To the Editor,
Glivec (STI 571), an inhibitor of bcr-abl tyrosine kinase, has become a first line agent in the treatment of Ph+ chronic myeloid leukemia (CML) and metastatic gastrointestinal stromal tumors [Citation1]. Activation of tyrosine kinases leads to phosphorylation of key substrates within the cell [Citation2].
Tyrosine kinase inhibitors compete with ATP for binding to the ATP binding site found on all tyrosine kinases [Citation3]. Such action occurs not only in cancer cells but also in normal cells and causes adverse effects including fluid retention, edema, nausea, vomiting, diarrhea, fatigue, and some skin disorders [Citation4,Citation5]. Pancytopenia has also been reported as an adverse effect, though its mechanism is not known [Citation6]. Vocal fold hemorrhage may be caused by laryngeal trauma, phonotrauma, aspirin and non-steroid anti-inflammatories, and hormonal imbalance [Citation7]. There have been reports associating vocal fold hemorrhage with factor VIII deficiency, tenecteplase thrombolysis, and others; however, no cases have been reported of vocal fold hemorrhage occurring after the use of Glivec. Along with a literature review, we report a case in which we treated vocal fold hemorrhage discovered by laryngendoscopy in a patient who had been diagnosed with CML and had received Glivec treatment.
Case report
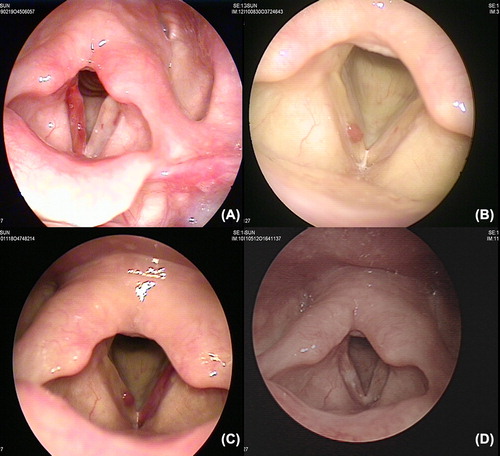
A 61-year-old woman visited the Department of Otolaryngology at our hospital in February 2009 complaining of a change in her voice and throat discomfort that had been occurring for two years prior to her visit. This patient had been on Glivec 400 mg/day for the treatment of CML for the past six years. The patient reported that her symptoms occurred each day shortly after taking the Glivec. Laryngendoscopy was performed and a hemorrhagic tendency was observed in the entire right vocal cord (). Conservative treatment was initially given, followed by regular follow-up observations. Discomfort in the throat disappeared. The patient came to the hospital again in August 2010 presenting with the same symptoms: a change in her voice and throat discomfort. Physical examination revealed a hemorrhagic polyp in the right vocal fold at the 1/3 anterior site but without any other remarkable manifestations (). The patient was given conservative treatment similar to before, with concomitant voice therapy. Three months after the beginning of the voice treatment, laryngendoscopy showed new diffuse ecchymosis in the left vocal fold and no improvement of the hemorrhagic polyp in the right vocal fold (). The change in voice and throat discomfort continued, and the patient was admitted to the hospital. Following tests, the Hemato-Oncology Department advised that the vocal fold hemorrhage was a pancytopenia induced by the prolonged use of a drug, and suspected an adverse effect from Glivec. Gastroscopy was then performed to rule out possible hemorrhage in the digestive tract, but no remarkable manifestations were observed, nor did a fecal examination find any traces of hemorrhage. It was decided to continue conservative treatment unless the patient's condition deteriorated. Follow-up observations over the next five months confirmed there had been no improvement of the lesion, therefore polypectomy was performed using laryngomicrosurgery, along with ablation of the feeding vessels using a CO2 laser. No recurrence of hemorrhage occurred for one year postoperatively (), and the patient is currently on observation as an outpatient.
Figure 1. Endoscopic image of the vocal folds. A) Diffuse hemorrhage is shown in the right vocal fold. B) A hemorrhagic polyp is shown in the right vocal fold. C) A hemorrhagic polyp in the right vocal fold and diffuse ecchymosis in the left vocal fold are shown. D) Healthy vocal folds are shown after laryngomicrosurgery and CO2 laser ablation.
Discussion
Glivec (imatinib, STI 571) is a chronic CML treatment first approved by FDA in May 2001 [Citation8]. Its hematologic side effects include anemia, neutropenia, and thrombocytopenia, and non-hematologic effects include hypertension, thrombosis, embolism, myocardial infarction, skin rash, edema, neuropathy and bleeding, although the exact mechanisms of such effects are unknown [Citation1].
Vascular lesions of the vocal fold occur due to dilatation or rupture of the blood vessels along the vocal fold mucosa and are characterized by a wide variety of symptoms [Citation9]. Symptoms for vascular lesions of the vocal fold include, among others, vocal fatigue, decreased vocal range, and dysphonia.
Among the cases of drug-induced hemorrhage in the vocal folds, those associated with the use of anticoagulants have often been reported. Sima et al. reported a case of a hemorrhagic polyp in the vocal fold that occurred after the use of tenecteplase and was cured after one month of conservative management without complications [Citation10]. Jeffrey et al. reported a case in which an opera singer, who suffered vocal fold hemorrhage after the use of Coumadin, received a microlaryngoscopic removal of the vocal fold polyp and CO2 laser ablation of the feeding vessels to the polyp [Citation7].
This is the first reported case, however, for treatment of vocal fold hemorrhage induced by Glivec, a CML drug. In our case, the patient did not require the use of her voice to a large extent in her profession, nor did she describe herself as a person who frequently talked or shouted. She also reported having had no traumatic experience. As she reported that her voice change and throat discomfort occurred only after intake of Glivec, we suspected a drug- induced effect. In the current case, conservative treatment and vocal therapy were given initially because the patient presented only with a hemorrhagic polyp in the right vocal fold upon arrival, but the condition did not improve and further hemorrhage was discovered in the left vocal fold. Microlaryngoscopic removal of the vocal fold polyp using a cold instrument and CO2 laser ablation of the feeding vessels to the polyp were then performed, and the condition was completely cured. No manifestation of hemorrhage recurrence could be observed for one year postoperatively, and the patient is currently in follow-up observations.
We suggest that surgical treatment be considered when vocal fold hemorrhage does not respond to conservative treatment. If the hemorrhage is an adverse effect of medication, use of the associated drug must be discontinued. Careful observation in regards to hemorrhagic tendency must be considered when administering Glivec in the treatment of CML. In conclusion, when treating CML patients with Glivec, it will be helpful to take into account the possibility of hemorrhage in the vocal fold or gastrointestinal tract.
Declaration of interest: The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
- Hartmann JT, Haap M, Kopp HG, Lipp HP. Tyrosine kinase inhibitors – a review on pharmacology, metabolism and side effects. Curr Drug Metab 2009;10:470–81.
- Orphanos GS, Ioannidis GN, Ardavanis AG. Cardiotoxicity induced by tyrosine kinase inhibitors. Acta Oncol 2009;48: 964–70.
- van Erp NP, Gelderblom H, Guchelaar HJ. Clinical pharmacokinetics of tyrosine kinase inhibitors. Cancer Treat Rev 2009;35:692–706.
- De Arriba JJ, Nerin C, Garcia E, Gomez-Aldaravi L, Vila B. Severe hemolytic anemia and skin reaction in a patient treated with imatinib. Ann Oncol 2003;14:962.
- van Oosterom AT, Judson I, Verweij J, Stroobants S, Donato di Paola E, Dimitrijevic S, et al. Safety and efficacy of imatinib (STI571) in metastatic gastrointestinal stromal tumours: A phase I study. Lancet 2001;358:1421–3.
- Miyazawa K, Nishimaki J, Katagiri T, Sashida G, Shoji N, Kawakubo K, et al. Thrombocytopenia induced by imatinib mesylate (Glivec) in patients with chronic myelogenous leukemia: Is 400 mg daily of imatinib mesylate an optimal starting dose for Japanese patients?Int J Hematol 2003;77: 93–5.
- Neely JL, Rosen C. Vocal fold hemorrhage associated with coumadin therapy in an opera singer. J Voice 2000;14: 272–7.
- Sawyers CL, Hochhaus A, Feldman E, Goldman JM, Miller CB, Ottmann OG, et al. Imatinib induces hematologic and cytogenetic responses in patients with chronic myelogenous leukemia in myeloid blast crisis: Results of a phase II study. Blood 2002;99:3530–9.
- Postma GN, Courey MS, Ossoff RH. Microvascular lesions of the true vocal fold. Ann Otol Rhinol Laryngol 1998;107: 472–6.
- Samimi-Fard S, Garcia-Gonzalez M, Dominguez-Rodriguez A. Vocal cord haematoma after tenecteplase thrombolysis. Acta Otolaryngol 2006;126:884–5.