To the Editor,
A 65-year-old woman who had never smoked presented with hemoptysis in December 2010. Chest x-ray showed massive right pleural effusion and pleural fluid cytology demonstrated metastatic non-small cell carcinoma. Bronchoscopy revealed a tumor occluding the right lower lobe bronchus and a transbronchial lung biopsy confirmed adenocarcinoma with positive immunohistochemical staining for thyroid transcription factor 1 (TTF-1) and cytokeratin 7 (CK7) (). Epidermal Growth Factor Receptor (EGFR) mutation analysis using Sanger sequencing identified a single point mutation L858R in exon 21 of the EGFR gene. Staging positron emission tomography-computed tomography (PET/CT) fusion scan showed a primary right lower lobe tumor, right pleural deposits and multiple lymphadenopathy in the mediastinum, bilateral supraclavicular fossae, left axilla and para-aortic region (). The patient was treated with gefitinib for six weeks, which led to a mixed response with clinical resolution of supraclavicular and left axillary lymph nodes but increased right pleural effusion. A pleural biopsy was thus performed. Examination of the biopsy specimen revealed a synaptophysin-positive small-cell neuroendocrine carcinoma (), which harbored the same EGFR exon 21 mutation L858R that was detected in the previous lung biopsy of adenocarcinoma. Based on the histological diagnosis of small cell lung cancer (SCLC), patient then received three cycles of etoposide and cisplatin. She achieved a near complete response with resolved right pleural effusion and only a small residual right lower lobe lesion ().
Figure 1. A. Lung biopsy showing adenocarcinoma. Hematoxylin and eosin stain; B. Pleural biopsy showing SCLC. Hematoxylin and eosin stain; C. Synaptophysin staining of the pleural biopsy specimen.
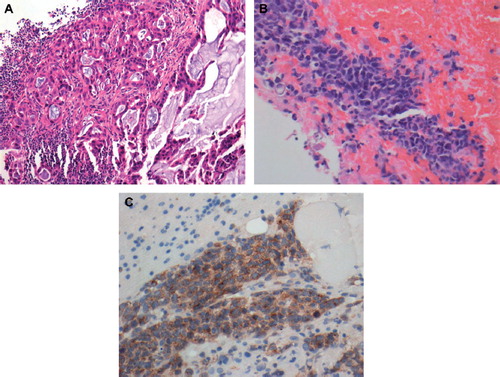
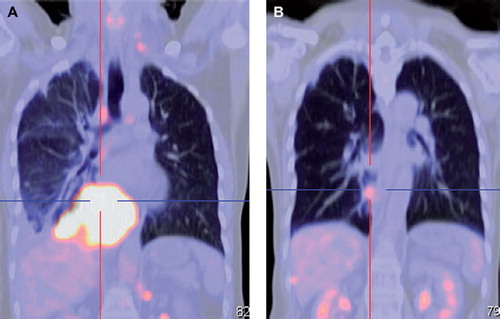
Figure 2. A. Coronal view of PET/CT at diagnosis showed a hypermetabolic mass in the right lower lobe; B. Significant improvement in the right lower lobe mass after chemotherapy.
Activating mutation in the EGFR gene is extremely rare in SCLC and is not predictive of response to tyrosine kinase inhibitor (TKI) of EGFR, in contrast to non-small cell lung cancer (NSCLC) [Citation1,Citation2]. Isolated case reports have described patients with EGFR-mutant SCLC, of which the majority are never-smoking females with either combined SCLC and adenocarcinoma at initial presentation or sequential diagnosis of adenocarcinoma followed by SCLC [Citation1–7]. Our patient is similar to four previous reports in which SCLC developed after being treated with EGFR TKIs for primary lung adenocarcinoma. Interesting, both SCLC and NSCLC tissues shared the same EGFR mutation, supporting the existence of a pluripotent population of EGFR-mutant cancer cells that are the source of EGFR TKI resistance [Citation1,Citation4,Citation5,Citation7]. Sequist et al. performed genetic and histological analyses of tumor biopsies from 37 patients with EGFR TKIs-resistant NSCLC carrying EGFR mutations and identified five cases of phenotypic transformation to SCLC, of which the original EGFR mutation was maintained [Citation8]. All the patients achieved a period of disease stabilization with EGFR TKI before developing drug resistance with the transition from NSCLC to SCLC. Morinaga et al. also described a case of SCLC with an EGFR mutation developing after prolonged treatment for primary adenocarcinoma of the lung [Citation5]. The same exon 19 deletion of EGFR was present in both the original lung adenocarcinoma and the metastatic SCLC. Although our patient had progression of disease at six weeks of gefitinib therapy, the evidence of response to treatment in certain disease regions suggests at least a partial effect of EGFR TKI in eliminating the EGFR mutant NSCLC clones. This is consistent with the hypothesis that two different clones of lung adenocarcinoma and small cell carcinoma coexist at the time of initial diagnosis. It is still unclear whether the adenocarcinoma may have transdifferentiated to small cell carcinoma, given the sequential development of SCLC after NSCLC in some cases. Furthermore, repeat biopsies at the time of clinical resistance to EGFR inhibition is important in diagnosing a clonally-related recurrence with SCLC and directly affects treatment decisions and outcomes.
References
- Tatematsu A, Shimizu J, Murakami Y, Horio Y, Nakamura S, Hida T, . Epidermal growth factor receptor mutations in small cell lung cancer. Clin Cancer Res 2008;14:6092–6.
- Shiae TH, Chang YL, Yu CH, Chang YC, Hsu YC, Chang SH, . Epidermal growth factor receptor mutations in small cell lung cancer: A brief report. J Thorac Oncol 2011;6:195–8.
- Okamoto I, Araki J, Suto R, Shimada M, Nakagawa K, Fukuoka M. EGFR mutation in gefitinib-responsive small-cell lung cancer. Ann Oncol 2006;17:1028–9.
- Zakowski MF, Ladanyi M, Kris MG. Memorial Sloan-Kettering Cancer Center Lung Cancer OncoGenome Group. EGFR mutations in small-cell lung cancers in patients who have never smoked. N Engl J Med 2006; 355:213–5.
- Morinaga R, Okamoto I, Furuta K, Kawano Y, Sekijima M, Dote K, . Sequential occurrence of non-small cell and small cell lung cancer with the same EGFR mutation. Lung Cancer 2007;58:411–3.
- Fukui T, Tsuta K, Furuta K, Watanabe SI, Asamura H, Ohe Y, . Epidermal growth factor receptor mutation status and clinicopathological features of combined small cell carcinoma with adenocarcinoma of the lung. Cancer Sci 2007;98:1714–9.
- Alam N, Gustafson KS, Ladanyi M, Zakowski MF, Kapoor A, Truskinovsky AM, . Small-cell carcinoma with an epidermal growth factor receptor mutation in a never-smoker with gefitinib-responsive adenocarcinoma of the lung. Clin Lung Cancer 2010;11:E1–4.
- Sequist LV, Waltman BA, Dias-Santagata D, Digumarthy S, Turke AB, Fidias P, . Genotypic and histological evolution of lung cancers acquiring resistance to egfr inhibitors. Sci Transl Med 2011;3:75ra26.