Case reports
Case number 1
A 34-year-old female, presenting with an enlarged node at the neck, was diagnosed with a nodular sclerosis Hodgkin lymphoma in April 2007. The staging included a computed tomography (CT) scan of the neck, thorax and abdomen, bone marrow biopsy from the iliac crest and standard laboratory values. Enlarged lymph nodes, 2–3 cm in diameter, were observed at both sides of the neck and in the upper mediastinum. Laboratory values were normal with the exception of an elevated sedimentation rate of 67 mm/h. The bone-marrow biopsy did not show any signs of lymphoma. The patient was free from symptoms except for a slight itching and a low-grade lumbar back-pain during the previous two months. The patient was considered to be in stage IIA, with two risk factors (more than two engaged lymph node stations and a sedimentation rate of >50 mm/h). Treatment was initiated with ABVD (doxorubicin, bleomycin, vinblastine and dacarbazine). Granulocyte-colony stimulating factor (G-CSF) was not given with the ABVD schedule. The patient’s symptoms disappeared immediately after initiation of treatment. After four courses of ABVD, an F-18-fluoro-deoxy-glucose positron emission tomography/computed tomography (FDG-PET/CT) scan was performed, and showed no uptake at the initial lymphoma manifestations, thus considered as complete remission (CR). Consolidating radiotherapy 1.75 Gy/fraction to 30 Gy was planned for the initially enlarged lymph nodes.
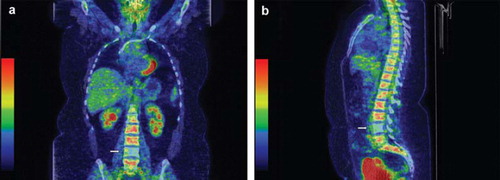
However, during the planning of radiotherapy, it was observed that the fourth lumbar vertebra (L IV) lacked normal glucose uptake at the FDG-PET/CT scan ( (coronal) and (sagittal)). The CT scan of the abdomen, at the time of diagnosis, was carefully re-examined and increased sclerosis was identified in L IV, consistent with Hodgkin lymphoma involvement. This finding was clinically supported by the fact that the patients back-pain resolved subsequent to the first course of therapy. The initial stage was changed from stage II to stage IV and the planned radiotherapy was omitted. Instead treatment was escalated to full dose chemotherapy, according to recommendations for advanced stages. After termination of treatment the patient was evaluated with CT and two times with magnetic resonance imaging (MRI) of the spine and was considered to be in CR at follow-up CT 12 months after termination of treatment. The MRI-examinations at treatment termination and two months later did not show signs of other possible causes of cold spots, such as hemangioma, tuberculous abscess or metastasis. However, on these examinations there was an increasing fat content in L IV, which is a sign of treatment response [Citation1]. The patient remains in CR 26 months after cessation of treatment.
Figure 1. a. FDG-PET/CT (coronal section) showing lack of normal FDG-uptake in L IV in a patient with Hodgkin lymphoma after four courses of ABVD, indicating previous lymphoma involvement. b. Sagittal section from the same examination.
Case number 2
As a further illustration of this phenomenon we describe a 58-year-old man who presented with weight loss, night sweats, abdominal discomfort and fatigue. He was staged using CT of the neck, thorax and abdomen. Enlarged lymph nodes were found in the mediastinum, axillae, retroperitoneum and intraabdominally. The spleen was enlarged. A biopsy specimen was obtained from one of the abdominal nodes and showed lymphocyte depleted Hodgkin lymphoma, an extremely rare subtype. The diagnosis was made by an experienced haematopathologist. A bone-marrow biopsy from the iliac crest showed Hodgkin lymphoma involvement. The patient was in stage IVB. He had five risk factors (male, age >45, stage IV, B-Haemoglobin <105 g/l, S-Albumin <40 g/l), according to the international prognostic score [Citation2]. Treatment with BEACOPP-14 (Bleomycin, Etoposide, Doxorubicin, Cyclophosphamide, Vincristine, Procarbazine, Prednisone, given every 14 days supported with G-CSF) was initiated.
After two chemotherapy courses an FDG-PET/CT scan was performed. It showed complete metabolic remission. In the bone marrow there was an increased FDG uptake, as expected, due to G-CSF. However, in one thoracic vertebra (ThI) there was a complete lack of FDG-uptake indicating an earlier lymphoma involvement (). The patient had also focal reductions of elevated uptake in other vertebrae. These findings were more obvious than in case one, due to the activation of the normal bone-marrow secondary to G-CSF treatment. This finding did not change the planned treatment with full chemotherapy, since the staging was not altered due to the unchanged stage. A total of six courses were given. The patient is still in CR 20 months after cessation of treatment.
Figure 2. FDG-PET/CT showing lack of normal FDG-uptake in Th I in a patient with Hodgkin lymphoma after two courses of BEACOPP-14, indicating previous lymphoma involvement.

Discussion
FDG-PET/CT scan is a valuable tool in staging and remission evaluation in patients with Hodgkin lymphoma. In addition, it seems to provide important prognostic information when performed early in the treatment [Citation3–6]. In remission evaluation, the new response criteria recommend PET to patients with residual tumours and if negative the patient is considered to be in CR [Citation4,Citation7].
When evaluating treatment response with PET it is optimal to perform an FDG-PET/CT before the start of treatment. FDG-PET/CT evidently detects lymphoma involvement better than standard procedures, and it is easier to evaluate response having a base-line investigation. In a Danish study, FDG-PET would have upstaged 19%, downstaged 5% of patients, leading to different treatment in 9%, as compared to CT [Citation8]. In an Italian study, CT and FDG-PET stages were concordant in 156 patients (84%) and discordant in 30 patients (16%). Fourteen percent were upstaged and 1% downstaged [Citation9]. For practical and economical reasons, however, an FDG-PET/CT before treatment is not always possible.
We have, with the first case history, showed that important unsuspected staging information can be obtained by the treatment evaluation PET scan. The second case illustrates that such a finding is not unique. In both cases, the previous lymphoma involvement was revealed by cold areas in the bone-marrow. Also, an FDG-PET scan as well as an MRI at diagnosis would have revealed the bone involvement in these cases. The first patient had symptoms of back-pain. The pain was, however, so diffuse that the clinician did not suspect bone involvement and did not order an MRI, which is not a routine investigation in the staging of Hodgkin lymphoma. This case illustrates that this kind of finding can contribute greatly to the decision of treatment strategy, as the patient received full chemotherapy instead of a short course of chemotherapy followed by radiotherapy. In the second case, the finding did not change the treatment regime. Cold areas after chemotherapy, where HL involvement was present before treatment, have previously been described; however in that case, the involvement had already been demonstrated on a PET before therapy [Citation10]. The finding was more obvious in case 2, due to G-CSF activation of the bone-marrow, although it was still noticed in case 1.
These cases illustrate that it may be worthwhile to also examine for cold areas in the bone-marrow which normally should have activity, when evaluating PET-scans during therapy. In the absence of a staging FDG-PET before treatment, the evaluation PET can “salvage” a suboptimal staging procedure.
Declaration of interest: The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
- Lien HH, Holte H. Fat replacement of Hodgkin disease of bone marrow after chemotherapy: Report of three cases. Skeletal Radiol 1996;25:671–4.
- Hasenclever D, Diehl V. A prognostic score for advanced Hodgkin’s disease. International Prognostic Factors Project On Advanced Hodgkin’s Disease. N Engl J Med 1998: 339:1506–14.
- Gallamini A, Hutchings M, Rigacci L, Specht L, Merli F, Hansen M, . Early interim 2-[18F]fluoro-2-deoxy-D-glucose positron emission tomography is prognostically superior to international prognostic score in advanced-stage Hodgkin’s lymphoma: A report from a joint Italian-Danish study. J Clin Oncol 2007;25:3746–52.
- Brepoels L, Stroobants S, De Wever W, Spaepen K, Vandenberghe P, Thomas J, . Hodgkin lymphoma: Response assessment by revised International Workshop Criteria. Leuk Lymphoma 2007;48:1539–47.
- Bjurberg M, Gustavsson A, Ohlsson T, Brun E. FDG-PET in the detection of residual disease and relapse in patients with Hodgkin’s lymphoma. Experience from a Swedish centre. Acta Oncol 2006;45:743–9.
- Hutchings M, Loft A, Hansen M, Pedersen LM, Buhl T, Jurlander J, . FDG-PET after two cycles of chemotherapy predicts treatment failure and progression-free survival in Hodgkin lymphoma. Blood 2006;107:52–9.
- Cheson BD, Pfistner B, Juweid ME, Gascoyne RD, Specht L, Horning SJ, . Revised response criteria for malignant lymphoma. J Clin Oncol 2007;25:579–86.
- Hutchings M, Loft A, Hansen M, Pedersen LM, Berthelsen AK, Keiding S, . Position emission tomography with or without computed tomography in the primary staging of Hodgkin’s lymphoma. Haematologica 2006;91:482–9.
- Rigacci L, Vitolo U, Nassi L, Merli F, Gallamini A, Pregno P, . Positron emission tomography in the staging of patients with Hodgkin’s lymphoma. A prospective multicentric study by the Intergruppo Italiano Linfomi. Ann Hematol 2007;86:897–903.
- Kazama T, Faria SC, Varavithya V. FDG PET in the evaluation of treatment for lymphoma: Clinical usefulness and pitfalls. Radiographics 2005;25:191–207.