
Abstract
Background: During radiofrequency (RF) hyperthermia treatment, hot-spot phenomena may occur and prevent treatment continuation if the output is not lowered. We previously reported a significant correlation between the initial energy output at which output-limiting symptoms occurred and patient status. Patients with a complete clinical response had significantly increased temperature, while some patients with partial clinical response and stable disease had increased temperature, depending on the occurrence of output-limiting symptoms. To predict the initial energy output at which output-limiting symptoms occur, we performed multiple regression analysis with the parameters of patients’ physical status. Materials and methods: Hyperthermia alone or concomitant with chemotherapy and/or radiotherapy was applied in 62 patients with malignant disease for a total of 310 treatments with a Thermotron RF-8 between December 2011 and April 2014. Results: No output-limiting symptoms were shown in 65.5% of 310 treatments. Pain (29.7%), micturition desire (1.9%), skin discomfort (0.6%), subcutaneous induration (1.6%), cold sensation (0.6%), and nausea (0.3%) were reported in the 310 treatments. A good predictive equation for initial energy output at which output-limiting symptoms occur was determined with two parameters, initial time of an output-limiting symptom onset, and thickness of the fat of the abdominal wall. Multiple regression analysis showed an adjusted R2 = 0.99 and variance inflation factor < 2. Conclusions: We present a good predictive equation for initial energy output at which output-limiting symptoms occur. It is critical to prevent RF hyperthermia-induced output-limiting symptoms and establish new prevention strategies.
Introduction
Hyperthermia has been used for cancer therapy over the past three decades. There are numerous positive phase III trials indicating that it can enhance the efficacy of both radiotherapy and chemotherapy [Citation1]. Although it has been proven effective in many circumstances, the treatment requires exposure of a portion of the body to externally applied power, such as radiofrequency. Under some circumstances pain that is associated with the treatment limits the amount of power that can be applied. In such circumstances it is possible that substandard hyperthermia application will result, thereby lessening its therapeutic effectiveness.
In our study of capacitively coupled RF hyperthermia, we found a significant positive correlation between the initial energy output at which output-limiting symptoms occurred and the time of an output-limiting symptom onset. Initial energy output also had a significant negative correlation to the patient’s physical status. Body mass index (BMI), visceral fat area, total fat area, thickness of the abdominal wall fat, subcutaneous fat area, abdomen girth and body weight were used to define physical status of patients. All patients with a clinical complete response (CR) had significantly higher skin temperatures than other groups. Output-limiting symptoms associated with energy output were correlated with occurrence of complete response (CR), clinical partial response (PR), stable disease (SD) or disease progression. Elevation of temperature was also associated with response [Citation2].
The hot-spot phenomenon, thought to result from large RF reflections at the interface between soft tissue and bone or air, can also cause severe output-limiting symptoms, including pain, unpleasant sensations and burning at maximum power of the RF equipment [Citation3–8]. Patients who experience these side effects may not receive optimal hyperthermia treatment because of limitations in applied power. If these output-limiting symptoms can be predicted and prevented, patients may be able to better tolerate application of hyperthermia, thereby maximising the likelihood that they will be effectively treated.
In this study we aimed to establish a predictive formula of the initial energy output at which output-limiting symptoms occur by using a multiple regression analysis with parameters such as the time of an output-limiting symptom onset and physical status of patients treated with hyperthermia.
Materials and methods
Hyperthermia alone (HT) or concomitant with chemotherapy (CT) and/or radiotherapy (RT) performed on 62 patients with malignant diseases (median age 65 years; range 33–89 years, male:female ratio 45:17, 48 primary and six recurrent rectal cancers, six recurrent colon cancers, one primary pancreas cancer, and one recurrent pseudomixoma), for a total of 310 abdominal treatments by using a Thermotron RF-8 (Yamamoto Vinita, Osaka, Japan) between December 2011 and April 2014.
Hyperthermia
Abdominal HT was applied five times per week for 50 min per treatment. From December 2011 to November 2012, a total of 26 patients began receiving CT and/or RT first through oral administration of fluoropyrimidine and/or a total dosage of 50 Gy by intensity-modulated radiotherapy. Patients then received RF thermal therapy either on the same day or on the next day, and continued to receive the same treatment cycle weekly. RF output was started from 300 W and increased by operators to 1200 W until output-limiting symptoms occurred. When these symptoms occurred, the output was decreased and increased again when symptoms reappeared, with output varying roughly from patient to patient. This method of adjusting power was recorded, but not standardised. To determine whether power adjustments affected treatment outcome, the data were retrospectively evaluated.
From November 2012 to January 2014, a total of 36 patients prospectively received a treatment with standardised power escalation principles. From retrospective evaluation of the data about output-limiting symptoms, we had noticed that patients with output-limiting symptoms showed greater thickness of the abdominal wall, internal organs fat area and total fat area than those without output-limiting symptoms. Therefore, we classified patients into two groups. Group A comprised patients with thickness of the fat of abdominal wall <16 mm, visceral fat area <100 cm2, and total fat area <190 cm2, and group B comprised patients with any one of the aforementioned factors. For patients in group A, the output increase was 50 W/min, while for those in group B it was 25 W/min. The operator started the output at 200 W and increased to 1200 W until output-limiting symptoms occurred and then decreased the output by 100 W. Most patients did not complain and continued the first RF thermal treatment. Subtracting 100 W output was judged as the optimal energy output dose without output-limiting symptoms. From the second to fifth RF thermal treatment, this output was applied for 50 min. These principles were maintained in patients with standardised power escalation principles in this prospective study [Citation2].
The study was approved by the ethics committee of Hidaka Hospital and Gunma University and each patient provided written informed consent before being accepted into the study. The physical status of all patients; thickness of the fat of the abdominal wall at the level of the navel, subcutaneous fat area, total fat area, and internal organ fat area were evaluated using computer tomography/magnetic resonance imaging (CT/MRI) before treatment. Height, body weight, body mass index (BMI), abdomen girth, body surface area calculated by the DuBois formula (BSA = W0.425 × H0.725 × 0.007184) and age were also recorded.
Multiple regression analysis
We analysed the correlations between the initial energy output at which output-limiting symptoms occurred, the initial time at which output-limiting symptoms occurred, and patients’ physical status such as body weight, height, BMI, and age as well thickness of the fat of the abdominal wall, internal organ fat area, total fat area and subcutaneous fat area, which were used as exploratory variables for multiple regression analysis. Variance inflation factor (VIF) was used to check for multicollinearity. The predictor equation was determined using a correlation analysis and executing a combination of stepwise and multiple linear regressions.
Statistical analysis
The SPSS Statistics package (IBM, Armonk, NY, USA), version 21, was used to analyse all data. For statistical efficiency we used a stepwise multiple regression method to predict the initial energy output at which an output-limiting symptom occurred. The correlations were evaluated using Pearson correlation coefficients (r) and significance values (p). Categorical data were analysed using the χ2-test. All reported p-values were two-tailed and considered significant if p < 0.05.
Results
There was no significant difference between patients with and without output-limiting symptoms in gender and age (<65 years old and >66 years old). Output-limiting symptoms of 310 treatments occurred in 64.5% and 35.5% of patients <65 years old and >66 years old, respectively; this difference was significant (p = 0.013), and in 56.1% and 43.9% of patients without and with standardised power escalation principles, respectively (p < 0.001). There was no significant difference between patients with and without output-limiting symptoms in combination treatments (HT plus CT plus RT (n = 56), HT plus RT (n = 2), HT plus CT (n = 3) and HT (n = 1)). Pain (29.7%), micturition desire (1.9%), skin discomfort (0.6%), subcutaneous induration (1.6%), cold sensation (0.6%), and nausea (0.3%) were reported for 310 treatments. The patients’ physical status with and without output-limiting symptoms in applied abdominal thermal therapy are summarised in . Patients with output-limiting symptoms had a significantly higher body weight and thicker abdominal wall fat than those without output-limiting symptoms (p = 0.05 and p = 0.028, respectively). shows the results of multiple regression analysis in patients who received abdominal thermal therapy with and without standardised power escalation principles. Adjusted R2 were 0.99 and 0.90 in patients with and without standardised power escalation principles, respectively, and all VIF values were less than 2. There was no multicollinearity in the model. We attempted to use a forced entry multiple regression method to predict the initial energy output at which output-limiting symptoms occurred, but all the adjusted R2 values were less than that obtained using stepwise regression.
Table 1. Characteristics of patients’ physical status with and without output-limiting symptoms.
Table 2. Results of multiple regression analysis in patients receiving abdominal irradiation with and without standardised power escalation principles.
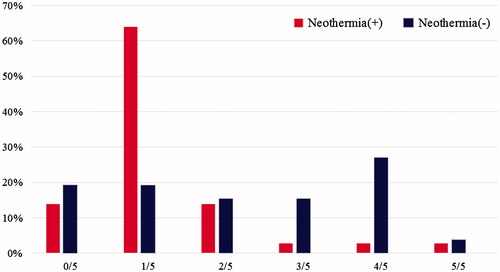
shows the incidence of output-limiting symptoms during the five RF treatment sessions. Almost all patients receiving standardised power escalation principles developed output-limiting symptoms only once during the five treatment sessions, while those without standardised power escalation principles developed several output-limiting symptoms during the five treatment sessions. There was a significant difference in distribution between them (p < 0.001). No output-limiting symptoms during five treatments (310 abdominal thermal therapy) were observed in 73.9% and 53.8% patients with and without standardised power escalation principles, respectively. There was a significant difference between them (p < 0.001).
Figure 1. Incidence of output-limiting symptoms during five RF treatments. Patients with standardised power escalation principles developed output-limiting symptoms only once during five treatments, while those without standardised power escalation principles developed several output-limiting symptoms during five treatments.
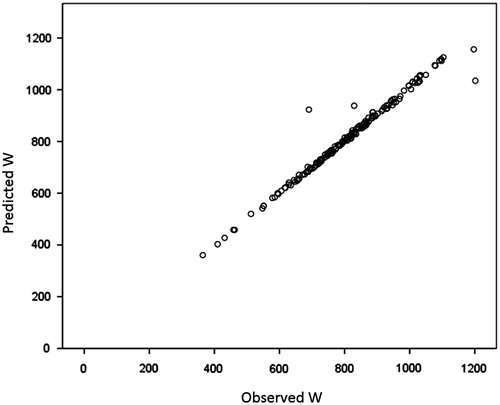
shows the relationship between the observed and expected initial energy output at which output-limiting symptoms occurred in patients receiving abdominal thermal therapy with standardised power escalation principles. There was a good correlation between the observed and expected initial energy output obtained with the two parameters.
Figure 2. Relationship between the observed and expected initial irradiation output at which output-limiting symptoms occurred in patients receiving abdominal irradiation with standardised power escalation principles, in watts.
Discussion
In this study we demonstrated that a good predictor equation for initial energy output at which output-limiting symptoms occurred was determined with two parameters: time of an output-limiting symptom onset, and thickness of the fat of the abdominal wall. However, this conclusion is limited due to the small sample of this study.
It has been demonstrated in several prior clinical studies with deep hyperthermia that higher thermal doses are associated with better response. The achievement of optimal thermal doses requires deposition of adequate power, as we have reported previously [Citation2], to the target tumour volume. To date, however, there have been no reports examining the relationship between RF output and thermal dose achieved in individual patients with deep-seated tumours, and no one has examined what factors might contribute to onset of pain during capacitive RF heating.
The hyperthermia group in Rotterdam reported that the Rotterdam method detailed a hyperthermia treatment planning system for which they calculated specific absorption rate (SAR) distributions and the successful outcomes of hyperthermia in patients with cervical cancer. They also reported that areas of pain correlated with modelled SAR peak locations [Citation9–15].
SAR is a good parameter for standardisation of therapy and prediction of output-limiting symptoms with phased array devices. We show that time of onset of symptoms is associated with outcome. A future direction for those involved in phased array devices might be to examine this relatively simple tool. Fat thickness is an issue that is particularly limiting for capacitive RF devices. Whether or not this would be helpful with phased array devices would have to be tested.
Conclusion
In conclusion, we developed a good predictive equation for the initial energy output at which an output-limiting symptom will occur using the time of output-limiting symptom onset and thickness of the fat of the abdominal wall as parameters. Our results show that it is very important to prevent RF hyperthermia-induced output-limiting symptoms. New strategies need to be established for the prevention of output-limiting symptoms.
Acknowledgements
We would like to thank all participating patients and the radiological technicians Satoshi Suda, Kouji Sugawara, and Kazuki Jinbo for their assistance.
Declaration of interest
No specific funding was used for this study. The authors have no disclosure or financial support to declare. The authors alone are responsible for the content and writing of the paper.
References
- Datta NR, Ordóñez SG, Gaipl US, Paulides MM, Crezee H, Gellermann J, et al. Local hyperthermia combined with radiotherapy and/or chemotherapy: Recent advances and promises for the future. Cancer Treat Rev 2015;41:742–53. doi: 10.1016/j.ctrv.2015.05.009
- Shoji H, Motegi M, Osawa K, Okonogi N, Andou Y, Asao T, et al. Does standardization of radiofrequency hyperthermia benefit patients with malignancies? Ann Cancer Res Ther 2014;22:28–35
- Hiraoka M, Jo S, Akuta K, Nishimura Y, Takahashi M, Abe M. Radiofrequency capacitive hyperthermia for deep-seated tumors II. Effect of thermoradiotherapy. Cancer 1987;60:128–35
- Lee CK, Song CW, Rhee JG, Foy JA, Levitt SH. Clinical experience using 8 MHz radiofrequency capacitive hyperthermia in combination with radiotherapy: Results of a phase I/II study. Int J Radiat Oncol Biol Phys 1995;32:733–45
- Wust P, Stahl H, Löffel J, Seebass M, Riess H, Felix R. Clinical, physiological and anatomical determinants for radiofrequency hyperthermia. Int J Hyperthermia 1995;11:151–67
- Van der Zee J, Van der Holt B, Rietveld PJ, Helle PA, Wijnmaalen AJ, van Putten WL, et al. Reirradiation combined with hyperthermia in recurrent breast cancer results in a worthwhile local palliation. Br J Cancer 1999;79:483–90
- Kok HP, van Haaren PM, van de Kamer JB, Zum Vörde Sive Vörding PJ, Wiersma J, Hulshof MC, et al. Prospective treatment planning to improve locoregional hyperthermia for oesophageal cancer. Int J Hyperthermia 2006;22:375–89
- Wiersma J, Van Wieringen N, Crezee H, Van Dijk JD. Delineation of potential hot spots for hyperthermia treatment planning optimisation. Int J Hyperthermia 2007;23:287–301
- Van der Zee J, Gonzalez Gonzalez D, Van Rhoon GC, Van Dijk JD, van Putten WL, Hart AA. Comparison of radiotherapy alone with radiotherapy plus hyperthermia in locally advanced pelvic tumours: A prospective, randomised, multicentre trial. Dutch Deep Hyperthermia Group. Lancet 2000;355(9210):1119–25
- Van Rhoon GC, Van Der Heuvel DJ, Ameziane A, Rietveld PJ, Volenec K, Van Der Zee J. Characterization of the SAR distribution of the Sigma-60 applicator for regional hyperthermia using a Schottky diode sheet. Int J Hyperthermia 2003;19:642–54
- van der Wal E, Franckena M, Wielheesen DH, van der Zee J, van Rhoon GC. Steering in locoregional deep hyperthermia: Evaluation of common practice with 3D-planning. Int J Hyperthermia 2008;24:682–93
- de Bruijne M, Van der Zee J, Ameziane A, Van Rhoon GC. Quality control of superficial hyperthermia by treatment evaluation. Int J Hyperthermia 2011;27:199–213
- Linthorst M, Drizdal T, Joosten H, van Rhoon GC, van der Zee J. Procedure for creating a three-dimensional (3D) model for superficial hyperthermia treatment planning. Strahlenther Onkol 2011;187:835–41
- Canters RAM, Franckena M, van der Zee J, van Rhoon GC. Optimizing deep hyperthermia treatments: Are locations of patient pain complaints correlated with modelled specific absorption rate (SAR), of which distributions of the Sigma-60 applicator are in good agreement with theoretically expected values, peak locations? Phys Med Biol 2011;56:439–51
- Canters RAM, Paulides MM, Franckena MF, van der Zee J, van Rhoon GC. Implementation of treatment planning in the routine clinical procedure of regional hyperthermia treatment of cervical cancer: An overview and the Rotterdam experience. Int J Hyperthermia 2012;28:570–81