

Abstract
The current paper describes the age, period and cohort effects on breast cancer mortality in Taiwan. Female breast cancer mortality data were collected from the Taiwan death registries for 1971–2010. The annual percentage changes, age- standardised mortality rates (ASMR) and age–period–cohort model were calculated. The mortality rates increased with advancing age groups when fixing the period. The percentage change in the breast cancer mortality rate increased from 54.79% at aged 20–44 years, to 149.78% in those aged 45–64 years (between 1971–75 and 2006–10). The mortality rates in the 45–64 age group increased steadily from 1971 to 1975 and 2006–10. The 1951 birth cohorts (actual birth cohort; 1947–55) showed peak mortalities in both the 50–54 and 45–49 age groups. We found that the 1951 birth cohorts had the greatest mortality risk from breast cancer. This might be attributed to the DDT that was used in large amounts to prevent deaths from malaria in Taiwan. However, future researches require DDT data to evaluate the association between breast cancer and DDT use.
Introduction
The incidence rates of breast cancer have been increasing and causing a burden throughout the world (CitationParkin and Fernandez 2006). Furthermore, cancer is a leading cause of death worldwide. According to the World Health Organization (WHO) media centre, a total of 458,000 breast cancer deaths occurred in 2008, which was ranked fifth after lung, stomach, liver and colon cancers (CitationWHO 2011). In Taiwan, the incidence of breast cancer has increased significantly in the past two decades according to the statistics of Department of Health. Breast cancer has been the most common female cancer since 2003. Furthermore, the standardised breast cancer incidence increased by 14.69% from 2003 to 2008 (CitationChang et al. 2012).
The interpretation of breast cancer mortality trends is complicated by the coexisting changes in risk factors, screening programmes and treatment strategies. Age, period of death and birth cohort are the three temporal factors related to cancer mortality. Several studies have applied the age–period–cohort model (APC model) to demonstrate breast cancer mortality trends (CitationOsmond and Gardner 1982; CitationGardner and Osmond 1984). In the age–period–cohort analysis, cohort effects may present some evidences of early stage carcinogens or risk factors that may influence breast cancer mortality and period effects may demonstrate the effects of screening and adjuvant treatment on breast cancer mortality.
Taiwan adopted dichlorodiphenyltrichloroethane (DDT) for malaria control shortly after the Second World War. In 1945, there were over 1 million cases of malaria in the island. However, in 1969, only nine cases were reported, and shortly thereafter, the disease was permanently eradicated. Similarly, spectacular decreases in malaria cases and deaths were seen everywhere DDT was used (CitationWright et al. 1972). The association has been studied between breast cancer and DDT use (CitationCohn et al. 2007).
However, to date, no systematic epidemiological study has been conducted to describe the recent and temporal trends in breast cancer mortality in the Taiwanese population. The current paper describes the age, period and cohort effects on breast cancer mortality in Taiwan.
Materials and methods
The study covers mortality data from 1971 to 2010, which were obtained from the Office of Statistics, Department of Health, in Taiwan. The Taiwanese government requires residents to register deaths in a timely manner, and therefore the deaths registry is comprehensive. The mortality data were initially recorded in 1- or 5-year age bands (0, 1, 2, 3, 4, 5–9, 10–14, 15–19, 20–24, 25–29, 30–34, …, 80– 84, 85–89, 90–94, 95–99 and ≥ 100 years). The International Classification of Diseases (ICD) codes used for mortality were reviewed three times during this period. ICD codes used for breast cancer included: ICD-8 codes (174.0–174.9) for cases diagnosed before 1980; ICD-9 codes (174.0–174.9) for those from 1981 to 2008 and ICD-10 codes (C50.0-C50.9) for those diagnosed in 2009 or later.
To examine breast cancer mortality trends, only mortalities resulting from breast cancer from 1971–2010 among individuals between the ages of 20–80 years were selected. The mortality data were grouped into 13, 5-year age groups (20–24, 25–29, 30–34, … to 80– 84 years), and eight periods (1971–75, 1976–80, 1981, 1985, … and 2006–10). Those born between 1887 and 1895 who died between 1971 and 1975 (80–84 years old) represented the oldest cohort, while those born between 1982 and 1990, who died between 2006 and 2010 (20–24-years old), represented the youngest cohort. Therefore, the data design comprised 20 birth cohorts (the oldest: 1887–95, to the youngest: 1982–90). The age-standardised mortality rates (ASMR) was estimated for each age group. The 2000 World Standard Population data provided by the World Health Organization were used as the reference population. Age-specific mortality rates were calculated by period and birth cohorts.
In the age–period–cohort (APC) model, the best forecast parameterisation model was selected between AP–C and AC–P by calculating the mean absolute percentage error. The AC–P model was chosen by a sequential approach. An age–cohort model was fitted; a period–function was later fitted using the log-fitted values from the age–cohort model as the offset, to produce the period effect conditional on the estimates from the age–cohort model (CitationCarstensen 2007). The standard errors of the resulting estimates were also calculated. The age effects were calculated as rates for the reference period in the age–period model, while the period effects were calculated as rate ratios (RR) relative to the reference period. Cohort effects were derived from the model using the log from the age–period model as the offset. The optimal number of knots was selected by adding an increasing number of knots at subsequent quantiles for age, period and cohort, respectively. The best-fitting model was defined as one that minimised the Akaike information criterion. All estimators were computed using the Epi package provided by the statistical software R.
Results
The mortality rates, number of deaths and increased mortality rates for three age groups (20–44, 45–64 and 65–84 years) during eight periods (1971–75 to 2006–10) are shown in . The mortality rates increased with advancing age groups when fixing the period. The percentage change in breast cancer mortality rate increased from 54.79% in those aged 20–44 years, to 149.78% in those aged 45–64 years (between 1971–75 and 2006–10). In those aged 20–44, the mortality rates increased almost two-fold (from 2.85 per 100,000 in 1971–75 to 5.88 per 100,000 in 1996–2000). The mortality rates in the 45–64 age group increased steadily from 1971–75 to 2006–10. shows the age, period and cohort-specific mortality rates and ASMR for breast cancer. Peak mortality rates (ASMR) were evident in individuals aged 55–59 years during 2006–10, and in those aged 50–54 years during 2001–05 (). The ASMR of breast cancer increased about two-fold from 1971 to 1975 and 2006–10 (). The 1951 birth cohorts (actual birth cohort; 1947–55) showed peak mortalities in both 50–54 and 45–49 age groups (). shows the age, period and cohort estimates derived from APC analysis. The mortality rate increased steadily with age and plateaued at 63.01 per 100,000 people in the 80–84 year-old group (). Period effects suggested slightly raised RRs in the periods 1976–80 and 1991–2000 (). Cohort effects expressed as rate ratio with cohorts born in 1891 was 0.41 (95% CI 0.30–0.56), which rose steadily and attained a peak ratio, 1.99 (95% CI 1.92–2.07) in those born in 1951, before decreasing to 0.63 in 1986 (95% CI 0.30–1.36) ().
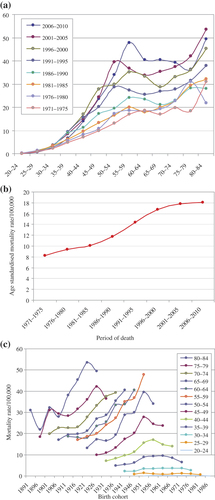
Table I. Observed cases (n), mortality rate, percentage change and corresponding 95% CI for breast cancer in Taiwan, 1971–2010.
Discussion
In this study, we showed that the percentage changes in breast cancer mortality increased in all age groups. The highest change (149.78%) was observed in the age group 45–65 years. Our results are consistent with previous studies (CitationShen et al. 2005; CitationLeong et al. 2010). Significantly increasing trends were noted in age groups: 40–44, 50–54 and 50–64 years, though increasing trends have been reported in all age groups (CitationShen et al. 2005). Furthermore, there was a noticeable difference in the peak age for breast cancer, which was between 40 and 50 years in Asia, but was between 60 and 70 years in Western countries, although there were significant similarities during a comparison of epidemiological and clinical outcome data (CitationLeong et al. 2010). Over the last decades, breast cancer incidence has been increasing worldwide (CitationHortobagyi et al. 2005; CitationIgene 2008; CitationAnderson and Jakesz 2008). The greatest increase in the incidence of breast cancer has been in Asian countries (CitationGreen and Raina 2008). Certain Asian countries have experienced a trend of Westernised lifestyle in recent decades (CitationSeow et al. 1996; CitationNagata et al. 1997). Nutrition, lifestyle and behaviour have been proposed as factors associated with the increased incidence of breast cancer (CitationGerber et al. 2003; CitationMcTiernan 2003). A high fat and low fibre dietary pattern, overweight, a sedentary life pattern, early menarche and delayed childbearing may also increase breast cancer risk.
Three stages of nationwide breast cancer screening programmes evolved in Taiwan between 1995 to 2004: (1) selective screening for those women with 1st-degree relatives with breast cancer, by mammography, ultrasound and physical examination from 1995–98; (2) a mass screening programme by public health nurses through physical examination from 1999–2001 and (3) a two-stage breast cancer screening programme using risk-factor questionnaires and mammography for moderate-to-high risk women from 2002 to 2004 (CitationChang et al. 2008). From the results seen in , it can be seen that the age-standardised mortality rate per 100,000 increased more slowly between 1996 and 2000. This may be due to the breast cancer screening programme in Taiwan.
Our study showed a strong birth cohort effect on breast cancer mortality (). This is consistent with other studies that assessed the trend or breast cancer incidence in different geographic areas (CitationPersson et al. 1993; CitationRobertson and Boyle 1997; CitationRostgaard et al. 2001; CitationMinami et al. 2004). Birth cohort has been used to examine birth cohort trends in breast cancer mortality and also may contribute to lifestyle and environmental factors leading to breast cancer (CitationTarone and Chu 1992). In this study, those aged 55–59 years in 2006–10 and 50–54 years in 2001–05 were in the same birth cohort (1947–55) and showed peak mortalities (ASMR), as shown in . also shows a peak in both age groups 50–54 and 45–49 in the birth cohort 1951. A peak in the rate ratio was evident in the 1951 birth cohort, as shown in . A 6-year malaria eradication programme using the DDT residual house spraying method was launched in Taiwan in 1952 (CitationLiang 1991). High levels of serum DDT predicted a statistically significant five-fold increased risk of breast cancer among women who were exposed to DDT when under 14 years of age. Women who were not exposed to DDT before the age of 14 showed no association between DDT and breast cancer. Thus, exposure to DDT early in life may increase breast cancer risk. The public health significance of DDT exposure early in life may be large (CitationCohn et al. 2007). The use of DDT in large amounts almost began with the 1951 birth cohorts which, in this study, were observed to have greatest mortality risk from breast cancer. This result is consistent with Cohn's work carried out in 2007.
We only included breast cancer cases in women between the ages of 20 and 84 years. Inclusion of cases > 85 years in the APC model might have generated a cohort effect due to measurement error. The original database made use of a 5-year trend aggravated data. Cases ≥ 85 years were designated to one group. In the APC model, the cohort groups were calculated according to age and period groups. If cases ≥ 85 were included in the study, their birth cohorts by 2006–10, and those in the 80–84 age group at 2001–05 could not have been in the same cohort. Conversely, individuals aged 20 and below included very few deaths, thus only those between 20 and 84 years were considered to ensure adequate reliability of the estimates. No sensitivity analyses were performed. However, we think the impact that such analyses may have had on our results, would be minimal. We excluded individuals under 20 and over 80 in order to have more reliable estimates.
Conclusion
We found that the 1951 birth cohorts had the greatest mortality risk from breast cancer. This might be attributed to DDT that was used in large amounts to prevent deaths from malaria in Taiwan. However, future researches require DDT data to evaluate the association between breast cancer and DDT use.
Declaration of interest: The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
- Anderson BO, Jakesz R. 2008. Breast cancer issues in developing countries: an overview of the breast health global initiative. World Journal of Surgery 32:2579–2585.
- Carstensen B. 2007. Age-period-cohort models for the Lexis diagram. Statistics in Medicine 26:3018–3045.
- Chang KJ, Kuo WH, Wang MY. 2008. The epidemiology of breast cancer in Taiwan. Journal of Chinese Oncology 24:85–93.
- Chang LY, Yang YL, Shyu MK, Hwa HL, Hsieh FJ. 2012. Strategy for breast cancer screening in Taiwan: obstetrician–gynecologists should actively participate in breast cancer screening. Journal of Medical Ultrasound 20:1–7.
- Cohn BA, Wolff MS, Cirillo PM, Sholtz RI. 2007. DDT and breast cancer in young women: new data on the significance of age at exposure. Environmental Health Perspectives 115: 1406–1414.
- Gardner MJ, Osmond C. 1984. Interpretation of time trends in disease rates in the presence of generation effects. Statistics in Medicine 3:113–130.
- Gerber B, Muller H, Reimer T, Krause A, Friese K. 2003. Nutrition and lifestyle factors on the risk of developing breast cancer. Breast Cancer Research and Treatment 79: 265–276.
- Green M, Raina V. 2008. Epidemiology, screening and diagnosis of breast cancer in the Asia-Pacific region: current perspectives and important considerations. Asia-Pacific Journal of Clinical Oncology 4(Suppl 3): S5–S13.
- Hortobagyi GN, de la Garza Salazar J, Pritchard K, Amadori D, Haidinger R, Hudis CA, et al. 2005. The global breast cancer burden: variations in epidemiology and survival. Clinical Breast Cancer 6:391–401.
- Igene H. 2008. Global health inequalities and breast cancer: an impending public health problem for developing countries. Breast Journal 14: 428–434.
- Leong SP, Shen ZZ, Liu TJ, Agarwal G, Tajima T, Paik NS, et al. 2010. Is breast cancer the same disease in Asian and Western countries?World Journal of Surgery 34:2308–2324.
- Liang KC. 1991. Historical review of Malaria control program in Taiwan. Kaohsiung Journal of Medical Sciences 7:271–277.
- McTiernan A. 2003. Behavioral risk factors in breast cancer: can risk be modified?Oncologist 8:326–334.
- Minami Y, Tsubono Y, Nishino Y, Ohuchi N, Shibuya D, Hisamichi S. 2004. The increase of female breast cancer incidence in Japan: emergence of birth cohort effect. International Journal of Cancer 108: 901–906.
- Nagata C, Kawakami N, Shimizu H. 1997. Trends in the incidence rate and risk factors for breast cancer in Japan. Breast Cancer Research and Treatment 44:75–82.
- Osmond C, Gardner MJ. 1982. Age, period and cohort models applied to cancer mortality rates. Statistics in Medicine 1:245–259.
- Parkin DM, Fernandez LM. 2006. Use of statistics to assess the global burden of breast cancer. Breast Journal 12(Suppl 1):S70–S80.
- Persson I, Bergstrom R, Sparen P, Thorn M, Adami HO. 1993. Trends in breast cancer incidence in Sweden 1958–1988 by time period and birth cohort. British Journal of Cancer 68:1247–1253.
- Robertson C, Boyle P. 1997. Statistical modelling of breast cancer incidence and mortality rates in Scotland. British Journal of Cancer 76:1248–1252.
- Rostgaard K, Vath M, Holst H, Madsen M, Lynge E. 2001. Age–period– cohort modeling of breast cancer incidence in the Nordic countries. Statistics in Medicine 20:47–61.
- Seow A, Duffy SW, McGee MA, Lee J, Lee HP. 1996. Breast cancer in Singapore: trends in incidence 1968–1992. International Journal of Epidemiology 25:40–45.
- Shen YC, Chang CJ, Hsu C, Cheng CC, Chiu CF, Cheng AL. 2005. Significant difference in the trends of female breast cancer incidence between Taiwanese and Caucasian Americans: implications from age-period- cohort analysis. Cancer Epidemiology, Biomarkers and Prevention 14: 1986–1990.
- Tarone RE, Chu KC. 1992. Implications of birth cohort patterns in interpreting trends in breast cancer rates. Journal of the National Cancer Institute 84:1402–1410.
- WHO. 2011. World Health Organization Medical Center “Cancer” 2011. Available at: www.who.int/mediacentre/factsheets/fs297/en/index.htm.
- Wright JW, Fritz RF, Haworth J. 1972. Changing concepts of vector control in malaria eradication. Annual Review of Entomology 17:75–102.