
To the Editor,
The 1984 industrial accident in Bhopal, India led to the immediate deaths of thousands and resulted in long-term morbidity for survivors. Although unknown at the time, the health consequences of exposure to the released gas, methyl isocyanate, included dysfunction of the central nervous system, pulmonary toxicity, and an increased risk of malignancy. The interval between exposure and development of clinically significant malignancies can be prolonged. We present a case of a woman diagnosed with both acute myeloid leukemia and mesothelioma 28 years after exposure to methyl isocyanate during the Bhopal disaster. Given the potential for a long latency between exposure and appearance of disease, practitioners must be aware of the health consequences for survivors of this industrial accident and maintain a high index of suspicion to detect incident cases given on going international migration.
Report of a case
A 67-year-old woman from the Indian subcontinent presented with one month of diffuse itching. She was otherwise in good health. She had recently moved from India to live in Dallas, Texas with her daughter. She had worked as a nurse while living in India. She was a non-smoker and denied environmental tobacco exposure. However, she did report exposure to the 1984 Bhopal gas leak. On 3 December 1984, water leakage into a storage tank triggered an explosion at the Union Carbide India Limited pesticide plant in Bhopal, India. This event led to the release of more than 30 tons of methyl isocyanate gas over approximately 80 square kilometers. The patient recalled standing outside with her neighbors to watch the fires burn at the plant. She also stated she was given a governmental identification card confirming she was a survivor of the disaster.
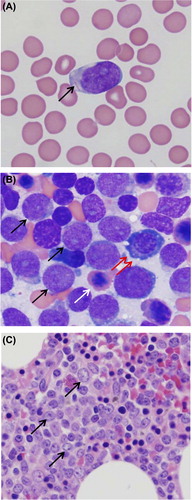
On exam, vital signs were stable and she had no abnormal pulmonary findings on auscultation. She had no lymphadenopathy, organomegaly, jaundice, or rash. Laboratory data demonstrated a white blood cell count of 11 000 with 95% blasts. shows the patient's peripheral smear with a circulating blast cell (arrow). Bone marrow aspirate revealed numerous myeloblasts (, black arrows), a lymphoid precursor (, double red arrow), and an erythroid precursor (, white arrow). Bone marrow biopsy demonstrated 68% blasts with morphology consistent with acute myeloid leukemia (AML) (). Cytogenetic analysis confirmed AML with chromosome 9q deletion, specifically del(9)(q12q32). She underwent induction chemotherapy with “7 + 3” cytarabine-idarubicin regimen. She completed induction therapy but her clinical course was complicated by two weeks of prolonged neutropenic fever requiring broad spectrum antibiotics.
Figure 1. Peripheral smear with circulating blast (A), bone marrow aspirate demonstrating myeloblasts with lymphoid and erythroid precursor cells (B), and bone marrow biopsy consistent with acute myeloid leukemia (C).
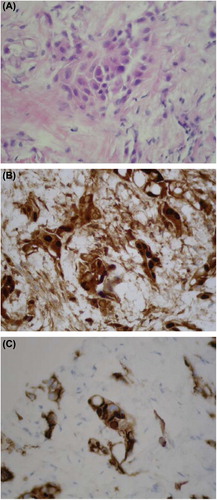
During this period, computed tomography (CT) of the chest, abdomen, and pelvis was performed to identify a potential source of the fever. These studies revealed multiple bilateral peripheral and subpleural nodules (). Given concern for leukemic infiltrates or a second primary malignancy, CT-guided biopsy of a right upper lung nodule was performed. Pathology demonstrated malignant mesothelioma, epithelioid type, without evidence of hematolymphoid malignancy (). Immunohistochemical staining was positive for both cytoplasmic and nuclear calretinin () and cytoplasmic D2–40 () confirming mesothelial origin of the cells.
Figure 2. CT chest demonstrating bilateral peripheral and subpleural nodules consistent with malignant mesothelioma.
Figure 3. Biopsy of right upper lung nodule demonstrating epithelioid mesothelioma (A) with immunohistochemical staining positive for calretinin (B) and cytoplasmic D2-40 (C) confirming mesothelial origin of biopsied cells.
Subsequently, the patient completed one cycle of high-dose Ara-C (HiDAC) consolidation therapy. She declined any treatment for the mesothelioma. Her pulmonary disease was unchanged on repeat imaging two months later.
Discussion
The gas disaster at Bhopal remains the world's worst industrial accident. While exact numbers are unknown, it is believed that approximately 8000 people died from methyl isocyanate poisoning within 72 hours of the explosion. Used as an intermediate in pesticide production, methyl isocyanate is a toxic organic compound known to cause inflammation, extensive DNA damage, and genomic instability [Citation1]. The long-term health effects of this agent remain unclear [Citation2]. In the ensuing years, over 15 000 individuals have died from complications stemming from their exposure. There are over 500 000 registered victims of the Bhopal disaster who continue to experience chronic illnesses of the respiratory, neurologic, gastrointestinal, musculoskeletal, and reproductive systems [Citation3]. By comparison, the 1986 nuclear accident at Chernobyl led to only 57 direct deaths with approximately 4000 additional deaths related to the development of cancer among the most highly exposed individuals. However, while the effects of Bhopal were limited to a remote area of central India, the nuclear fallout from Chernobyl resulted in the exposure of an estimated 400 million people across Eastern Europe and additional environmental exposure across Scandinavia due to wind direction. As a result, there is a vast amount of global data analyzing the health effects of Chernobyl [Citation4]. In contrast, the health consequences of the Bhopal disaster have received little attention in Western medical literature.
Despite initial clinical research on the detrimental effects of methyl isocyanate exposure following the Bhopal disaster, there remains a paucity of information regarding the long-term health implications for survivors. Affected individuals suffer from chronic illnesses such as pulmonary fibrosis, asthma, chronic obstructive pulmonary disease, keratopathy, corneal opacities, and a heightened incidence of neuromuscular defects [Citation3]. Perinatal and neonatal mortalities are significantly higher in the exposed geographic area [Citation5]. Although no study has established a conclusive link between methyl isocyanate and carcinogenesis, observational cohort studies published in South Asian medical journals suggest that exposed individuals are at increased risk of cancers, particularly those involving the oral cavity, lung, esophagus, and cervix [Citation6]. Malignancies that developed after the Bhopal disaster continue to be tallied in a Bhopal population-based cancer registry. Reported hematologic malignancies include non-Hodgkin's lymphoma and acute leukemia [Citation7]. An analysis of the Bhopal cancer registry from 2006–2011 found approximately 1200 separate newly diagnosed malignancies in individuals exposed to methyl isocyanate [Citation8]. Breast and lung cancers were found to have the highest incidence during the examined time period followed by malignancies of the oral cavity and cervix. There were six reported cases of AML and no described cases of mesothelioma.
Methyl isocyanate is an organic compound used as an intermediate in the production of carbamate pesticides. A clear and colorless liquid, methyl isocyanate will hydrolyze in an exothermic reaction. The leakage of water into the tank containing methyl isocyanate at Bhopal led to a vigorous reaction resulting in the aerosolization of this gas. Although an irritant with a pungent odor, methyl isocyanate is thought to have poor warning properties as human thresholds for detection of mucosal irritation and odor exceed the threshold limit of chemical exposure [Citation9]. Prior to the Bhopal disaster, no studies had been done to examine the long-term health effects of exposure. Presumably, as an intermediate in a closed production process, methyl isocyanate was not subjected to detailed examination of its toxicity because it was thought to have limited potential for wide spread human exposure [Citation10]. The lack of knowledge regarding the toxic effects of this gas prior to the Bhopal disaster hindered the ability of practitioners to anticipate the clinical course of various exposure-related illnesses [Citation11].
Inhalation of methyl isocyanate results in abnormal gas exchange, decreased oxygen affinity of hemoglobin, and deposition of mucus and fibrin in small airways leading to obstruction [Citation10]. The mechanism underlying the risk of increased malignancies in this exposed population centers on a heightened occurrence of chromosomal abnormalities leading to carcinogenesis [Citation6,Citation12–14]. An association between genetic abnormalities and methyl isocyanate exposure in Bhopal survivors has been demonstrated. A study performed shortly after the disaster demonstrated an increased number of chromosomal aberrations in peripheral lymphocytes obtained from methyl isocyanate exposed individuals compared to those from an unexposed group [Citation1]. The patient described in this case presented with AML characterized by del(9q). Unfortunately, cytogenetic analysis could not be performed on the patient's mesothelioma tissue specimen as the biopsy was formalin fixed and paraffin embedded.
Conclusion
This case highlights a number of important considerations regarding the Bhopal disaster: 1) methyl isocyanate exposure may be associated with diverse malignancies; 2) the interval between exposure and development of clinically evident malignancy may be prolonged, requiring ongoing surveillance to detect incident cases; and 3) due to increasing international migration, identifying diseases potentially related to the event requires global tracking of exposed individuals. Furthermore, this report is unique in that it presents the only known occurrence of mesothelioma in a methyl isocyanate- exposed survivor. While the patient's lack of asbestos exposure is unverifiable, this case demonstrates that methyl isocyanate exposure may lead to a lengthy latency period comparable to that seen in asbestos-exposed individuals [Citation15]. New malignancies continue to be described in Bhopal survivors. Six malignancies previously not described in methyl isocyanate-exposed survivors were described in the most recent registry report [Citation8]. The development of two primary cancers in the current case suggests a possible common molecular mechanism. Given the long-term carcinogenic effects of methyl isocyanate, ongoing monitoring of affected populations and further research are clearly needed.
Declaration of interest: The authors of this report have no conflicts of interest to report.
References
- Malla TM, Senthilkumar CS, Sharma NC, Ganesh N. Chromosome instability among Bhopal gas tragedy survivors. Am-Euras J Toxicol Sci 2011;3:245–9.
- Mishra PK, Bhargava A, Raghuram GV, Gupta S, Tiwari S, Upadhyaya R, et al. Inflammatory response to isocyanates and onset of genomic instability in cultured human lung fibroblasts. Genet Mol Res 2009;10:129–43.
- Mishra P, Samarth R, Pathak N, Jain SK, Banerjee S, Maudar KK. Bhopal gas tragedy: Review of clinical and experimental findings after 25 years. Int J Occup Med Environ Health 2009;22:193–202.
- Drozdovitch V, Bouville A, Chobanova N, Filistovic V, Ilus T, Kovacic M, et al. Radiation exposure to the population of Europe following the Chernobyl accident. Radiat Prot Dosimetry 2007;123:515–28.
- Dhara VR, Dhara R, Acquilla SD, Cullinan P. Personal exposure and long-term health effects in survivors of the Union Carbide disaster at Bhopal. Environ Health Perspect 2002;110:487–500.
- Goswami HK, Chandorkar M, Bhattacharya K, Vaidyanath G, Parmar D, Sengupta S, et al. Search for chromosomal variations among gas-exposed persons in Bhopal. Human Genetics 1990;84:172–6.
- Dikshit R, Kanhere S, Surange S. Cancer survival in Bhopal, India, 1991–1995. IARC Sci Publ 2011;162:107–13.
- Senthilkumar CS, Malla TM, Sah NK, Ganesh N. Cancer morbidity among methyl isocyanate exposed long-term survivors and their offspring: A hospital-based five year descriptive study (2006–2011) and future directions to predict cancer risk in the affected population. Asian Pac J Cancer Prev 2011;12:3443–52.
- Bucher JR. Methyl isocyanate: A review of health effects research since Bhopal. Fundam Appl Toxicol 1987;9: 367–79.
- Salmon AG. Does acute toxicity testing tell us anything useful?Methyl isocyanate as a test case. Br J Ind Med 1985;42:577–8.
- Crabb C. Revisiting the Bhopal tragedy. Science 2004; 306:1670–1.
- Senthilkumar CS, Sah NK, Ganesh N. Methyl isocyanate and carcinogenesis: Bridgeable gaps in scientific knowledge. Asian Pac J Cancer Prev 2012;13:2429–35.
- Mason JM, Zeigler E, Haworth S, Ivett J, Valencia R. Genotoxicity studies of methyl isocyanate in Salmonella, Drosophila, and cultured Chinese hamster ovary cells. Environ Mutagen 1986;9:19–28.
- Shelby MD, Allen JW, Caspary WJ, Haworth S, Ivett J, Kligerman A, et al. Results of in vitro and in vivo genetic toxicity tests on methyl isocyanate. Environ Health Perspect 1987;72:181–5.
- van der Bij S, Koffijberg H, Burgers JA, Baas P, van de Vijver MJ, de Mol BA, et al. Prognosis and prognostic factors of patients with mesothelioma: A population-based study. Br J Cancer 2012;107:161–4.