
CASE REPORT
A 12-month-old male with bilateral anophthalmia presented with an increasing “bump” of the right upper eyelid noted 2 months prior. Examination revealed a soft, palpable fullness of the right upper eyelid, with conformers in the appropriate position bilaterally and no discharge or periorbital erythema or edema. MRI of the orbits revealed a 2.8-cm lobular mass in the superolateral right extraconal orbit with mild intrinsic T1 shortening, fat suppression, and diffusion restriction most consistent with a dermoid cyst (). Histopathologic review following anterior orbitotomy with excisional biopsy revealed an thin- walled encapsulated lesion lined by compressed keratinized squamous epithelium and an abundant keratinaceous debris consistent with a dermoid cyst.
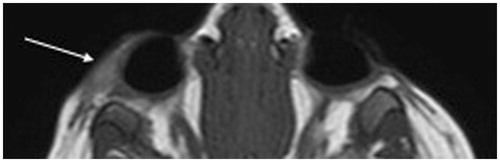
FIGURE 1. MRI showing 2.8-cm lobular mass in the superolateral right pre-septal orbit extending post-septally in the extraconal orbit above the lacrimal gland towards the posterior orbit with mild intrinsic T1 shortening, fat suppression, diffusion restriction most consistent with a lobular dermoid cyst.
COMMENT
Dermoid cysts represent the most common benign space-occupying mass of the orbit in children.Citation1 The incidence of anophthalmia or microphthalmia ranges from 0.4–1.4 per 10,000 live births.Citation2–4 Most dermoids are idiopathic, but an association has been noted in some heritable genetic syndromes, and in association with rubella, alcohol, thalidomide, retinoic acid,Citation5,Citation6 hydantoin,Citation7 and LSD. Dermoids arise from sequestration of embryonic epithelium between orbital bones, are slow growing, most commonly occur in the superotemporal or superonasal quadrants, and typically present as an enlarging mass.Citation8,Citation9 Imaging often reveals a fluid signal on MR and restriction on diffusion weighted imaging.Citation10 Definitive diagnosis is made through histopathologic review.Citation11 Although dermoid cysts have never been reported in the setting or bilateral anophthalmia, they should be considered in the differential diagnosis in the appropriate clinical setting.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
- Bonavolonta G, Strianese D, Grassi P, et al. An analysis of 2480 space-occupying lesions of the orbit from 1976 to 2011. Ophthal Plast Reconstr Surg 2013;29(2):79–86
- Busby A, Dolk H, Collin R, et al. Compiling a national register of babies born with anophthalmia/microphthalmia in England 1988–94. Arch Dis Child Fetal Neonatal Ed 1998;79(3):F168–F173
- Shaw GM, Carmichael SL, Yang W, et al. Epidemiologic characteristics of anophthalmia and bilateral microphthalmia among 2.5 million births in California, 1989–1997. Am J Med Genet A 2005;137(1):36–40
- Lowry RB, Kohut R, Sibbald B, Rouleau J. Anophthalmia and microphthalmia in the Alberta Congenital Anomalies Surveillance System. Can J Ophthalmol 2005;40(1):38–44
- Fraunfelder FT, LaBraico JM, Meyer SM. Adverse ocular reactions possibly associated with isotretinoin. Am J Ophthalmol 1985;100(4):534–537
- Lammer EJ, Chen DT, Hoar RM, et al. Retinoic acid embryopathy. N Engl J Med 1985;313(14):837–841
- Hampton GR, Krepostman JI. Ocular manifestations of the fetal hydantoin syndrome. Clin Pediatr (Phila) 1981;20(7):475–478
- Sherman RP, Rootman J, Lapointe JS. Orbital dermoids: clinical presentation and management. Br J Ophthalmol 1984;68(9):642–652
- Hopper KD, Sherman JL, Boal DK, Eggli KD. CT and MR imaging of the pediatric orbit. Radiographics 1992;12(3):485–503
- Khanna G, Sato Y, Smith RJ, et al. Causes of facial swelling in pediatric patients: correlation of clinical and radiologic findings. Radiographics 2006;26(1):157–171
- Shields JA, Kaden IH, Eagle RC, Shields CL. Orbital dermoid cysts: clinicopathologic correlations, classification, and management. The 1997 Josephine E. Schueler Lecture. Ophthal Plast Reconstr Surg 1997;13(4):265–276