To the Editor,
The patient, a 55-year-old man, consulted his general practitioner for an annual health control in 2007. At diagnosis serum prostate specific antigen (PSA) level was 109 ng/ml. The tumor was regarded as non-organ confined by digital rectal examination (cT3A). Further investigation with transrectal ultrasound-based biopsies confirmed the prostate cancer (PCa) histologically (Gleason score 7B). The patient was referred to pelvic lymph node dissection showing lymphatic spread in one of 10 removed lymph nodes (pN1). Further staging procedures were continued according national and international recommendations, including magnetic resonance imaging (MRI), chest x-ray and bone scan [Citation1]. The disease was staged as T3apN1M0 (TNM-UICC 2010). As part of an inhouse protocol bone marrow and blood samples were drawn. Applying standardized immunocytostaining methods (CellSearch®) no isolated tumor cells were found in these samples.
Treatment
Neoadjuvant androgen deprivation treatment (ADT) with a GnRH-agonist (goserelin) was started during the first six months combined with three-dimensional computed tomography (3D-CT) planned conformal radiotherapy (RAD) encompassing the prostate and vesiculae seminales (74 Gy, 2 Gy per fraction, five days per week) and image modulated radiotherapy to the whole pelvis (50 Gy, 2 Gy per fraction) was performed.
Follow-up
Six months after initiation of ADT therapy PSA decreased from baseline 109 to 1.1 ng/ml and after the course of radiotherapy PSA declined to 0.6 ng/ml. Apart from the loss of potency, the patient had minor acute side effects of combined therapy. At one year follow-up a planned extended examination, including MRI, revealed no evidence of disease. The MRI showed substantial fibrosis of the irradiated prostate and nearby structures. Radiologically there was additional sign of fibrosis to the lymph nodes and pelvis bone marrow was replaced with fat tissue. Serum PSA was still low at 0.4 ng/ml. The patient reported normal voiding and no mucous or bloody rectal discharge. He did not regain potency.
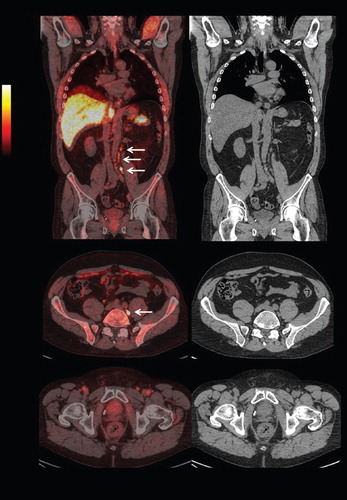
After two years on GnRH-agonist therapy PSA raised to 2.4 ng/ml, however, clinically the patient was asymptomatic. A rigorous staging was performed according to the protocol, including bone marrow samples, MRI, and bone scan. None of the investigations could locate the recurrence. In view of the patient's age a localized relapse could open for a salvage therapy, therefore we performed 18F-FDG positron emission tomography (PET)/CT, so far the only institutionally available radiotracer in Norway. This method could not find the cause of the ongoing PSA rising. The patient was referred to a private institute performing anti-1-amino-3-18F-fluorocyclobutane-1-carboxylic acid (FACBC) PET/CT (). FACBC is a synthetic amino acid analog, its uptake is mediated through amino acid transport proteins, and the radiotracers are not metabolized [Citation2]. FACBC-based PET/CT detected pathological uptake in lymph nodes of 9 mm and 3 mm in axial size situated at the paraaortic drainage and inside a lymph node dorsal to the left common iliaca vein, 13 mm at the largest diameter.
Figure 1. Positron emission tomography / computed tomography (PET / CT) diagnostic images (arrow ¬ showing FACBC-uptake in paraaortic lymph nodes).
Discussion
The preferred treatment of patients with pN1 disease is controversial. In line with the published results in patients with locally advanced PCa (pN1) [Citation3], we tried a multimodal approach combining RAD and ADT. Unfortunately, the patient had PSA rising two years after RAD. In view of his young age, a localization of the relapse was warranted for tailoring subsequent therapy, especially the use of salvage techniques. Modern image techniques, such as multiparametric MRI and PET/CT could be valuable tools in these circumstances. However, despite of the rigorous approach used in this case neither MRI nor 18F-FDG-PET was able to locate the relapse in our patient. No metastases were seen. In addition, promising tracers investigated for patients with relapsing PCa, for instance choline or acetate, are not accessible in Norway. In this situation, we decided to test FACBC.
FACBC- PET/CT showed convincingly uptake in several lymph nodes located outside the previous radiation field but following the drainage of lymph from the left pelvis. Interestingly, the patient had a histologically positive lymph node nearby the left iliaca interna vein. In a recently published study, Schuster and colleagues showed that FACBC had excellent concordance with pelvic node findings with clinical follow-up [Citation4].
In summary, promising new isotopes, such as FABC can be suitable for the detection of recurrence in patients with PCa. These methods will avoid unnecessarily at random performed biopsies and undoubted increase the sensitivity of the investigation. FACBC is such a novel radiotracer as shown in our patient and should be studied in a larger cohort.
Declaration of interest: The authors report no conflicts of interest. The authors alone are responsible for the content and writing of this paper.
References
- Heidenreich A, Aus G, Bolla M, Joniau S, Matveev VB, Schmid HP, . EAU guideline on prostate cancer. Eur Urol 2008;53:68–80.
- Martarello L, McConathy J, Camp VM, Malveaux EJ, Simpson NE, Simpson CP, . Synthesis of syn- and anti-1-amino-3-[18F]fluoromethyl-cyclobutane-1-carboxylic acid (FMACBC), potential PET ligands for tumor detection. J Med Chem 2002;45:2250–9.
- Messing EM, Manola J, Sarosdy M, Wilding G, Crawford ED, Trump D. Immediate hormonal therapy compared with observation after radical prostatectomy and pelvic lymphadenectomy in men with node-positive prostate cancer. N Engl J Med 1999;341:1781–8.
- Schuster DM, Votaw JR, Nieh PT, Yu W, Nye JA, Master V, . Initial experience with the radiotracer anti-1-amino-3-18F-fluorocyclobutane-1-carboxylic acid with PET/CT in prostate carcinoma. J Nucl Med 2007;48:56–63.