
Dear Editor,
Large international differences in colorectal cancer survival are known to exist and attempts have been made to investigate the extent to which stage at diagnosis explains these differences [Citation1]. It is well documented that making useful international comparisons based on stage at diagnosis is fraught with difficulties, in particular with regards to the standardisation of staging data [Citation2]. The recently published study by Maringe et al. [Citation3] takes staging data between countries that use a variety of staging systems (TNM, Dukes’, SEER and locally SEER-based) and translate this data into one unified classification. Despite the obvious limitations of this methodology the authors have principally misinterpreted the origins and composition of the data used in their analysis. As we will demonstrate this can lead to spurious results when analysing data within a single country, let alone comparing countries with different staging systems.
Taking England as an example, the authors prioritised the use of T, N and M data over Dukes’ stage where available, preferring pathological T and N over clinically based values. In doing so, a problem arises if a significant proportion of tumours are staged using the Dukes’ staging system. Dukes’ stage can be assigned at multi disciplinary team (MDT) meetings (using a combination of pathological and clinical information) or by the pathologist based on the specimen resected. Between 2000 and 2007, seven of eight English Cancer Registries predominantly staged colorectal cancer cases based on Dukes’ stage from pathological reports. Using pathological Dukes’ stage leads to an apparent downstaging of tumours when compared to a registry-derived integrated stage (this combines imaging, pathology and MDT data staging colorectal carcinomas). This is because the pathologist will not typically receive evidence of distant metastases in resected specimens. Indeed, the apparent downstaging is exacerbated as the Royal College of Pathologists (RCPath) defines Dukes’ C as the highest Dukes’ stage that a pathologist should record in their report, regardless of the presence of distant metastases. The reasoning behind the RCPath's recommendation is that the ultimate assessment for distant metastases should be made at MDT level.
Armed with this understanding of how the data is produced and where it comes from we were able to apply the methodology developed by Maringe et al. to colorectal carcinomas diagnosed between 1 January 2011 and 31 December 2011, and registered at the Eastern Office of the National Cancer Registration Service, Public Health England (formerly Eastern Cancer Registry and Information Centre). A total of 4880 cases were identified, of which 2406 had both a pathological stage and an integrated stage. We then compared the stage distribution of colorectal tumours obtained using the pathological stage (the methodology used by Maringe et al. when the source data supplied was of predominant pathological source) against the integrated stage for the same population of data.
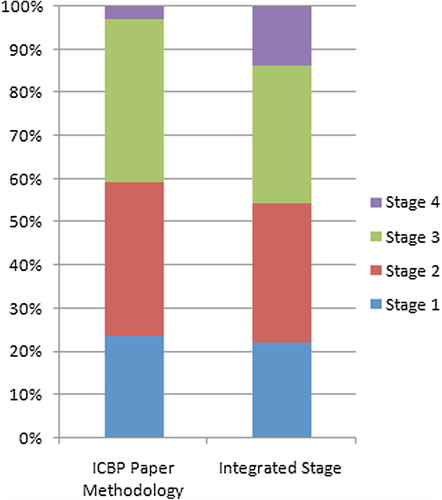
As seen in , the stage distribution determined by registry-derived integrated staging rules shows a significant increase (p-value = < 0.01) in the proportion of Stage 4 (Dukes’ D) tumours and a significant decrease in the proportion of Stage 2 (Dukes’ B) and Stage 3 (Dukes’ C) tumours as compared to the stage distribution determined using the Maringe et al. methodology when only pathological stage is available. This is a direct result of the correct allocation of tumours to Stage 4 (Dukes’ D) using the integrated stage.
Figure 1. Comparison of staging profiles using ICBP paper methodology and integrated stage.
shows that correctly assigning stage also has a significant (p-value = < 0.01) positive effect on survival in Stage 3 and 4 tumours consistent with the Will Rogers phenomenon [Citation4–6]. Stage 3 tumour one-year overall survival increases from 85% to 90% and Stage 4 tumour one-year overall survival increases from 33% to 63%. The small number of Stages 2 and 3 tumours that were downstaged represent cases where the pathological stage was not the stage at diagnosis (either post-chemotherapy or represented progression of disease).
Figure 2. Schematic showing stage, with corresponding numbers alive after one year against total number and percentage one-year overall survival.
In conclusion, misinterpretation of the origins and composition of the data used in analysis has significant ramifications upon stage distribution and consequently on the one-year overall survival, particularly for Stages 3 and 4 tumours. Analysis of stage data, particularly when used in international comparisons must understand the source of the data if interpretation is to be meaningful. If Maringe et al. had had access to integrated stage data for the English colorectal carcinoma it is entirely reasonable to expect England to show broadly similar if not better stage distribution and one-year overall survival for colorectal cancer when compared to the other countries in the study.
Declaration of interest: The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
- Allemani C, Rachet B, Weir HK, Richardson LC, Lepage C, Faivre J, et al. Colorectal cancer survival in the USA and Europe: A CONCORD high-resolution study. Br Med J Open 2013;3:e003055.
- Walters S, Maringe C, Butler J, Brierley JD, Rachet B, Coleman MP. Comparability of stage data in cancer registries in six countries: Lessons from the International Cancer Benchmarking Partnership. Int J Cancer 2013;132:676–85.
- Maringe C, Walters S, Rachet B, Butler J, Fields T, Finan P, et al. Stage at diagnosis and colorectal cancer survival in six high-income countries: A population-based study of patients diagnosed during 2000–2007. Acta Oncol 2013;52:919–32.
- Sormani MP. The Will Rogers phenomenon: The effect of different diagnostic criteria. J Neurol Sci 2009;287 (Suppl 1):S46–9.
- Basu S, Alavi A. Staging with PET and the “Will Rogers” effect: Redefining prognosis and survival in patients with cancer. Eur J Nucl Med Mol Imaging 2008; 35:1–4.
- Kim MM, Hoffman KE, Levy LB, Frank SJ, Pugh TJ, Choi S, et al. Improvement in prostate cancer survival over time: A 20-year analysis. Cancer J 2012;18:1–8.