
Abstract
Background. Residents of geothermal areas have increased incidence of non-Hodgkin's lymphoma, breast, prostate, and kidney cancers. The aim was to study whether this is also reflected in cancer mortality among the population using geothermal hot water for space heating, washing, and showering.
Methods. The follow-up was from 1981 to 2009. Personal identifier of those 5–64 years of age was used in record linkage with nationwide death registry. Thus, vital and emigration status was ascertained. The exposed population was defined as inhabitants of communities with district heating generated from geothermal wells since 1972. Reference populations were inhabitants of other areas with different degrees of volcanic/geothermal activity. Hazard ratio (HR) and 95% confidence intervals (CI) were adjusted for age, gender, education, housing, reproductive factors and smoking habits.
Results. Among those using geothermal water, the HR for all causes of death was 0.98 (95% CI 0.91–1.05) as compared with cold reference area. The HR for breast cancer was 1.53 (1.04–2.24), prostate cancer 1.74 (1.21–2.52), kidney cancer 1.78 (1.03–3.07), and for non-Hodgkin's lymphoma 2.01 (1.05–3.38). HR for influenza was 3.36 (1.32–8.58) and for suicide 1.49 (1.03–2.17).
Conclusion. The significant excess mortality risk of breast and prostate cancers, and non-Hodgkin's lymphoma confirmed the results of similarly designed studies in Iceland on cancer incidence among populations from high-temperature geothermal areas and users of geothermal hot water. The risk is not confined to cancers with good prognosis, but also concerns fatal cancers. Further studies are needed on the chemical and physical content of the water and the environment emissions in geothermal areas.
Air pollution and its impact on human health have been considered a serious problem in active volcanic areas. Millions of people globally live within volcanic-geothermal areas [Citation1]. Toxic emissions from volcanic and geothermal areas include carbon dioxide (CO2), sulphur dioxide (SO2), hydrogen chloride (HCl), hydrogen fluoride (HF), hydrogen sulphide (H2S), carbon monoxide (CO), radon (Rn) and various trace elements [Citation2–6]. Unlike emissions of hazardous air pollutants during eruptions, ground gas emissions from geothermal fields are continuous and communities in these areas may be chronically exposed to elevated gas concentrations.
The main components of the gas emissions from the geothermal fields and fumaroles in Iceland are CO2, H2S, SO2, and hydrogen (H2) and the information available from Icelandic settings indicate the presence of traces of hazardous elements in the geothermal water including arsenic (As) (1–2 ppb), mercury (Hg) (0.05 ppb), and Rn (3–100 Bq/l), i.e. in low quantities, but in varying concentrations [Citation7–10]. The geothermal hot water, from deep drilled wells (down to 800 m), has been piped into power plants, industries, green houses and domestic houses and used for heating, laundry, bathing, showering and washing dishes [Citation11]. The faint rotten egg odour of H2S breaking out from showers, spas and swimming pools are frequently perceived by foreign visitors, while the local population seem to have acclimatised the smell. Approximately 90% of all houses and swimming pools are at present heated with geothermal water and 12% of the electricity is generated from geothermal power plants in Iceland [Citation11]. The geothermal water is not used for drinking water because it is bad tasting and foul smelling.
Long-term mortality studies on populations living on geothermal fields or in volcanic areas are rare. A mortality study in New Zealand's Rotorua geothermal area showed an elevated ratio for diseases of the respiratory system; however, that finding was possibly confounded by ethnicity [Citation12]. The study in Rotorua did not include mortality from cancer [Citation12]. An ecological study of the population in geothermal areas of Tuscany, Italy [Citation13] showed excess mortality among males for respiratory diseases, in particular due to pneumoconiosis, including silicosis, and an excess of tuberculosis was also found, thus possibly indicating significant industrial exposure, besides geothermal emissions.
Previous studies on the incidence of cancer among populations in geothermal or volcanic areas have been inconsistent [Citation14–16], however a pattern has emerged from two Icelandic studies showing increased incidence of non-Hodgkin's lymphoma, breast, and prostate cancers, and basal cell carcinoma of the skin [Citation17,Citation18].
Many of the tumours found in excess in the incidence studies [Citation14,Citation16–18] have good prognosis, and are possibly subject to detection bias. Mammography screening and prostate-specific antigen testing may produce overdiagnosis [Citation19,Citation20] of these cancers. Moreover, risk factors for advanced or lethal breast and prostate cancers may be different from those for indolent cancers [Citation21,Citation22]. These debatable questions call for assessment of the risk of cancer mortality among populations in geothermal areas.
The aim was to study cause-specific mortality, with special focus on cancer mortality, in geothermal areas where the population has been using geothermal hot water for space heating, bathing and washing for decades.
Methods
Iceland is located in the middle of the North Atlantic Ocean on the Mid-Atlantic Ridge where the North American and Eurasian tectonic plates move apart. These movements can be observed in Iceland, which gets 2 cm longer from east to west each year, and Iceland has great volcanic activity and several geothermal fields [Citation23,Citation24].
The source of data for this cohort study was the 1981 National Census in Iceland. The material has been described in previous studies, so a short outline will be given here [Citation17,Citation18].
The census included information on personal identification number, gender, age, residency, education, and type of housing. The cohort included people aged 5–64 years. Personal identification numbers were used in record linkage with the National Registry to obtain information, where applicable, on the date of emigration and with the National Cause-of-Death Registry to obtain information on vital status and, where applicable, the date and the cause of death according to death certificates. These registries are kept at Statistics Iceland. Through this procedure it was possible to ascertain the vital and emigration status for the entire cohort.
The European shortlist [Citation25] was used to define the causes of death and to standardise these to ICD-10 [Citation25], except for the cancers, where the same categories were used as in previous studies also complying with ICD-10 [Citation17,Citation18].
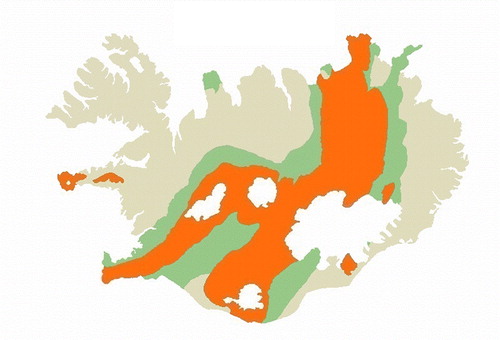
The age of the bedrock played a pivotal role in the definition of the populations studied (). The four-digit community code in the census was used to identify the populations living in communities with geothermal heating since 1972 or earlier, according to an overview of geothermal primary energy production [Citation11,Citation26]. In these communities the hot water was used for domestic heating, laundry, bathing, showering, and washing dishes, and in spas and swimming pools, but not as drinking water. These are the communities dealt with in previous studies [Citation17,Citation18], here called geothermal heating areas. They included three small towns, two of these were inland, Selfoss (8100), Hveragerdi (8716), and one was coastal, Husavik (6100), and six rural districts Reykjahreppur (6610), Skutustadahreppur (6607), Laugardalshreppur (8712), Biskupstungnahreppur (8711), Hrunamannahreppur (8710), and Skeidahreppur (8708) (), and they are all located within the volcanic zone in the middle of the country, where the bedrock is less than 3.3 million years old () [Citation23,Citation24].
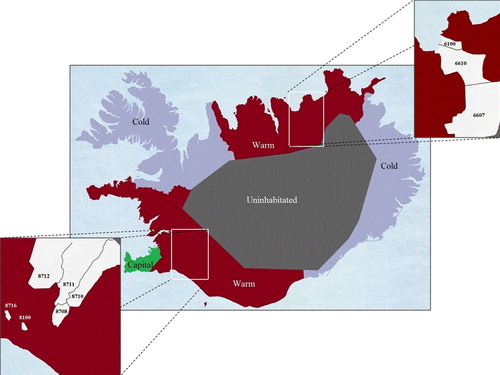
The two comparison populations were identified by the community codes in the census [Citation26] according to the age of the bedrock [Citation23,Citation24] and without geothermal heating system as old as 1972 [Citation11]. The main reference area, the cold area, was located in the west and east parts of the country where the bedrock is more than 3.3 million years old, and the warm reference area was located in the middle of the country, where the age of the bedrock is 0.8–3.3 million years old. These reference areas are the same as in a previous study [Citation18] ().
The populations in the capital Reykjavik and in the south-west peninsula of Reykjanes were excluded from the study, as the population of the capital area and its adjacent south-west peninsula has had higher cancer incidence than the rest of the country in the Cancer Registry since the beginning of the registry [Citation27], a well-known phenomenon in cancer registries, sometimes called the capital effect.
The follow-up started on the day of the census, 31 January 1981, and continued to the date of emigration, or date of death, or 31 December 2009 (the end of the follow-up period), whichever occurred first.
Survival for the event-free proportion was shown for the exposed group and the two reference groups combined by Kaplan-Meier curves for breast, and prostate cancer mortality, non-Hodgkin's lymphoma, and suicides [Citation28].
The Cox proportional hazard model was used to estimate hazard ratio (HR) and 95% confidence intervals (95% CI) for all causes of death and selected causes of death [Citation29]. Gender was introduced as a dichotomous variable, and age as a continuous variable in years. Educational level (basic, medium and academic education), was introduced as a categorical variable according to the previous classification in a census study [Citation30] with two additional categories: one, unclassified for people under 20 years of age, who had not yet attained their full education level, and another missing educational information to include individuals who did not indicate their education in the census. Type of residence, single-family house or other type of residence, was introduced as a dichotomous variable.
The exposed population living in the geothermal heating area was compared with the other populations (warm reference area and cold reference area) in separate analyses. Several calculations were done in the model: crude comparison without any adjustments, comparison with adjustment for age and gender only, and with adjustment for age, gender, educational level, housing, and smoking. These models had nearly identical results. Only the results with all these adjustments are presented here. Further adjustment for urban/rural region did not change the results and were omitted from the model. Separate analyses were done after dividing the material by gender, and then the cold and warm reference populations were combined into one comparison population, and into groups of individuals who were 20 years of age or older at the time of the census, and those who were under 20 years of age.
Information on smoking was not collected in the census and thus not available on an individual level. Since 1985, the Public Health Institute of Iceland has collected results from annual surveys on smoking habits among random samples of the population according to gender and postal codes [Citation31]. Raw data on smoking surveys during 1991 to 1995 were obtained from the institute for the purpose of this study. The postal codes were translated to 22 community areas to fit into the community codes in the census and rates for never-smokers were calculated for each community and gender. These estimated never-smoker rates were assumed for inhabitants of the study areas, and allocated to the individuals of the respective communities regardless of age, but broken down by gender, and introduced as a continuous variable in the Cox model.
Information on reproductive factors was not available from the census. The most important reproductive factor, age at first birth [Citation32], was estimated according to information from Statistics Iceland [Citation26] with calculation of codes on age at first birth (< 25 and 25+) by a method described in the previous publication [Citation18]. In order to adjust for possible confounding, these community codes were introduced as a continuous variable in the Cox model in a separate analysis for breast cancer mortality.
The statistical analyses were performed using the PASW (SPSS) software version 18, and Microsoft Excel 2007.
The National Bioethics Committee (VSNb201 0060005/03.1) and the Data Protection Commission (2010060524ÞPJ/--) approved the study.
Results
The national census in 1981 used in the study covered, according to the National Registry, 99.2% of the population aged 5–64 years [Citation18,Citation26]. During the follow-up, a total of 10 102 persons had died, 6132 men and 3970 women.
The baseline characteristics in the three study populations: Geothermal heating area and the reference areas (warm area, and cold area) are shown in . The proportion of never-smokers in the geothermal heating area was 43.8, it was 46.9 in the warm reference area, and 44.7 in the cold reference area.
Table I. Baseline characteristics in the geothermal heating area and the two reference areas according to census 1981.
shows the results of the Kaplan-Meier analyses; these demonstrate the time until deaths occur due to breast and prostate cancer, non- Hodgkin's lymphoma, and suicide in the geothermal heating area and the combined reference areas.
The number of all causes of death, and selected causes of death for the genders combined in the three areas, the HR, and 95% CI, adjusted for age, gender, education, type of housing, and smoking habits are shown in Supplementary Table I (available online at http://informahealthcare.com/doi/abs/10.3109/0284186X.2014.923113). During the follow-up, 996 deaths were among men and women in the geothermal heating area and the HRs for all causes of death were 1.01 (95% CI 0.94–1.08) compared with the warm reference area, and 0.98 (95% CI 0.91–1.05) compared with the cold reference area. The HRs for all cancers were 1.05 (95% CI 0.94–1.18), and 1.03 (95% CI 0.92–1.17) compared with the reference areas. The HRs for breast cancer were 1.48 (95% CI 1.03–2.12), and 1.53 (95% CI 1.04–2.24). The HRs for prostate cancer were 1.88 (95% CI 1.33–2.66), and 1.74 (95% CI 1.21–2.52). The HRs for kidney cancer were 1.39 (95% CI 0.85–2.28), and 1.78 (95% CI 1.03–3.07). The HRs for lymphoid and haematopoietic tissue cancer were 1.29 (95% CI 0.90–1.86), and 1.25 (95% CI 0.85–1.84), and for non-Hodgkin's lymphoma 1.96 (95% CI 1.09–3.55), and 2.01 (95% CI 1.05–3.84).
The HRs for all diseases of the respiratory system were 1.04 (95% CI 0.80–1.35), and 1.08 (95% CI 0.82–1.42), and for influenza 3.77 (95% CI 1.58–8.99), and 3.36 (95% CI 1.32–8.58). The HRs for suicide and intentional self-harm were 1.72 (95% CI 1.20–2.48), and 1.49 (95% CI 1.03–2.17).
Among men, 596 deaths occurred in the geothermal heating area, and the HR for all causes of death was 1.00 (95% CI 0.91–1.08), adjusted for age, education, housing, and smoking in comparison with the combined reference areas (). The HRs for all cancers were 1.06 (95% CI 0.91–1.23), for prostate cancer 1.88 (95% CI 1.37–2.60), and for non-Hodgkin's lymphoma 2.31 (95% CI 1.21–4.41). The HR for influenza was 3.10 (95% CI 1.09–8.84). The HR for suicide and intentional self-harm was 1.46 (95% CI 1.00–2.13).
Table II. Number of all causes of death and selected causes of death among men and women separately in the geothermal heating area, hazard ratio (HR), 95% confidence intervals (CI) according to comparison with the reference areas combined, adjusted for age, education, type of housing, and smoking habits. Statistically significant HRs are in bold.
Among women, 400 deaths occurred in the geothermal heating area, and the HR for all causes of death was 1.00 (95% CI 0.90–1.11), adjusted for age, education, housing, and smoking in comparison with the combined reference areas (). The HRs for all cancers were 1.04 (95% CI 0.89–1.23), and for breast cancers 1.49 (95% CI 1.06–2.09). The HR for immunoproliferative diseases was 8.39 (95% CI 1.15–61.42) based on two death cases. The HR for influenza was 3.99 (95% CI 1.21–13.18). The HR for suicide and intentional self-harm was 2.05 (95% CI 1.02–4.15).
Restricting the analysis to those 20 years of age and older at the time of the census, there were 949 deaths in the geothermal heating area. In this older part of the cohort, comparison of the geothermal heating area with the combined reference areas gives similar HRs as in the total exposed cohort and HR for all causes of death was 0.99 (95% CI 0.93–1.06). The HRs for all cancers were 1.05 (95% CI 0.93–1.17), for breast cancer 1.40 (95% CI 0.99–2.00), for prostate cancer 1.88 (95% CI 1.36–2.59), for kidney cancer 1.57 (95% 0.98–2.51). The HRs for lymphoid and haematopoietic tissue cancer were 1.33 (95% CI 0.94–1.89), and for non-Hodgkin's lymphoma 2.01 (95% CI 1.16–3.49). The HRs for all diseases of the respiratory system were 1.05 (95% CI 0.82–1.35), and for influenza 3.22 (95% CI 1.48–7.02). The HRs for all external causes were 1.09 (95% CI 0.83–1.75), and suicide and intentional self-harm 1.80 (95% CI 1.21–2.68), adjusted for age, gender, education, type of housing, and smoking habits. HRs for other causes of death did not significantly deviate from unity.
Restricting the analysis to those under 20 years of age at the time of the census, there were 47 deaths in the geothermal heating area. The HRs for all causes of death, all cancer deaths, and suicide and intentional self-harm were higher in the geothermal heating area compared to the combined reference areas, but not to a statistically significant degree. The HR for breast cancer deaths in this younger part of the cohort, based on four cases, was significantly elevated 4.65 (95% CI 1.33–16.21).
Analysing the breast cancer mortality with additional adjustment for age at first birth, the HR was 1.44 (95% CI 0.94–2.19), when restricted to those 20 years of age and older the HR was 1.29 (95% CI 0.83–2.02), and for those under 20 years of age the HR was 5.91 (95% CI 1.52–22.90).
Discussion
This population-based study on nearly a thousand deaths in areas supplied with geothermal hot water used for heating, bathing and washing for decades, which shows increased mortality for breast and prostate cancer, and non-Hodgkin's lymphoma, confirms results from similarly designed incidence studies on increased risk for these cancers [Citation17,Citation18]. It is thus unlikely that these previous studies on cancer incidence were skewed by detection bias and overdiagnosis [Citation17,Citation18]. The increased mortality for breast cancer in the present study is consistent with the increased incidence of breast cancer among the population in the Furnas village, located in geothermal area of the volcanic island Sao Miguel, in Azores [Citation14]. There was increased mortality for kidney cancer corresponding to the increased kidney cancer incidence in the previous study [Citation18]. In this mortality study it was possible to adjust for social variables such as education and type of housing, and for estimates of age at first birth (reproductive factor) and smoking habits. Contrary to the previous cancer incidence studies, no clear evidence of exposure- response relation were observed between breast and prostate cancers, or non-Hodgkin's lymphoma and the degree of volcanic/geothermal activity of the reference areas in the present study.
Most of the remaining causes of death were in line with averages, and the HRs for diseases of the nervous and circulatory system were close to unity. An exception was an excess for influenza, based on nine cases, but mortality for other diseases of the respiratory system was not increased. In the Rotorua geothermal area study, an increased standardised mortality ratio was found due to all diseases of the respiratory system, confined to female and particularly Maori female, and concerned the subcategories: pneumonia and influenza combined, and chronic obstructive respiratory diseases [Citation12]. In the Tuscan geothermal area study, there seemed also to be an excess mortality for all diseases of the respiratory system among males, mainly due to an excess of pneumoconiosis [Citation13]. The three- to four-fold increase in mortality for influenza was fairly consistent compared to the two reference areas and among both genders in the present study. The significance of these findings is uncertain; however, in the light of previous studies [Citation17,Citation18] one may speculate whether this is an indication of an immunosupression.
Mortality for all external causes of death was not significantly increased; however, suicides were increased for both males and females. This was not hypothesised and came unexpected, as suicide risk is not mentioned in previous mortality studies from geothermal areas [Citation12,Citation13] and is here without explanation. In this connection it is worth pointing out that the proportion of individual living in rural regions was lowest in the geothermal heating area, thus not indicating an overrepresentation of farmers in that population, compared to the reference populations. Further, possible social differences were adjusted for with two variables form the census, educational level and type of housing.
Strength
Strength of the study is the long follow-up time of the cohort. Furthermore, the use of the comprehensive population registries and the personal identification number, which enabled easy and accurate record linkage, strengthen the study. Thus, vital and emigration status were ascertained through the National Registry and the National Cause-of-Death Registry for all individuals in the exposed cohort and the two reference populations. No information was missing from death certificates, and only 0.2% of the causes of death among the exposed cohort were reported on the death certificates as due to unknown and unspecified causes. This low proportion is indicative of the quality of the information.
All death certificates are issued by a physician, and if the deceased person's physician is not able to attest the cause of death or when the circumstances of the death are unexplained, unusual, suspicious, due to intoxication, or following an accident, the death is reported to the police and the medical examiner, who carry out an autopsy and forensic investigations before the death certificate is issued [Citation33]. An in-depth study on the quality of the recording of the cause of death on death certificates in Iceland is not available. However, when evaluating death registration at a global level, the quality of registration data from Iceland was categorised as high overall and ranked in the same category as data from 23 developed countries including the US and the UK [Citation34].
As said previously, the results of this study oppose the possibility of detection bias concerning breast cancer and prostate cancer. Mammography screening has been offered to the female population, aged 49–69 years, since 1987, and the participation rate since then has been around 70%, with no indication of geographical disproportional distribution [Citation27]. No systematic screening for prostate cancer has been carried out in the study populations; however, sporadic prostate-specific antigen testing might have occurred in these populations as elsewhere. In the general population in Iceland the incidence of breast and prostate cancer has been steadily increasing from 1959 to 2010, while mortality for breast cancer has decreased and mortality for prostate cancer has been constant over the period 1995–2010 [Citation27].
Limitation
More than 50 calculations of HR for all causes of death and selected causes of death were performed in the present study. The HRs for the rare causes of death are shown for descriptive purposes; however, the main interest was in relation to cancers, which had been in excess in previous incidence studies [Citation17,Citation18]. The many calculations performed in the study may give rise to concern; however, it has been argued that no adjustment is needed for these [Citation35].
A limitation here is the lack of exact information on the physical and chemical content of the geothermal water used for space heating system since 1972 in the target communities. The components of gas emissions have been documented in other geothermal areas [Citation3,Citation4,Citation6,Citation7]; however, the content of the geothermal hot water has not been investigated for the purpose of this study.
Information of occupation from the census was not available for this study; however, the results were adjusted for social variables, such as education, and type of housing.
Future studies should use length of residency in areas with the geothermal hot water systems as a surrogate for the exposure among these populations. To that information, one should link measurements on physical, chemical and biological components of the geothermal water [Citation36]. In the present study adjustment was made for the levels of individual exposure in terms of social-related variables, and also for smoking habits and reproductive factors on the community level, and these factors do not seem to be associated with cancer mortality. Moreover, the focus should be on factors of concern in previous studies in volcanic areas. A recent study showed evidence of DNA damage among individuals from the volcanically active area in Furnas, Azores [Citation37]. This finding was attributed to degassing in the volcanic environment in general, and particular to the Rn emission [Citation37]. The settings may be different in Iceland; nevertheless the use of geothermal hot water for showering and in spas has analogies with studies on the release of Rn and its decay products from shower water, which leads to transient increase in airborne Rn concentration [Citation38,Citation39]. The decreased lung cancer mortality in the present study, although is not statistically significant, does not indicate serious indoor Rn exposure of the population with the long-term usage of geothermal water.
Conclusion
The significant excess mortality risk of breast and prostate cancers, and non-Hodgkin's lymphoma confirmed the results of similarly designed studies on cancer incidence among populations from high-temperature geothermal areas and users of geothermal hot water. The cancer risk is thus not confined to cancers with good prognosis, but also concerns fatal cancers. Adjustment was made for individual social-related variables, as well as for reproductive factors and smoking habits on the community level. Further studies are needed on the chemical and physical content of the environmental emissions in geothermal areas, and the exposure and the dermal contamination resulting from the use of the geothermal water.
Supplementary material available online
Supplementary Table I (available online at http://informahealthcare.com/doi/abs/10.3109/0284186X.2014.923113).
ionc_a_923113_sm7914.pdf
Download PDF (33.3 KB)Declaration of interest: The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
This study was supported by grants from the Icelandic Centre for Research (RANN S), grant number 141746-051, and the University of Iceland Research Fund, grant number 1238-123368.
References
- Small C, Naumann T. The global distribution of human population and recent volcanism. Global Environ Change Part B: Environ Hazards 2001;3:93–109.
- Bernstein RS, Baxter PJ, Buist AS. Introduction to the epidemiological aspects of explosive volcanism. Am J Public Health 1986;76(3 Suppl):3–9.
- Durand M, Scott BJ. Geothermal ground gas emissions and indoor air pollution in Rotorua, New Zealand. Sci Total Environ 2005, 345:69–80.
- Allen AG, Baxter PJ, Ottley CJ. Gas and particle emissions from Soufriére Hills Volcano, Montserrat, West Indies: Characterization and health hazard assessment. Bull Volcanol 2000;62:8–19.
- Hansell A. Health hazards from volcanic gases: A systematic literature review. Arch Environ Health 2004; 59:628–39.
- Carapezza ML, Badalamenti B, Cavarra L, Scalzo A. Gas hazard assessment in a densely inhabited area of Colli Albani Volcano (Cava de i Selci, Roma). J Volcanol Geother Res 2003;123:81–94.
- Kristmannsdottir H. Efnasamsetning kalds neysluvatns á Husavik, vatns frá Husavikurhofda og Hafralaekjarskola. (Chemical content of drinking water Husavik, water from Husavikurhofda and Hafralaekjarskola). Skyrsla HK-04/04. Akureyri: University of Akureyri; 2004.
- Arnorsson S. Arsenic in surface- and up to 90°C ground water in basalt area. N-Iceland: Processes controlling its mobility. Applied Geo 2003;18:1297–312.
- Armannsson H, Gislason G, Hauksson T. Magmatic gases in well fluids aid the mapping of the flow pattern in geothermal system. Geochim Cosmochim Acta 1982;46:167–77.
- Einarsson P, Theodorsson P, Hjartardottir AR, Gudjonsson GI. Radon changes associated with the earthquake sequence in June 2000 in South Iceland seismic zone. Pure Appl Geophys 2008;165:63–74.
- Haraldsson IG, Ketilsson J. Frumorkunotkun jarðavarmavirkjana og hitaveitna á Íslandi til ársins 2009. (Geothermal primary energy production for electricity generation and heating in Iceland up to year 2009). OS-2010/03. Reykjavik: Orkustofnun; 2010.
- Bates MN, Garrett N, Graham B, Read D. Air pollution and mortality in Rotorua geothermal area. Aust N Z J Public Health 1997;21:581–6.
- Minichilli F, Nuvolone D, Bustaffa E, Cipriani F, Vigotti MA, Bianchi F. State of health of population residing in geothermal areas of Tuscany. Epidemiol Prev 2012;36(Suppl 5):1–104.
- Amaral A, Rodrigues V, Oliveira J, Pinto C, Carneiro V, Sanbento R, et al. Chronic exposure to volcanic environments and cancer incidence in the Azores, Portugal. Sci Total Environ 2006, 367:123–8.
- Bates MN, Garrett N, Graham B, Read D. Cancer incidence, morbidity and geothermal air pollution in Rotorua, New Zealand. Int J Epidemiol 1998, 27:10–4.
- Pellegriti G, De Vathaire F, Scollo C, Attard M, Giordano C, Arena S, et al. Thyroid cancer incidence in the volcanic area of Sicily. J Natl Cancer Ins 2009, 101:1575–83.
- Kristbjornsdottir A, Rafnsson V. Incidence of cancer among residents of high-temperature geothermal areas in Iceland: A census based study 1981 to 2010. Environ Health 2012;11:73.
- Kristbjornsdottir A, Rafnsson V. Cancer incidence among population utilizing geothermal hot water: A census-based cohort study. Int J Cancer 2013;133:2944–52.
- Miller AB. Overdiagnosis of breast cancer. Int J Cancer 2013;133:2511.
- Sandhu GS, Andriole GL. Overdiagnosis of prostate cancer. J Natl Cancer Inst Monogr 2012;2012:146–51.
- Schairer C, Frawley P, Graubard BI, Graubard BI, Wellman RD, Buist DS, et al. Risk factors for inflammatory breast cancer and other invasive breast cancers. J Natl Cancer Inst 2013;105:1373–84.
- Huncharek M, Muscat J, Kupelnik B. Dairy products, diary calcium and vitamin D intake as risk factors for prostate cancer: A meta-analysis of 26,769 cases from 45 observational studies. Nutr Cancer 2008;60:421–41.
- Fridleifsson IB. Geothermal activity in Iceland. Jökull 1979, 29:47–56.
- Saemundsson K. Outline of the geology of Iceland. Jökull 1979, 29:7–28.
- European Commission (2013). European shortlist for causes of death. [cited 2013 Oct 16]. Available from: https://joinup.ec.europa.eu/catalogue/asset_release/european-shortlist-causes-death.
- Statistics Iceland. Statistics. [cited 2013 Dec 2]. Available from: http://www.statice.is/Pages/422.
- Jonasson JG, Tryggvadottir L. Krabbamein á Íslandi. Upplýsingar úr Krabbameinsskránni fyrir tímabilið 1955–2010. (Cancer in Iceland. Information from the Cancer Registry for the period 1955–2010). Reykjavik: Krabbameinsfelagid; 2012.
- Armitage P, Berry G. Statistical methods in medical research, 2nd ed. Oxford: Blackwell Scientific Publication; 1991.
- Cox DR. Regression models and life-tables. J Royal Statist Soc Series B (Methodological) 1972;34:187–220.
- Vidarsdottir H, Gunnarsdottir HK, Olafsdottir EJ, Olafsdottir GH, Pukkala E, Tryggvadottir L. Cancer risk by education in Iceland: A census-based cohort study. Acta Oncol 2008;47:385–90.
- Public Health Institute of Iceland. Umfang reykinga. Samantekt 2005. [cited 2012 May 18]. Available from: http://www2.lydheilsustod.is/media/tobaksvarnir/rannsoknir/reykingaskyrsla_2005.pdf.
- Ewertz M, Duffy SW, Adami HO, Kvale G, Lund E, Meirik O, et al. Age at 1st birth, parity and risk of breast cancer: A meta-analysis of 8 studies from the Nordic Countries. Int J Cancer 1990;46:597–603.
- Log um danarvottord, krufningar og fleira. 61/1998. [cited 2013 Nov 28]. Available from: http://www.althingi.is/lagas/nuna/1998061.html.
- Mathers CD, Fat DM, Rao C, Lopez AD. Counting the dead and what they died from: An assessment of the global status of cause of death data. Bull World Health Org 2005; 83:171–7.
- Rothman KJ. No adjustments are needed for multiple compassion. Epidemiology 1990;1:43–6.
- Marteinsson VT, Hauksdottir S, Hobel CFV, Kristmannsdottir H, Hreggvidsson GO, Kristjansson JK. Phylogenetic diversity analysis of subterranean hot springs in Iceland. Appl Environ Microbiol 2001;67:4242–8.
- Rodrigues AS, Arruda MSC, Garcia PV. Evidence of DNA damage in humans inhabiting a volcanically active environment: A useful tool for biomonitoring. Environ Int 2012; 49:51–6.
- Fitzgerald B, Hopke PK, Datye V, Raunemaa T, Kuusaplo K. Experimental assessment of the short- and long-term effects of 222Rn from domestic shower water on the dose burden incurred in normally occupied homes. Environ Sci Technol 1997;31:1822–9.
- Ishikawa T, Yasuoka Y, Tokonami S, Takahashi H, Suda H. Charagterization of airborne radon released by domestic showering and the use of a washing machine. J Radioanal Nucl Chem 2009;279:719–24.