
To the Editor,
Axitinib is a potent, selective, second-generation inhibitor of vascular endothelial growth factor receptor (VEGFR) 1, 2, and 3, and has been approved for the treatment of advanced renal cell carcinoma after failure of one prior systemic therapy. Compared with first-generation tyrosine kinase inhibitors (TKIs), such as sorafenib, axitinib is a more specific VEGFR inhibitor. The toxicity profile of axitinib is tolerable. Common adverse events of axitinib include diarrhea, hypertension, and fatigue, and they have also been reported after using other TKIs. Other adverse events, such as palmar-plantar erythrodysesthesia, cutaneous toxicity, and myelosuppression, are less commonly reported after using axitinib than after using other TKIs [Citation1].
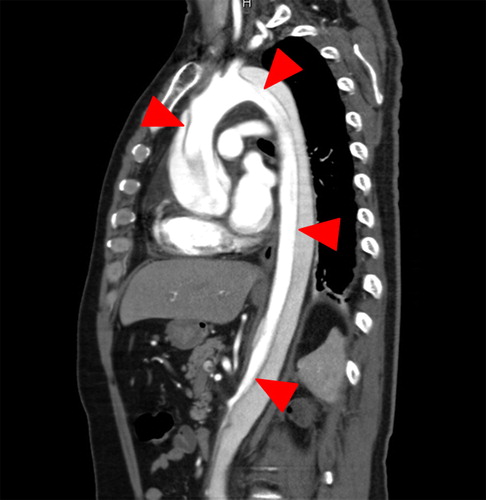
A 51-year-old man with a renal tumor, but without any other comorbidities including hypertension, underwent left radical nephrectomy. Pathological examination revealed the tumor as a pT3aN0M0 clear cell renal cell carcinoma. Six months after surgery, multiple lung metastases were detected via thoracic computed tomography (CT), after which sunitinib was administered as a four-weeks-on and two-weeks-off schedule. Sunitinib was discontinued owing to grade 3 palmar-plantar erythrodysesthesia after two cycles of treatment, and the patient was switched to axitinib. Ten days after receiving axitinib, he presented to the urology outpatient department with sudden midsternal pain. He looked well, and his blood pressure was 127/66 mmHg. An electrocardiogram showed ST-segment elevation in all leads. Contrast-enhanced thoracoabdominal CT revealed acute aortic dissection (Stanford type A) from the ascending aorta to the left external iliac artery (). The patient underwent emergency reconstruction of the ascending aorta.
Figure 1. Sagittal reconstruction of a contrast-enhanced computed tomography scan showing an aortic dissection involving the ascending aorta (arrowheads).
Acute aortic dissection is a life-threatening entity. The most common predisposing factor is hypertension, followed by atherosclerosis, history of cardiac surgery, Marfan syndrome, and iatrogenic causes [Citation2]. Hypertension is a frequent adverse event with axitinib and other small-molecule TKIs. Other cardiovascular toxicities including heart failure, left ventricular systolic dysfunction, and QT prolongation have also been reported. The mechanism of TKI-associated cardiotoxicity remains poorly understood. Possible mechanisms include the loss of vascular stability because of endothelial cell damage or decreased production of nitric oxide through inhibition of VEGF pathways [Citation3].
To our knowledge, this is the first case of acute aortic dissection in a patient treated with axitinib. Only two cases of aortic dissection during treatment with small-molecule multitargeted TKIs (1 with sorafenib [Citation4] and 1 with sunitinib [Citation5]) were previously published. Preexisting or drug-induced hypertension was observed in both cases. In this case, high blood pressure had not been observed before or during small-molecule multitargeted TKI therapy.
We suspected in this case aortic dissection is associated with axitinib, because he had no predisposing factor of aortic dissection including hypertension and it occurred soon after the initiation of axitinib. However, the causality between axitinib and acute aortic dissection could not be completely established in this case and further clinical observation is required. Axitinib has a relatively short history since its official approval, and its mechanism of action is not yet understood fully. Therefore, clinicians should be aware of this life threatening complication associated with using axitinib and other TKIs.
Declaration of interest: The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
- Rini BI, Escudier B, Tomczak P, Kaprin A, Szczylik C, Hutson TE, et al. Comparative effectiveness of axitinib versus sorafenib in advanced renal cell carcinoma (AXIS): A randomised phase 3 trial. Lancet 2011;378:1931–9.
- Sheikh AS, Ali K, Mazhar S. Acute aortic syndrome. Circulation 2013;128:1122–7.
- Lenihan DJ, Kowey PR. Overview and management of cardiac adverse events associated with tyrosine kinase inhibitors. Oncologist 2013;18:900–8.
- Serrano C, Suarez C, Andreu J, Carles J. Acute aortic dissection during sorafenib-containing therapy. Ann Oncol 2010;21:181–2.
- Edeline J, Laguerre B, Rolland Y, Patard JJ. Aortic dissection in a patient treated by sunitinib for metastatic renal cell carcinoma. Ann Oncol 2010;21:186–7.