response (PR) per RECIST 1.1; duration of soft tissue response, defined as the time from first objective evidence of a CR or PR to the first objective evidence of disease progression in soft tissue per RECIST 1.1 or in bone per PCWG3, or death, whichever occurs first; the proportion of patients with confirmed prostate-specific antigen (PSA) response ≥50%, and time to confirmed PSA progression, defined as a ≥25% increase in PSA with an absolute increase of ≥2 ng/ml above the nadir (or baseline for patients with no PSA decline), confirmed by a second consecutive PSA value at ≥21 days later.
Additional secondary and exploratory end points include time to initiation of antineoplastic therapy and time to progression on subsequent antineoplastic therapy, defined as the time from randomization to the start of second subsequent antineoplastic therapy after disease progression, or death from any cause, whichever occurs first; time to first symptomatic skeletal event; time to opioid use for prostate cancer pain; circulating tumor DNA burden (fraction) at baseline and on study per FoundationOne Liquid or another suitable validated assay; safety; pharmacokinetics (PK); biomarkers and patient-reported outcomes (PRO). Study end points are listed in .
Table 2. TALAPRO-3 study end points.
Efficacy analyses will be performed every 8 weeks through week 57, and every 12 weeks thereafter in all randomized patients using the tumor assessments by the investigator as the primary data source. A sample-based blinded independent central review approach will be implemented as an auditing tool for rPFS. Soft-tissue responses must be confirmed by a follow-up radiographic assessment ≥4 weeks later with no evidence of concurrent confirmed bone disease progression on repeated bone scans ≥6 weeks apart per PCWG3 criteria. The primary evaluation of ORR will be based on investigator assessment using derived response per RECIST 1.1.
Compliance with the study intervention will be assessed and documented by counting the number of returned capsules during each site visit. Patients will be considered non-compliant if ≥20% of monthly doses are missed.
Safety will be evaluated in all randomized patients who receive ≥1 dose of study intervention using AE, laboratory, and vital signs data. Treatment-emergent safety data will be defined as events from the first dose of study intervention through approximately 28 days after the last dose, or upon initiation of a new antineoplastic therapy, whichever occurs first. Incidence of AEs will be presented by type with and without regard to causality per investigator judgment and by frequency of overall toxicity graded by National Cancer Institute Common Terminology Criteria AE version 4.03.
PK data analyses will be conducted in patients who receive ≥1 dose of talazoparib or enzalutamide with an evaluable PK sample. Analyses will include descriptive summary statistics of the predose plasma concentrations of talazoparib, enzalutamide, and its N-desmethyl metabolite by study visit and treatment arm.
PROs will be evaluated as between-arm change from baseline and time to deterioration analyses. PROs will be assessed using the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire (Core 30; EORTC QLQ C30) and its QLQ-PR25 prostate cancer module, Brief Pain Inventory-Short Form (BPI-SF), European Quality of Life 5 Dimension, 5 Level Scale (EQ-5D-5L) and patient global impression of severity (PGI-S) at day 1 (baseline), every 4 weeks through week 25, every 8 weeks until week 57 and then every 12 weeks until treatment is discontinued.
The EORTC QLQ-C30 comprises five multi-item functional subscales, three multi-item symptom scales, a global health score/quality-of-life subscale, and six single-item symptom scales assessing other disease and/or treatment-related symptoms. The EORTC QLQ-PR25 comprises two multi-item functional scales (sexual activity and sexual functioning) and four single-item symptom scales (urinary symptoms, bowel symptoms, hormonal treatment-related symptoms and incontinence aid).
Pain will be assessed using the BPI-SF questionnaire, a validated nine-item instrument that uses a self-reported scale to assess level of pain, its effect on activities of daily living and analgesic medication use.
The EQ-5D-5L is a validated and standardized instrument that measures the general health status of participants. Patients will self-rate their current state of mobility, self-care, usual activities, pain/discomfort and anxiety/depression by choosing one of five possible responses that record the level of severity (no problems, slight problems, moderate problems, severe problems, or extreme problems) within each dimension. The questionnaire also includes a visual analog scale to self-rate general health state on a scale from ‘the worst health you can imagine’ to ‘the best health you can imagine’.
The PGI-S scale is a validated, generic, one-item questionnaire using balanced Likert scales that asks patients to rate the severity of their illness. The PGI-S can be used as an anchoring method to determine the minimal clinically significant difference for other PROs. Patients will rate the severity of their illness over the past 4 weeks on a five-point scale where 1 is ‘None’ and 5 is ‘Very severe’.
Biomarkers will be assessed separately for blood, circulating tumor cells, tumor tissue, and saliva collected during the study.
Statistical analysis
Time-to-event distributions will be estimated using Kaplan–Meier curves, and hazard ratios and associated 95% CI will be estimated using a Cox proportional hazard model. To control the overall type I error rate for the study, a hierarchical testing approach will be used, whereby rPFS will be formally tested first. If it is significant, then OS will be tested at an overall two-sided 5% level of significance.
For all PROs, longitudinal mixed-effects analysis will be used to estimate the overall between arm differences in change from baseline scores. Time to deterioration analyses will be evaluated via the Kaplan–Meier method.
Stratified analysis of key efficacy end points including rPFS and OS will be conducted, in addition to post hoc subgroup analyses of the BRCA and non-BRCA groups.
Discussion & future perspective
The clinical benefit of PARP inhibitors in patients with metastatic prostate cancer and HRR gene alterations has been established. Olaparib improved OS and was approved in the USA for the treatment of patients with mCRPC and HRR gene alterations following treatment with enzalutamide or abiraterone [Citation45,Citation46], and in Europe as a monotherapy for the treatment of adult patients with mCRPC and BRCA1/2 mutations who have progressed following prior therapy that included a new hormonal agent [Citation47]. Rucaparib also demonstrated antitumor efficacy and received accelerated approval from the US FDA for men with BRCA-mutated mCRPC [Citation48,Citation49]. Non-clinical studies showed enhanced activity of PARP inhibitors in combination with an ARSI, such as enzalutamide or abiraterone, relative to the respective single agents, thus providing a rationale for clinical studies focusing on combination therapy as first-line treatment options for patients with mCRPC [Citation39,Citation50,Citation51]. In addition, a phase III trial (NCT03748641) assessing niraparib in combination with abiraterone acetate and prednisone showed improved clinical outcomes in patients with HRR gene alterations [Citation52]; another phase III trial (NCT03732820) also demonstrated the benefit of olaparib in combination with abiraterone in patients with newly diagnosed mCRPC, regardless of HRR status [Citation53]. The TALAPRO-2 (NCT03395197) study is ongoing and OS data from patients with and without HRR gene alterations is awaited [Citation54].
PARP inhibitors are also entering the arena, alone or in combination with an ARSI, in the mCSPC setting. In addition to the TALAPRO-3 study described in this paper, another ongoing phase III trial is evaluating niraparib in combination with abiraterone acetate and prednisone in mCSPC in patients with HRR-mutated disease (NCT04497844). Other PARP inhibitors, including olaparib (NCT05167175) and rucaparib (NCT03413995), are also under investigation in single-arm phase II studies, in combination with abiraterone acetate and prednisone, or alone, in patients with mCSPC and DDR alterations. These trials, inclusive of TALAPRO-3, collectively may lead to a transformation in clinical practice with incorporation of PARP inhibitors in the treatment paradigm for mCSPC patients harboring HRR gene alterations.
Conclusion
The TALAPRO-3 study will be conducted to demonstrate whether talazoparib in combination with enzalutamide can improve efficacy in terms of rPFS versus placebo plus enzalutamide in men with mCSPC and HRR gene alterations undergoing ADT.
Background
Despite the combination of androgen deprivation therapy (ADT) with an androgen-receptor signaling inhibitor (ARSI) becoming standard-of-care for patients with metastatic castration-sensitive prostate cancer (mCSPC), many patients will still progress to metastatic castration-resistant prostate cancer (mCRPC) in ∼3 years, highlighting the need for novel therapeutic strategies.
Poly(ADP-ribose) polymerase (PARP) inhibitors in combination with an ARSI have shown clinical benefits in the treatment of mCRPC.
Talazoparib in combination with enzalutamide has recently been approved in the USA for the treatment of adult patients with HRR gene-mutated mCRPC.
Homologous recombination repair (HRR) alterations in mCSPC are associated with shorter progression to mCRPC and have also been shown to sensitize tumors to PARP inhibitors, suggesting the potential use of PARP inhibitors in patients with mCSPC and HRR alterations.
Talazoparib is a potent PARP inhibitor that has demonstrated robust antitumor activity in men with mCRPC with HRR gene alterations who received prior life-prolonging therapy for castration resistant disease.
TALAPRO-3 study design & key eligibility criteria
TALAPRO-3 is a phase III, multinational, double-blind, randomized study that aims to evaluate the efficacy and safety of talazoparib plus enzalutamide versus placebo plus enzalutamide in men with mCSPC and HRR gene alterations.
The study will compare the efficacy and safety of talazoparib (0.5 mg/day) plus enzalutamide (160 mg/day) to placebo plus enzalutamide (160 mg/day).
Patients are stratified by the following factors: de novo mCSPC versus relapsed mCSPC; high-volume disease versus low-volume disease and BRCA versus non-BRCA mutational status.
599 patients were enrolled in 27 countries, including the USA, Canada, South Africa and Australia, and in European, South American and Asia-Pacific countries.
End points & evaluations
The primary end point is investigator-assessed radiographic progression-free survival, defined as the time from the date of randomization to radiographic progression in soft tissue per RECIST 1.1, or in bone per PCWG3 criteria, or death, whichever occurs first.
Key secondary end points include overall survival, objective response rate, duration of soft-tissue response, proportion of patients with prostate-specific antigen response ≥50%, circulating tumor DNA burden, safety and patient-reported outcomes.
Conclusion
The TALAPRO-3 study will demonstrate whether talazoparib in combination with enzalutamide can improve the efficacy of enzalutamide in terms of radiographic progression-free survival in men with mCSPC and HRR gene alterations undergoing ADT.
Author contributions
Contributed to study conception or design: N Agarwal, F Saad, A Azad, J Chakrabarti, H-C Chen, S Lanzalone, A Niyazov and K Fizazi. Contribution to acquisition, analysis, or interpretation of data: All authors. Drafting of the manuscript or revising it critically for important intellectual content: all authors. Final approval of the version to be published: all authors. Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved: all authors.
Acknowledgments
The authors thank the patients and their families and caregivers for their participation, as well as the trial centers who supported this study.
Financial disclosure
This study was sponsored by Pfizer. Astellas Pharma Inc. provided enzalutamide. N Agarwal reports no personal COIs since 15 April 2021; consultancy roles with Astellas Pharma, AstraZeneca, AVEO, Bayer, Bristol Myers Squibb, Calithera Biosciences, Clovis, Eisai, Eli Lilly, EMD Serono, Exelixis, Foundation Medicine, Genentech, Gilead, Janssen Oncology, Merck, MEI Pharma, Nektar, Novartis, Pfizer, Pharmacyclics, and Seattle Genetics; and research funding to his institution from Arnivas, Astellas, AstraZeneca, Bavarian Nordic, Bayer, Bristol Myers Squibb, Calithera Biosciences, Celldex, Clovis, Crispr, Eisai, Eli Lilly, EMD Serono, Exelixis, Genentech, Gilead, GlaxoSmithKline, Immunomedics, Janssen, Lava, Medivation, Merck, Nektar, Neoleukin, NewLink Genetics, Novartis, Oric, Pfizer, Prometheus, Rexahn Pharmaceuticals, Roche, Sanofi, Seattle Genetics, Takeda, and TRACON Pharma. F Saad reports consulting fees from AAA/Novartis, Astellas Pharma, AstraZeneca/MedImmune, Bayer, Janssen Oncology, Merck, Myovant, Pfizer, Sanofi and Tolmar; funding for research work to his institution from AAA/Novartis, Astellas Pharma, AstraZeneca, Bayer, Bristol Myers Squibb, Janssen, Merck, Myovant, Pfizer, and Sanofi; and honoraria from AAA/Novartis, AbbVie, Amgen, Astellas Pharma, AstraZeneca, Bayer, Janssen Oncology, Merck, Myovant, Pfizer and Sanofi. AA Azad reports honoraria from Aculeus Therapeutics, Amgen, Astellas Pharma, AstraZeneca, Bayer, Bristol Myers Squibb, Ipsen, Janssen, Merck Serono, Merck Sharp & Dohme, Novartis, Noxopharm, Pfizer, Sanofi, Telix, and Tolmar; a consulting or advisory role for Aculeus Therapeutics, Amgen, Astellas Pharma, AstraZeneca, Bayer, Bristol Myers Squibb, Ipsen, Janssen, Merck Serono, Merck Sharp & Dohme, Novartis, Noxopharm, Pfizer, Sanofi, Telix, and Tolmar; speakers’ bureau for Amgen, Astellas Pharma, Bayer, Bristol Myers Squibb, Ipsen, Janssen, Merck Serono, and Novartis; research funding from Aptevo Therapeutics (institutional), Astellas Pharma (institutional), Astellas Pharma (investigator), AstraZeneca (institutional), AstraZeneca (investigator), Bionomics (institutional), Bristol Myers Squibb (institutional), Eli Lilly (institutional), Exelixis (institutional), Gilead Sciences (institutional), GlaxoSmithKline (institutional), Hinova (institutional), Ipsen (institutional), Janssen (institutional), MedImmune (institutional), Merck Serono (investigator), Merck Serono (institutional), Merck Sharpe & Dohme (institutional), Novartis (institutional), Pfizer (institutional), Sanofi Aventis (institutional), and Synthorx (institutional); and travel, accommodation, and expenses from Amgen, Astellas Pharma, Janssen, Merck Serono, Novartis, Pfizer and Tolmar. J Mateo reports participation in advisory boards for Amgen, AstraZeneca, Clovis Oncology, Janssen, Merck/Merck Sharp & Dohme, and Roche; participation in speakers’ bureau for Astellas Pharma, AstraZeneca, Guardant Health, Janssen, Merck Sharp & Dohme, and Pfizer; and has received research funding from AstraZeneca and Pfizer Oncology through grants to the institution. N Matsubara reports honoraria from AstraZeneca, Bayer, Chugai Pharma (institutional), Janssen and Merck Sharp & Dohme; a consulting or advisory role for AstraZeneca, Janssen, Lilly and Sanofi; and research funding to his institution from Astellas Pharma, AstraZeneca, Bayer, Bayer Yakuhin, Chugai Pharma, Janssen and Merck Sharp & Dohme. ND Shore is the Director of Carolina Urologic Research Center, has received payment from Ferring for expert testimony, and has served as a consultant or advisory board member for AbbVie, Amgen, Asieris, Astellas, AstraZeneca, Bayer, Bristol Myers Squibb, Boston Scientific, Clarity, Clovis Oncology, Cold Genesys, Dendreon, Exact Imaging, Exact Sciences, FerGene, Foundation Medicine, GenesisCare, Invitae, Janssen, Lantheus, Lilly, MDxHealth, Merck, Myovant, Myriad, Nymox, Pacific Edge, Pfizer, Phosphorous, Photocure, PreView, Propella, Sanofi Genzyme, Sema4, Sesen Bio, Specialty Networks, Telix, Tempus, Tolmar, UroGen and Vaxiion. J Chakrabarti, H-C Chen, S Lanzalone and A Niyazov are employees of Pfizer and hold Pfizer stock/stock options. K Fizazi reports consulting fees from Astellas Pharma, Bayer, Clovis, CureVac, ESSA, Janssen Oncology, Orion Pharma GmbH, and Sanofi; honoraria from Astellas Pharma, Bayer, Janssen, and Sanofi; and travel, accommodation, and expenses from Amgen, Janssen, and Merck Sharp & Dohme. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Competing interests disclosure
The authors have no competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending or royalties.
Writing disclosure
Medical writing support, under the direction of the authors, was provided by M Higgins and N Yang of CMC Affinity, a division of IPG Health Medical Communications, in accordance with Good Publication Practice (GPP 2022) guidelines. This assistance was funded by Pfizer.
Ethical conduct of research
The study is being conducted in accordance with the protocol (Final Protocol Amendment 1), legal and regulatory requirements, and the general principles set forth in the International Ethical Guidelines for Biomedical Research Involving Human Subjects (Council for International Organizations of Medical Sciences 2002), ICH Guideline for Good Clinical Practice, and the Declaration of Helsinki. Additionally, informed consent has been obtained from the participants involved.
Open access
This work is licensed under the Attribution-NonCommercial-NoDerivatives 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
Supplementary Data 1
Download PDF (358.8 KB)Supplementary data
An infographic accompanies this paper. To view or download this infographic in your browser please click here: https://www.tandfonline.com/doi/suppl/10.2217/fon-2023-0526
Data sharing statement
Upon request, and subject to review, Pfizer will provide the data that support the findings of this study. Subject to certain criteria, conditions and exceptions, Pfizer may also provide access to the related individual de-identified participant data. See www.pfizer.com/science/clinical-trials/trial-data-and-results for more information.
References
- Key Statistics for Prostate Cancer. www.cancer.org/cancer/prostate-cancer/about/key-statistics.html (12 September 2022).
- Prostate Cancer Statistics. www.wcrf.org/cancer-trends/prostate-cancer-statistics/ (21 September 2022).
- Siegel DA, O’Neil ME, Richards TB, Dowling NF, Weir HK. Prostate cancer incidence and survival, by stage and race/ethnicity - United States, 2001-2017. MMWR Morb. Mortal. Wkly Rep. 69(41), 1473–1480 (2020).
- Pinsky PF, Black A, Daugherty SE et al. Metastatic prostate cancer at diagnosis and through progression in the Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial. Cancer 125(17), 2965–2974 (2019).
- Greenberg DC, Wright KA, Lophathanon A, Muir KR, Gnanapragasam VJ. Changing presentation of prostate cancer in a UK population--10 year trends in prostate cancer risk profiles in the East of England. Br. J. Cancer 109(8), 2115–2120 (2013).
- Thurin NH, Rouyer M, Gross-Goupil M et al. Epidemiology of metastatic castration-resistant prostate cancer: a first estimate of incidence and prevalence using the French nationwide healthcare database. Cancer Epidemiol. 69, DOI:10.1016/j.canep.2020.101833 (2020).
- Chen R, Ren S, Yiu MK et al. Prostate cancer in Asia: a collaborative report. Asian J. Urol. 1(1), 15–29 (2014).
- Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2021. CA Cancer J. Clin. 71(1), 7–33 (2021).
- Harada K, Shiota M, Minato A et al. Treatment strategies for metastatic castration-sensitive prostate cancer: from “all-comers” to “personalized” approach. Onco. Targets Ther. 14, 2967–2974 (2021).
- Blas L, Shiota M, Eto M. Current status and future perspective on the management of metastatic castration-sensitive prostate cancer. Cancer Treat. Res. Commun. 32, DOI:10.1016/j.ctarc.2022.100606 (2022).
- Freedland SJ, Sandin R, Sah J et al. Treatment patterns and survival in metastatic castration-sensitive prostate cancer in the US Veterans Health Administration. Cancer Med. 10(23), 8570–8580 (2021).
- Kyriakopoulos CE, Chen YH, Carducci MA et al. Chemohormonal therapy in metastatic hormone-sensitive prostate cancer: long-term survival analysis of the randomized Phase III E3805 CHAARTED trial. J. Clin. Oncol. 36(11), 1080–1087 (2018).
- Armstrong AJ, Azad AA, Iguchi T et al. Improved survival with enzalutamide in patients with metastatic hormone-sensitive prostate cancer. J. Clin. Oncol. 40(15), 1616–1622 (2022).
- Chi KN, Chowdhury S, Bjartell A et al. Apalutamide in patients with metastatic castration-sensitive prostate cancer: final survival analysis of the randomized, double-blind, Phase III TITAN study. J. Clin. Oncol. 39(20), 2294–2303 (2021).
- Fizazi K, Tran N, Fein L et al. Abiraterone acetate plus prednisone in patients with newly diagnosed high-risk metastatic castration-sensitive prostate cancer (LATITUDE): final overall survival analysis of a randomised, double-blind, phase 3 trial. Lancet Oncol. 20(5), 686–700 (2019).
- Chi KN, Agarwal N, Bjartell A et al. Apalutamide for metastatic, castration-sensitive prostate cancer. N. Engl. J. Med. 381(1), 13–24 (2019).
- Hahn AW, Higano CS, Taplin M-E, Ryan CJ, Agarwal N. Metastatic castration-sensitive prostate cancer: optimizing patient selection and treatment. Am. Soc. Clin. Oncol. Educ. Book. 38, 363–371 (2018).
- Parker C, Castro E, Fizazi K et al. Prostate cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 31(9), 1119–1134 (2020).
- Chung JH, Dewal N, Sokol E et al. Prospective comprehensive genomic profiling of primary and metastatic prostate tumors. JCO Precis. Oncol. 3, DOI:10.1200/PO.18.00283 (2019).
- Armenia J, Wankowicz SAM, Liu D et al. The long tail of oncogenic drivers in prostate cancer. Nat. Genet. 50(5), 645–651 (2018).
- Castro E, Romero-Laorden N, Del Pozo A et al. PROREPAIR-B: a prospective cohort study of the impact of germline DNA repair mutations on the outcomes of patients with metastatic castration-resistant prostate cancer. J. Clin. Oncol. 37(6), 490–503 (2019).
- Annala M, Vandekerkhove G, Khalaf D et al. Circulating tumor DNA genomics correlate with resistance to abiraterone and enzalutamide in prostate cancer. Cancer Discov. 8(4), 444–457 (2018).
- Vandekerkhove G, Struss WJ, Annala M et al. Circulating tumor DNA abundance and potential utility in de novo metastatic prostate cancer. Eur. Urol. 75(4), 667–675 (2019).
- Lord CJ, Ashworth A. PARP inhibitors: synthetic lethality in the clinic. Science 355(6330), 1152–1158 (2017).
- Turk AA, Wisinski KB. PARP inhibitors in breast cancer: bringing synthetic lethality to the bedside. Cancer 124(12), 2498–2506 (2018).
- Bryant HE, Schultz N, Thomas HD et al. Specific killing of BRCA2-deficient tumours with inhibitors of poly(ADP-ribose) polymerase. Nature 434(7035), 913–917 (2005).
- Shen Y, Rehman FL, Feng Y et al. BMN 673, a novel and highly potent PARP1/2 inhibitor for the treatment of human cancers with DNA repair deficiency. Clin. Cancer Res. 19(18), 5003–5015 (2013).
- Murai J, Huang SY, Renaud A et al. Stereospecific PARP trapping by BMN 673 and comparison with olaparib and rucaparib. Mol. Cancer Ther. 13(2), 433–443 (2014).
- Agarwal N, Azad A, Shore ND et al. Talazoparib plus enzalutamide in metastatic castration-resistant prostate cancer: TALAPRO-2 Phase III study design. Future Oncol. 18(4), 425–436 (2022).
- Murai J, Huang SN, Das BB et al. Trapping of PARP1 and PARP2 by clinical PARP inhibitors. Cancer Res. 72(21), 5588–5599 (2012).
- U.S. Food and Drug Administration. TALZENNA® (talazoparib) prescribing information. (June 2023).
- Agarwal N, Azad AA, Carles J et al. Talazoparib plus enzalutamide in men with first-line metastatic castration-resistant prostate cancer (TALAPRO-2): a randomised, placebo-controlled, phase 3 trial. Lancet 402, 291–303 (2023).
- de Bono JS, Mehra N, Scagliotti GV et al. Talazoparib monotherapy in metastatic castration-resistant prostate cancer with DNA repair alterations (TALAPRO-1): an open-label, phase 2 trial. Lancet Oncol. 22(9), 1250–1264 (2021).
- Feng Q, He B. Androgen receptor signaling in the development of castration-resistant prostate cancer. Front. Oncol. 9, 858 (2019).
- Armstrong AJ, Szmulewitz RZ, Petrylak DP et al. ARCHES: a randomized, Phase III study of androgen deprivation therapy with enzalutamide or placebo in men with metastatic hormone-sensitive prostate cancer. J. Clin. Oncol. 37(32), 2974–2986 (2019).
- Smith MR, Hussain M, Saad F et al. Darolutamide and survival in metastatic, hormone-sensitive prostate cancer. N. Engl. J. Med. 386(12), 1132–1142 (2022).
- Fizazi K, Tran N, Fein L et al. Abiraterone plus prednisone in metastatic, castration-sensitive prostate cancer. N. Engl. J. Med. 377(4), 352–360 (2017).
- James ND, de Bono JS, Spears MR et al. Abiraterone for prostate cancer not previously treated with hormone therapy. N. Engl. J. Med. 377(4), 338–351 (2017).
- Schiewer MJ, Goodwin JF, Han S et al. Dual roles of PARP-1 promote cancer growth and progression. Cancer Discov. 2(12), 1134–1149 (2012).
- Polkinghorn WR, Parker JS, Lee MX et al. Androgen receptor signaling regulates DNA repair in prostate cancers. Cancer Discov. 3(11), 1245–1253 (2013).
- Li L, Karanika S, Yang G et al. Androgen receptor inhibitor–induced “BRCAness” and PARP inhibition are synthetically lethal for castration-resistant prostate cancer. Sci. Signal. 10(480), eaam7479 (2017).
- Min A, Jang H, Kim S et al. Androgen receptor inhibitor enhances the antitumor effect of PARP inhibitor in breast cancer cells by modulating DNA damage response. Mol. Cancer Ther. 17(12), 2507–2518 (2018).
- Chakraborty G, Armenia J, Mazzu YZ et al. Significance of BRCA2 and RB1 co-loss in aggressive prostate cancer progression. Clin. Cancer Res. 26(8), 2047–2064 (2020).
- Agarwal N, Zhang T, Efstathiou E et al. The biology behind combining poly [ADP ribose] polymerase and androgen receptor inhibition for metastatic castration-resistant prostate cancer. Eur. J. Cancer 192, DOI:10.1016/j.ejca.2023.113249 (2023).
- de Bono J, Mateo J, Fizazi K et al. Olaparib for metastatic castration-resistant prostate cancer. N. Engl. J. Med. 382(22), 2091–2102 (2020).
- U.S. Food and Drug Administration . LYNPARZA® (olaparib) prescribing information. ( Revised May 2023).
- LYNPARZA® (olaparib) Summary of Product Characteristics. www.medicines.org.uk/emc/product/9204/smpc (14 May 2021).
- Abida W, Patnaik A, Campbell D et al. Rucaparib in men with metastatic castration-resistant prostate cancer harboring a BRCA1 or BRCA2 gene alteration. J. Clin. Oncol. 38(32), 3763–3772 (2020).
- U.S. Food and Drug Administration . RUBRACA® (rucaparib) prescribing information. ( Revised June 2022).
- Asim M, Tarish F, Zecchini HI et al. Synthetic lethality between androgen receptor signalling and the PARP pathway in prostate cancer. Nat. Commun. 8(1), 374 (2017).
- Gui B, Gui F, Takai T et al. Selective targeting of PARP-2 inhibits androgen receptor signaling and prostate cancer growth through disruption of FOXA1 function. Proc. Natl Acad. Sci. USA 116(29), 14573–14582 (2019).
- Chi KN, Rathkopf D, Smith MR et al. Niraparib and abiraterone acetate for metastatic castration-resistant prostate cancer. J. Clin. Oncol. 41(18), 3339–3351 (2023).
- Clarke NW, Armstrong AJ, Thiery-Vuillemin A et al. Abiraterone and olaparib for metastatic castration-resistant prostate cancer. NEJM Evid. 1(9), DOI:10.1056/EVIDoa2200043 (2022).
- Talazoparib + enzalutamide vs. enzalutamide monotherapy in mCRPC (TALAPRO-2) (NCT03395197). https://clinicaltrials.gov/ct2/show/NCT03395197 (23 February 2023).