
Abstract
The everyday communication of children is commonly observed by their parents. This paper examines the responses of parents (n = 18) who had both a Cochlear Implant (CI) and a Normal Hearing (NH) child. Through an online questionnaire, parents rated the ability of their children on a gamut of speech communication competencies encountered in everyday settings. Comparative parental ratings of the CI children were significantly poorer than those of their NH siblings in speaker recognition, happy and sad emotion, and question versus statement identification. Parents also reported that they changed the vocal effort and the enunciation of their speech when they addressed their CI child and that their CI child consistently responded when their name was called in normal, but not in noisy backgrounds. Demographic factors were not found to be linked to the parental impressions.
Introduction
While successive technological generations of cochlear implant (CI) devices may have facilitated some improvements in speech perception in quiet, many CI recipients still experience considerable difficulty in perceiving the fine detail of speech and in understanding speech in adverse acoustic environments. Parents are in a unique position to comment knowledgeably about the hearing ability of their own children in listening environments that are encountered in everyday life. They could also be expected to be reliable respondents and oftentimes they are their child’s most frequent communication partners. Parent–child interaction has been shown to play a key role in the child’s language and emotional development (Calderon, Citation2000; Moeller, Citation2000). The position of parents as common communicators has been exploited in standardised questionnaires that provide clinicians with outcome measures following hearing aid fitting or cochlear implant mapping. Parental impressions have been found to be sensitive to changes in a child’s hearing status over time (Ching & Hill, Citation2007; Ching, Hill, & Dillon, Citation2008; Coninx et al., Citation2009) and to post-implantation improvements in CI children (Purdy, Farrington, Moran, Chard, & Hodgson, Citation2002).
Cohabiting siblings are good subjects for comparison, as the domestic language environment to which they are exposed is likely to be similar. We were interested in how the loss of fine-grained spectral and pitch detail (Moore, Citation2003) would affect daily listening by CI children in comparison to their normal hearing (NH) siblings. One area on which we wanted to focus was the prosodic perceptual ability of both groups as this has been reported as being lower for CI children than for their NH peers. Lyxell et al. (Citation2009) measured prosodic perceptual ability with 2-alternative forced choice identification tasks involving vowel quantity and word stress contrasts. They found that performance on these tasks was significantly poorer for the CI children than the NH control group. Moreover, when elicited via a structured interaction task, the word and phrase-level prosody production of CI children was found to be poorer than that of their NH peers. This is particularly relevant in light of the possibility that production and perception of speech prosody by prelingually-deafened CI recipients may be linked. This linkage has been reported by Peng, Tomblin, and Turner (Citation2008) who found that a panel of adult listeners judged the accuracy of question and statement sentence production by older CI children and adolescents, elicited during an interactive task, to be 73% while it was at ceiling for age-matched NH speakers. Furthermore, they found that production scores from the CI children were highly correlated with the perceptual results from the same children measured with a question/statement sentence identification task. O’Halpin (Citation2010) tested the ability of a group of 16 CI children and adolescents aged between two and 16 to identify the word in focus from sentences containing two (e.g. it’s a BLUE BOOK) and three (e.g. the DOG is EATING a BONE) focus word candidates. She found that on the two-focus task 10 CI subjects scored below chance and on the three-focus task four CI subjects scored below chance, while on both tasks all NH subjects scored above chance.
Given the prosody perceptual deficits that have been reported in paediatric cochlear implant recipients, it was deemed likely that regular communication partners of CI children, like parents, may compensate by altering their speech. For instance, mothers have been shown to be more prone to repeat utterances rather than expand on them when speaking to their hearing impaired child (Nienhuys, Cross, & Horsborough, Citation1984). Also, a comparative analysis of the infant-directed speech of NH mothers to their CI children found that they introduced significantly longer pauses between utterances and they had lower speech rates (syllables per second) when their speech was directed to their CI child than to a NH child matched for hearing experience (Bergeson, Miller, & McCune, Citation2006). Although infant-directed speech is usually slower, there may be a language-specific exception, as data from Danish parents addressing their NH infants show no rate reduction when compared to adult-directed speech (Bohn, Citation2013). From these previous reports of parental speech production, it is unclear as to whether the Danish parents of CI children would modify their speech and whether they would be conscious of changes in both vocal effort and enunciation when communicating with their CI child as opposed to their NH child.
In investigating prosodic cues we were particularly concerned with parental reports of the perceptual ability of children to perceive the emotional content of an utterance. Our interest in this was in order to ascertain if the acoustic cues that signal emotion in speech are available to CI children to the same extent as they would be to their NH siblings. The perception of emotion in speech is also tacitly linked to the long-term understanding and regulation of emotion. Wiefferink, Rieffe, Ketelaar, and Frijns (Citation2012) have shown that CI and NH children attain different levels on a nexus of intersecting indices including emotion regulation, socialisation and language skills. They found that parents of CI children reported that their children were prone to more frequent and intense expressions of negative emotions. However, in laboratory behavioural tests that sought to evoke emotions, CI children did not externalise their emotional response more than their NH peers.
Based on these previous findings, the goal of the present study was to exploit the sensitivity of parents in assessing the proficiency with which CI and NH siblings perceived nuance in speech. Specifically, our aims were threefold. Firstly, to compare CI and NH siblings perception of (i) prosodic cues in speech, such as question/statement and emotional content identification, (ii) speech in common and challenging listening conditions, and (iii) paralinguistic attributes of speech, like speaker recognition. Secondly, to investigate whether parents change their speech when it is directed to their CI child as opposed to their NH child and how adept the CI child is at responding in normal-domestic and noisy backgrounds. Thirdly, to examine the relationship between parental ratings and demographic variables such as age, age at implantation and duration of CI use. We hypothesised that the responses of parents would be worse for CI children on the prosodic tasks of emotion and question/statement identification and the perception of narrow focus. We also expected that parents would indicate that CI children had considerably more difficulty in responding in a noisy situation than in a situation with a normal noise background and that parents would rate that their CI children would neither be able to identify a known speaker nor imitate intonation as well as their NH siblings. As demographic factors like age at implantation and duration of experience with the CI have been linked to language development in implanted children (Boons et al., Citation2012; Szagun & Stumper, Citation2012), we expected that the difference in scores between parental evaluation of NH and CI children would vary systematically with these factors.
The potential advantage of investigating these topics is that it will highlight deficiencies in the communication ability of CI children during formative phases of their development. It will shed light on how communication factors like alterations in parental voice and acoustic properties of the surroundings influence a child’s perception in everyday situations. It will identify demographic variables that may have a bearing on speech perceptual abilities, and it will also contribute to the sparse reports of parental impressions of their implanted child’s communication.
Methods
Participants
Parents (n = 18) who had both a CI and a NH child took part in this study. The CI children had a mean age of 7 years 6 months (SD 2 years 9 months) and the mean age at implantation was 2 years 6 months (SD 2 years 7 months). All of the CI children except for two had been bilaterally implanted. The mean age of the NH children was 6 years 5 months (SD 2 years 8 months) and five were younger and 13 older than their CI siblings. Demographic details of the children and their NH reference siblings are provided in
Table 1. Demographic data of the CI and NH participants.
Questionnaire
A questionnaire was prepared for this study that consisted of 11 items which were formulated so as to be readily understandable for busy parents (Appendix). The first item addressed the ability of both CI and NH children to identify voices in the absence of visual cues. The second, third and fourth item addressed the ability of children to identify emotions. We chose to focus on happy, angry and sad as these are all basic emotions (Ekman, Sorenson, & Friesen, Citation1969) and had been used previously in the coping task employed in Wiefferink et al. (Citation2012) and in the emotion identification task in Fujiki, Spackman, Brinton, & Illig (Citation2006). The fifth item investigated the ability of the children to imitate emotions in their own speech, while the sixth and seventh items addressed the ability of the children to perceive narrow focus and identify when a question was posed. Answers to items one to seven were recorded on a five-point scale where one was “never” and five was “always”. The next two items required parents to rate the difference in the vocal effort (item eight) and the enunciation (item nine) of their own speech when addressing their CI child as opposed to their NH child. Ratings were made on a five-point scale where one was “not different” and five was “completely different”. The final two items required parents to rate the frequency with which their CI child reacted to their name being called in environments with noisy and normal noise backgrounds, where one was “never” and five was “always”. All items included a prompt to a specific domestic scenario where we expected the perceptual ability in question to surface. For example, item six addresses the perception of narrow focus and includes a scenario where parent and child are playing with balls. In this scenario, the parent uses narrow focus to draw the child’s attention to the colour of a particular ball.
Results
The mean total score for the NH group on the first seven questions was 4.9 (SD 0.6) and for the CI group it was 4.3 (SD 0.9). Although the mean CI group score was lower, CI03, CI09 and CI15 did score as well as their NH siblings on the first seven comparative items. To examine the association between parental ratings of CI and NH children multiple pairwise comparisons were carried out with Wilcoxon rank sum tests with group (CI or NH) as the between-subject factor. The sample sizes were equal and Bonferroni post hoc corrections were applied. Results from these are also presented in
Table 2. Mean (and standard deviation) from items involving parental ratings of both their CI and NH child’s perceptual ability.
To assess the internal consistency of the responses to the questionnaire, Cronbach’s alpha was calculated. This value reflects the variance in the scores and is appropriate to use with ordinal data like responses on a Likert scale. The overall value for the first seven items was 0.78 where one represents perfect reliability (Crocker & Algina, Citation1986). Cronbach’s alpha if item deleted, shown in , provides values for how the alpha would change if that question was not included in the questionnaire. The corrected item-total correlation is the correlation between the item and the composite score from all other items. The value of this correlation was low for item five, which may have reflected that the imitation skills assessed by this item reflected the speech production ability of the children and this was unrelated to the perceptual abilities measured by the other items.
Parental voice alteration and reaction to name
The responses to item eight (vocal effort) and item nine (enunciation) are shown in . To investigate whether parents reported compensating in their own speech when addressing their CI child, we performed one-sample t-tests on these results. These revealed that parents reported that they altered both the vocal effort (t20 = 3.4, p < 0.01) and the enunciation of their speech (t20 = 5.1, p < 0.01). However, responses on these two items were highly correlated (r = 0.71, p < 0.001) indicating that parents may not have been able to distinguish between these attributes of their own speech production.
Figure 1. Mean and standard deviation for items 8 to 11 showing parental ratings of vocal effort and enunciation in their own speech (left panel) and the frequency with which their CI child responds to their name being called (right panel).
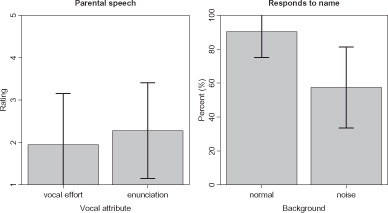
Responses to items dealing with the child’s reaction to their name being called in a noisy (item 10) and a normal background (item 11) were converted into percentages, where one (never) was 0% and five (always) was 100%. The mean score on the item dealing with the child’s response when their name was called in an environment with normal background noise was 90% (4.4) indicating that CI children reacted appropriately most of the time. This was not the case in the noisy background where the mean was 57% (3.2) and the scores from both environments were significantly different (U = 277, p < 0.001).
Principal component analysis
To examine inter-item responses from the questionnaire Pearson’s product–moment correlations were calculated from the CI only data. This showed that parental responses to the identification of happy speech were correlated with the recognition of angry (r = 0.74, p < 0.001) and sad (r = 0.71, p < 0.001) speech. The identification of angry and sad speech was also correlated (r = 0.59, p < 0.01). Furthermore, the identification of sad speech was correlated with the identification of narrow focus (r = 0.73, p < 0.001) and questions versus statements (r = 0.58, p < 0.01).
In order to investigate structure in the questionnaire data and yield a reduced number of variables, the correlation matrix was submitted to principal component analysis. Bartlett’s test of sphericity was significant (p < 0.001) and this was a pre-condition for pursuing further analysis. Four factors were found to have eigenvalues (λ) greater than one and these explained 84% of the variance in the data. Examination of the factor scores of the rotated component matrix, shown in
Table 3. Factor scores for the loadings of the rotated component matrix.
Demographic factors
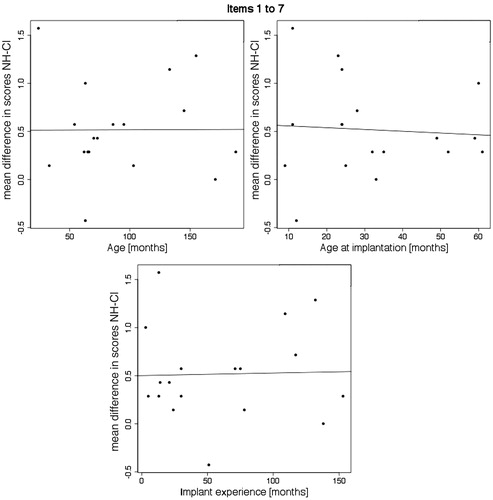
The demographic factors of age, age at implantation and duration of implant experience were examined in relation to the difference scores between NH and CI children for items one to seven. These items were chosen as they involved parental comparison of CI and NH children and also the principal component analysis revealed that the two constructs measured by these items accounted for the majority of the variance in the data. Regression analysis showed that the differences between NH and CI scores decreased as the age at implantation increased, but this was not significant (r = −0.15, p = 0.55). Furthermore, we did not find correlations between NH and CI difference scores and the demographic factors of age (r = −0.01, p = 0.9) or duration of implant experience (r = −0.07, p = 0.76), as displayed in . As the CI group included some adolescents, we examined the same demographic factors after the removal of data from CI01, CI05, CI06, CI09 and CI10, who were all above 10 years of age. However, after the removal of these participants, correlations remained non-significant for age (r = 0.06, p = 0.85), age at implantation (r = 0.003, p = 0.99) and duration of implant experience (r = −0.13, p = 0.67).
Figure 2. Scatterplots and regression line of the difference between NH and CI responses according to age (left panel), age at implantation (right panel) and duration of implant experience (lower panel).
We also examined the demographic variables in relation to the mean scores of items grouped according to the factors derived from the principal component analysis. This did not reveal any correlations that survived post-hoc corrections, but did show an association between the mean ratings for the CI children on factor two and implant experience, which was the length of time that they had been using their implant (r = 0.5, p = 0.03).
In summary, we found significant differences in the parental ratings of prosodic and paralinguistic ability of CI and NH children. Parents reported that they altered their speech when addressing their CI child and situations with a noisy background significantly affected the ability of the CI child to respond when their name was called. Parental ratings of prosodic and paralinguistic abilities of CI children were not related to demographic variables.
Discussion
Our overall aim in comparing parental impressions of CI and NH siblings was to examine the communication competencies of children in everyday situations where fine-grained differences in speech are encountered. We found that parental evaluation of speaker, happy and sad emotion and question/statement identification differed between CI and NH children, while ratings of the identification of anger in speech, the perception of narrow focus and imitation of the intonation of an utterance, did not.
One explanation for why we did not find a significant group difference between the narrow focus and imitation items () is that the consequences of perception of these may have only a minimal bearing on the direction of a typical parent–child dyad. Narrow focus is generally expended on a syllable or a word, and may be accompanied by other actions like gestures or facial expressions. For instance, in the illustrative scenario that accompanied item six, the parent emphasised the colour of the ball that the child was to pick up. Had this occurred in everyday life, the parent may have also pointed at the red ball. Similarly, imitation may occur at the termination of an exchange. The parent may not be attentive to the speech of their CI child, particularly if other children are present and trying to gain the parents’ attention. In contrast to focus and imitation, the aspects of speech communication that we examined in the other items could be expected to have immediate consequences for the parent–child exchange. For instance, a question requires an answer, and speech with strong emotional content would probably be repeated or enhanced if it was misunderstood.
Associations between items
The principal component analysis undertaken in this study showed that the items in our questionnaire could be divided into four separate factors. The first factor consisted of items one to five, which were speaker recognition, emotion identification and imitation. The inclusion of the item that probed imitation, in factor one, must be interpreted in light of the lack of a significant group-wise difference for this item and the low correct item-total correlation value found (see ). Therefore, it is unclear from these results whether a CI child’s ability to recognise speakers and perceive emotion in speech is linked to their ability to imitate intonation in their own speech.
Factor two consisted of items six and seven, which probed the ability of the child to perceive narrow focus and identify questions versus statements. The inclusion of these items in factor two may be due to the prominent role of voice pitch in cueing narrow focus and question/statement contrasts. Factor three consisted of the items that probed parental voice alterations and the child’s response to their name observed in a domestic environment with a noisy background, while the fourth factor included the child’s response to their name in an environment with a normal noise level.
We also found that parents reported that they altered both the vocal effort and the enunciation of their speech when addressing their child with a CI. Results on these two items were highly correlated. This may indicate either that parents that varied one attribute of their speech also varied the other, or that parents may not have been able to reliably distinguish between vocal effort and enunciation alterations in their own speech production.
Demographic factors
The finding that the demographic factors of age, age at implantation and duration of CI experience did not correlate with differences in parental observations between NH and CI children may be explained by a number of reasons. Firstly, the prosodic, paralinguistic and imitation skills investigated by our questionnaire may not have been affected by demographic factors. Secondly, the social and linguistic environment surrounding the child may be more decisive for their language development than demographic factors. Thirdly, parents may be prone to inter-sibling bias that invalidates this type of comparison.
Limitations
The data presented in this study is based on parental responses from CI children who had a younger or an older NH sibling. It would be an advantage if further work that assesses parental impressions of a child’s communication ability could at the same time evaluate the speech perceptual ability of the parents and their sensitivity to variations in the competencies that were being rated. The present study is also limited in that we admitted a range of ages to both the CI and the NH group. However, the mean age difference between CI and NH siblings was only 1 year 1 month. Also, in examining the demographic variables we removed adolescents from the CI group and found that this did not change the overall results. Further qualitative study of the auditory behaviour of CI recipients could focus on the behaviour of infants in the language developmental period just prior to their first year, where prosody aids in word segmentation (Jusczyk, Houston, & Newsome, Citation1999). However, data based on parental impressions of infants may prove unreliable, as Lin et al. (Citation2008) identified a trend whereby parental perceptions of language development were better associated with speech perceptual results in older (4–5 years old) rather than younger children (2–3 years old).
Implications
There is a plethora of validated instruments for investigating parental views on paediatric cochlear implantation and post-implant receptive communication, for instance, see Clark et al. (Citation2011) and Coninx et al. (Citation2009). The questionnaire employed in the present study was not developed as a clinical tool for investigating the effect of device settings on the receptive communication ability of children. Nonetheless, this study suggests that a questionnaire format can be used to investigate prosodic and paralinguistic communication skills.
We found that three of the parents rated the speaker recognition, prosody perception and imitation ability of their CI child to be equal to that of their NH child. This means that these parents considered that their children derived real-world benefit from their CI, so that their communication ability involving nuanced perceptual tasks was commensurate with that of their NH child. This suggests that there are some paediatric CI recipients who do extremely well with their implant. However, group-wise comparisons of the parental impressions revealed that there were significant differences between CI and NH children. Parental ratings of the ability of CI children to respond when their name was called were affected by the noise level in the domestic environment. The detrimental effect of noise on recognition may be expected to influence listening in other situations. Therefore, these findings are relevant to the acoustic properties of educational facilities and they support the position that signal-noise improvements should be optimised for CI listeners. They are also relevant to the pre-operative counselling of parents of paediatric CI candidates who should be alerted to the possible negative consequences of cochlear implantation. The overall finding that CI children are not deemed by their parents as being as competent in prosody perception, indicates that facilitating improvements in these perceptual domains should be pursued in device development and rehabilitation.
Conclusions
The parental observations recorded in this study indicate that in comparison to their NH siblings, CI children have difficulty in some aspects of prosodic and paralinguistic perception. They also show that parents are aware of the perceptual deficit experienced by their CI child and that they alter their speech to compensate for this. Parents also reported that noisy environments had a strong adverse affect on the ability of CI children to respond when their name was called. Demographic variables were not found to be linked to the parental reports of listening ability.
Acknowledgements
The authors would like to thank the staff members of the Konkylien integrated daycare institution for their advice on data collection.
Declarations of interest
No outside funding or grants in support of this work were received. The authors report no conflicts of interest and are alone responsible for the content and the writing of this paper.
References
- Bergeson, T. R., Miller, R. J., & McCune, K. (2006). Mothers’ speech to hearing-impaired infants and children with cochlear implants. Infancy, 10, 221–240
- Bohn, O.-S. (2013). Acoustic characteristics of Danish infant directed speech. Proceedings of Meetings on Acoustics, 19, 1–7
- Boons, T., Brokx, J. P. L., Dhooge, I., Frijns, J. H. M., Peeraer, L., Vermeulen, A., Wouters, J., van Wieringen, A. (2012). Predictors of spoken language development following pediatric cochlear implantation. Ear and Hearing, 33, 617–639
- Calderon, R. (2000). Parental involvement in deaf children’s education programs as a predictor of child’s language, early reading, and social-emotional development. Journal of Deaf Studies and Deaf Education, 5, 140–155
- Ching, T. Y. C., & Hill, M. (2007). The Parents’ Evaluation of Aural/Oral Performance of Children (PEACH) Scale: Normative data. Journal of the American Academy of Audiology, 18, 220–235
- Ching, T. Y. C., Hill, M., & Dillon, H. (2008). Effect of variations in hearing-aid frequency response on real-life functional performance of children with severe or profound hearing loss. International Journal of Audiology, 47, 461–475
- Clark, J. H., Aggarwal, P., Wang, N. Y., Robinson, R., Niparko, J. K., & Lin, F. R. (2011). Measuring communicative performance with the FAPCI instrument: Preliminary results from normal hearing and cochlear implanted children. International Journal of Pediatric Otorhinolaryngology, 75, 549–553
- Coninx, F., Weichbold, V., Tsiakpini, L., Autrique, E., Bescond, G., Tamas, L., Compernol, A., Georgescu, M., Koroleva, I., Le Maner-Idrissi, G., Liang, W., Madell, J., Mikic, B., Obrycka, A., Pankowska, A., Pascu, A., Popescu, R., Radulescu, L., Rauhamäki, T., Rouev, P., Kabatova, Z., Spitzer, J., Thodi, Ch., Varzic, F., Vischer, M., Wang, L., Zavala, J.S., & Brachmaier, J. (2009). Validation of the LittlEARS((R)) Auditory Questionnaire in children with normal hearing. International Journal of Pediatric Otorhinolaryngology, 73, 1761–1768
- Crocker, L. M., & Algina, J. (1986). Introduction to classical and modern test theory, New York: Holt, Rinehart, and Winston
- Ekman, P., Sorenson, E. R., & Friesen, W. V. (1969). Pan-cultural elements in facial displays of emotion. Science, 164, 86–88
- Fujiki, M., Spackman, M. P., Brinton, B., & Illig, T. (2006). Ability of children with language impairment to understand emotion conveyed by prosody in a narrative passage. International Journal of Language Communication Disorders, 43, 330–345
- Jusczyk, P. W., Houston, D. M., & Newsome, M. (1999). The beginnings of word segmentation in English-learning infants. Cognitive Psychology, 39, 159–207
- Lin, F. R., Wang, N.-Y., Fink, N. E., Quittner, A. L., Eisenberg, L. S., Tobey, E. A., Niparko, J. K. (2008). Assessing the use of speech and language measures in relation to parental perceptions of development after early cochlear implantation. Otology & Neurotology, 29, 208–213
- Lyxell, B., Wass, M., Sahlén, B., Samuelsson, C., Asker-Árnason, L., Ibertsson, T., Mäki-Torkko, E., Larsby, B., Hällgren, M. (2009). Cognitive development, reading and prosodic skills in children with cochlear implants. Scandinavian Journal of Psychology 50, 463–474
- Moeller, M. P. (2000). Early intervention and language development in children who are deaf and hard of hearing. Pediatrics, 106, 43–43
- Moore, B. C. J. (2003). Coding of sounds in the auditory system and its relevance to signal processing and coding in cochlear implants. Otology & Neurotology, 24, 243–254
- Nienhuys, T. G., Cross, T. G., & Horsborough, K. M. (1984). Child variables influencing maternal speech style. Deaf and hearing children. Journal of Communication Disorders, 17, 189–207
- O’Halpin, R. (2010). The perception and production of stress and intonation by children with cochlear implants (Dissertation). University College London, London
- Peng, S.-C., Tomblin, J. B., & Turner, C. W. (2008). Production and perception of speech intonation in pediatric cochlear implant recipients and individuals with normal hearing. Ear and Hearing, 29, 336–351
- Purdy, S. C., Farrington, D. R., Moran, C. A., Chard, L. L., & Hodgson, S.-A. (2002). A parental questionnaire to evaluate children’s Auditory Behavior in Everyday Life (ABEL). American Journal of Audiology, 11, 72–82
- Szagun, G., & Stumper, B. (2012). Age or experience? The influence of age at implantation and social and linguistic environment on language development in children with cochlear implants. Journal of Speech, Language, and Hearing Research, 55, 1640–1654
- Wiefferink, C. H., Rieffe, C., Ketelaar, L., & Frijns, J. H. M. (2012). Predicting social functioning in children with a cochlear implant and in normal-hearing children: The role of emotion regulation. International Journal of Pediatric Otorhinolaryngology, 76, 883–889
Appendix
Translation of the questionnaire from Danish.
Responses to questions 1–7 are to be given on the scale below. Parents are requested to tick only one box for each child.
1. This question is about the recognition of voices. How often does your CI and NH children recognise a familiar voice when they cannot see who is talking?
An example may be that a family member enters your house and calls out to the child who is in another room.
________________________________
The next 3 questions deal with ability to discern an emotional state from a voice. Indicate the extent to which you think your CI and NH children can hear from your voice if you are:
2. happy
3. angry
4. sad
_______________________________
5. This question is about imitation. Indicate the extent to which your CI and NH children mimic the way you say things when they imitate or repeat something you say.
For example, you may say to them, “can you say ‘slide’?” pronounced with a happy and lively intonation.
_________________________________
6. This question is about emphasis as clarification of a word. Imagine that you are playing with different coloured balls. You ask the child to get the red ball, but your child reaches for the blue ball. You say “No, not the blue ball. The RED ball”. Indicate the extent to which you think your CI and your NH child understands, from the emphasis that you placed on the word, that it is the red ball that you would like.
_____________________________
7. This question is about your children’s ability to understand when a question has been asked. Assess the extent to which your CI and NH children understand when you ask them a question. By this we mean if they know that a question has been posed and that it requires some kind of response.
_____________________________
Responses to questions 8 and 9 were given on the scale below.
The next two questions are about the vocal effort (volume) and clarity of your speech.
8. This question concerns differences in the vocal effort of your speech when you speak to your children. Assess whether there is a difference in the strength of your voice when you address your CI and your NH child.
____________________________
9. This question concerns differences in enunciation when you speak to your children. Assess whether there is a difference in clarity when you address your CI and your NH child.
__________________________
Responses to questions 10 and 11 were given on the scale below.
The next two questions are about noisy and quiet situations that you may encounter at home in the course of everyday life.
10. Imagine a noisy situation at home where your CI child cannot see you. Noise sources could include siblings, the television, a hair dryer, etc. Assess how often your CI child would react when you call their name.
A reaction could include looking up, turning to the sound, or a verbal response.
______________________
11. Imagine a situation at home, where there is a normal level of noise and your child cannot see you. Noise sources could include siblings, the television, a hair dryer, etc. Assess how often your CI child would react when you call their name.
A reaction could include looking up, turning to the sound, or a verbal response.