
Abstract
Background. Patients with haematological malignancies have a poorer labour market prognosis than the general population. We have previously found that they have low rates of return to work, and a higher risk of being granted disability pension, than individuals without a history of these diseases. The aim of this study was to further investigate the labour market prognosis for these patients, by comparing the risk of being granted wage-subsidised (WS) employment as a result of permanently reduced work capacity among patients diagnosed with haematological malignancies to a reference cohort, and to determine if relative risks differ between subtypes of haematological malignancies.
Material and methods. We combined data from national registers on Danish patients diagnosed with haematological malignancies between 2000 and 2007 and a reference cohort without a history of these diseases. A total of 3194 patients and 28 627 reference individuals were followed until they were granted WS employment, disability pension, anticipatory pension, old age pension, emigration, death or until 26 February 2012, whichever came first.
Results. A total of 310 (10%) patients and 795 (3%) reference individuals had their work capacity permanently reduced to an extent that they were granted WS employment during the follow-up period. Age- and gender-adjusted relative risks differed significantly between the subgroups of haematological malignancies, and four years after diagnosis they ranged from 2.47 (95% CI 1.46–4.16) for patients with Hodgkin lymphoma to 10.83 (95% CI 7.15–16.40) for patients with chronic myeloid leukaemia.
Conclusion. All eight subtypes of haematological malignancies were associated with an increased risk of being granted WS employment due to permanently reduced work capacity compared to the reference cohort. The relative risks differed according to haematological malignancy subtype, and the highest was found for patients with chronic myeloid leukaemia.
The treatment of haematological malignancies has improved markedly during recent years, and more people therefore survive from these diseases. Previous studies have documented that these patients have a poor labour market prognosis compared to cancer-free control groups [Citation1–4] and patients with other cancer types [Citation5–8].
Treatment of haematological malignancies differs from that of other malignancies in several aspects. It rarely involves surgery, but more often chemotherapy for extended time periods. The various subtypes of haematological malignancies differ markedly in terms of their presentation, treatment, progression and outcome. The simplest categorisation is leukaemias, lymphomas and multiple myeloma. However, these diagnoses also comprise several subgroups of which some run a highly acute course, whereas others are chronic conditions with intermittent needs for treatment.
In two recent register-based cohort studies, we have shown that there is a clear need of distinguishing between different types of haematological malignancies when considering future labour market participation, since haematological malignancy subtype was found to be strongly associated with both return to work rates and risk of disability pension [Citation4,Citation9]. According to haematological malignancy subtype, these patients had a two to 12-fold higher risk of being granted disability pension compared to a reference cohort without a history of haematological malignancies. Patients with indolent subtypes of haematological malignancies tended to have the highest relative risks of disability pension [Citation4].
In Denmark, the social security system is obligated to support a person financially through public transfer payments if the person is unable to work due to physical or mental disability. Disability pension is granted if the work capacity is permanently reduced to an extent that makes return to work unlikely. All options available for improving labour market participation must have been exhausted before disability pension is granted. An option that is considered before disability pension is to give wage subsidies to employers for hiring the long-term disabled, known as the Danish Flexjob Scheme. In a wage-subsidised (WS) job, the employee has reduced working hours and special job tasks, taking into account the reduced work capacity. To be granted WS employment, the person's work capacity must be reduced to a level that permanently prevents him or her from having a non-wage-subsidised job [Citation10,Citation11].
To the best of our knowledge, no studies have investigated if the Danish Flexjob scheme is widely applied among patients diagnosed with haematological malignancies. Based on our previous studies, it is hypothesised that patients with indolent subtypes of haematological malignancies have the poorest labour market prognosis. However, to give a full picture of the extent of work incapacity among these patients, an identification of the extent of WS employment within the different subtypes of haematological malignancies is necessary.
Therefore the present study aimed to compare the risk of being granted WS employment as a result of permanently reduced work capacity among patients diagnosed with haematological malignancies to an age- and gender-matched reference cohort without a history of these malignancies, and to determine if relative risks differ between haematological malignancy subtypes.
Material and methods
The study period proceeded from 1 January 2000 to 26 February 2012 within the entire Danish population of approximately 5.6 million inhabitants. In Denmark, a considerable amount of health-related information is recorded in national population-based registers, and linkage of register data at the individual level is possible by means of a unique civil registration number assigned to all Danish residents [Citation12]. The data used in this study were obtained from these national registers.
Eligible persons were diagnosed with a haematological malignancy at the age of 19–55 years in Denmark during the period from 1 January 2000 to 31 December 2007. Disability pensioners, WS employees and emigrants were excluded. Haematological malignancies were divided into the following subtypes: Hodgkin lymphoma, diffuse large B-cell lymphoma, follicular lymphoma, multiple myeloma, acute myeloid/lymphoid leukaemia, chronic myeloid leukaemia, chronic lymphoid leukaemia and others. Each patient was individually matched on gender and date of birth to 10 persons without a history of haematological malignancies. The individuals in the reference cohort were assigned the same date of diagnosis as the patient to whom they were matched. The patient cohort and the reference cohort have been described in detail previously [Citation4].
Outcome
At inclusion, all individuals were potentially active members of the labour market. The different work-related pathways in the study are illustrated in . The main outcome was WS employment as a result of permanently reduced work capacity. Permanent exits from labour market like disability pension, anticipatory retirement pension and old age pension were considered competing events to this outcome. During the entire study period it was possible to retire due to age at 65 years in Denmark and there was an anticipatory retirement scheme from the age of 60 years. Individuals in both cohorts were followed from date of diagnosis until they were either granted WS employment, disability pension, old age pension or anticipatory pension, emigration, death or until 26 February 2012, whichever came first.
Figure 1. The pathways of permanently partly or completely exit from the labour market. Individuals who were employed, students, unemployed, sickness absent or on social security were considered to be potentially active members of the labour market. They were followed until they were either granted wage-subsidised employment, emigration, disability pension, old age pension or anticipatory pension, death or until 26 February 2012, whichever came first.
Information on labour market participation was obtained from the Danish Register for Evaluation of Marginalisation (DREAM). DREAM contains information on all public transfer payments administered by Danish ministries and municipalities for Danish residents on a weekly basis since 1991. The register is based on data from the Danish Ministry of Employment, the Danish Ministry of Education, the Danish Civil Registration System and SKAT (the Danish Tax Authority) [Citation13].
Statistics
Using generalised linear regression models for pseudo observations [Citation14], age- and gender-adjusted relative cumulative risks (RR) of being granted WS employment and associated 95% confidence intervals (CI) two, four and six years after diagnosis were estimated for the eight subgroups of haematological malignancies compared to the reference cohort. In a previous study we found that the cancer disease modified the effect of comorbidity, social-economic factors and previous history of sickness leave on labour market participation among patients diagnosed with haematological malignancies (compared to a reference cohort) [Citation4].Therefore, adjustments were only made for age and gender.
Wald tests were used to test if the relative risks differed between subgroups, and to test the overall association between diagnosis subtype and the risk of being granted WS employment as a result of permanent reduced work capacity. Death, disability pension, anticipatory pension, and old age pension were considered competing events in all the analyses.
Results
A total of 3616 patients between 19 and 55 years of age were diagnosed with haematological malignancies in Denmark for the first time between 2000 and 2007; and hence initially the reference cohort consisted of 36 160 individuals.
After excluding disability pensioners, WS employees and emigrants, a total of 3194 (88%) patients and 28 627 (79%) reference individuals were included in the study. The inclusion process has previously been described [Citation4].
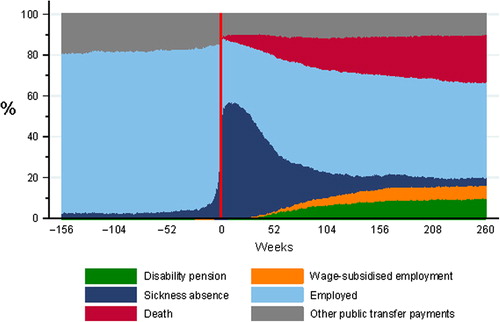
A week-by-week overview of the proportion of public transfer payments in the patient cohort from three years before diagnosis until five years after is given in . Sickness absence increased immediately after diagnosis followed by increasing return to work proportions during the following years. The proportion of patients granted disability pension and WS employment increased during the years after diagnosis. Results on the course of return to work and disability pension in this cohort have been published previously [Citation4,Citation9].
Figure 2. Overview of the proportion of social transfer payments in the patient cohort (N = 3194).
Subtypes of haematological malignancies
A total of 310 (10%) patients had their work capacity permanently reduced to an extent that they were granted WS employment during the follow-up period. The highest proportion was found for patients with multiple myeloma (18%) and chronic myeloid leukaemia (17%), and the lowest for patients with Hodgkin lymphoma (5%). In the reference cohort, a total of 795 (3%) individuals were granted WS employment during the follow-up period ().
Table I. Reference and patient cohort outcome stratified by subtype of haematological malignancy.
presents the results of age- and gender-adjusted analyses of the risk of being granted WS employment due to permanently reduced work capacity according to subtype of haematological malignancy compared to the reference cohort. Both two, four and six years after diagnosis, haematological malignancy subtype was significantly associated with being granted WS employment (p < 0.001), and relative risks differed significantly between the eight subgroups (p < 0.001). These associations were strongest two years after diagnosis and became slightly weaker year by year, as the risk of being granted WS employment increased in the reference cohort with increasing age. The relative risks were lowest for patients with Hodgkin lymphoma and four years after diagnosis this subgroup had a 2.5-fold higher risk of being granted WS employment than the reference cohort (RR 2.47, 95% CI 1.46–4.16). The highest risk was found for patients with chronic myeloid leukaemia, and four years after diagnosis, the risk of being granted WS employment was more than 10-fold higher for this patient group compared to the reference cohort (RR 10.83, 95% CI 7.15–16.40). The second highest relative risk was found among patients diagnosed with multiple myeloma (RR 8.48, 95% CI 6.22–11.56). At this time-point, the other subgroups of haematological malignancies had three- to five-fold higher risks of having their work capacity permanently reduced to an extent that they were granted WS employment compared to the reference cohort.
Table II. Age- and gender-adjusted cumulative relative risks of wage-subsidised employment two, four and six years after diagnosis for haematological malignancy subtypes compared with the reference cohort.
Discussion
In this nationwide register-based cohort study we found that compared to a reference cohort, patients with eight subtypes of haematological malignancies (Hodgkin lymphoma, diffuse large B-cell lymphoma, follicular lymphoma, multiple myeloma, acute myeloid/lymphoid leukaemia, chronic myeloid leukaemia, chronic lymphoid leukaemia and others) had a higher risk of having their work capacity permanently reduced to an extent that they were granted WS employment. The relative risks differed considerably between haematological malignancy subtypes, and the highest were found for patients with chronic myeloid leukaemia.
Chronic myeloid leukaemia usually occurs after the age of 40 years and is in most cases incurable. Symptoms are often sparse at time of diagnosis. Biological therapy [tyrosine kinase inhibitors (TKIs)], which is administered as oral tablets, effectively delays disease progression and has improved overall survival considerably (5-year survival rate 90%) [Citation15]. Due to this effective treatment scheme, it is somehow surprising that this patient group had the highest relative risks of having their work capacity permanently reduced to a level that they were granted WS employment. In general, when interpreting the results of this study, it is though important to have in mind that the proportion of death differed widely between the subgroups. The proportion at risk of work disability was therefore higher in those subgroups with a high survival rate than those with lower survival rates. The same concern is valid for the proportion of disability pension, which also differed markedly between haematological malignancy subgroups (). This does, however, not seem to be the only explanation of our findings, as the relative risks of WS employment were lower than for chronic myeloid leukaemia in both patients with follicular lymphomas and chronic lymphoid leukaemia. The proportion of death and disability pension was similar in these three subgroups, and like chronic myeloid leukaemia, follicular lymphomas and chronic lymphoid leukaemia are usually incurable diseases with a chronic course.
In Denmark, the Flexjob scheme has been found to raise the employment probability among long-term disabled with reduced work capacity by 33% points [Citation16]. Thus, in spite of permanently reduced work capacity, the Flexjob scheme can provide patients with chronic myeloid leukaemia with the possibility of keeping an affiliation to the labour market. For the same reason, WS employment should not entirely be seen as a negative event.
However, being granted WS employment does mean that a person's functional level is impaired considerably. In this present study, patients diagnosed with chronic myeloid leukaemia had a 10-fold higher risk of being granted WS employment than the reference cohort. We do not know the mechanism behind this finding. Symptoms and late effects from disease and treatment could play a role, as previous studies have shown that a considerable proportion of patients diagnosed with chronic myeloid leukaemia experience reduced quality of life and symptoms like fatigue, depression, anxiety, and musculoskeletal pain [Citation17–20].
We did not have information regarding treatment type. But during the study period, first choice of medication for the largest part of the patients with chronic myeloid leukaemia was Imatinib (a TKI). It should, however, be emphasised that several other types of treatment could have been used as second line therapies (often other TKIs) in patients not responding to first line treatment or in patients experiencing side effects [Citation15]. Thus, the present study can not be used to determine if there are differences between the side effects of different TKIs, as found in other studies [Citation17,Citation20]. Allogeneic bone marrow transplantation is performed among some patients diagnosed with chronic myeloid leukaemia (16% in this present study). This could affect the risk of WS employment, since this treatment regimen is associated with several chronic late effects [Citation21]. However, only one of the patients diagnosed with chronic myeloid leukaemia in this present study was granted WS employment following allogeneic bone marrow transplantation, and therefore use of this treatment scheme cannot explain our results.
Due to improved cancer treatment the survival of patients beyond cancer diagnosis has increased markedly during recent years. Therefore more focus on rehabilitation of these patients is needed in order to secure high quality of life and optimal degree of life functioning following treatment [Citation22,Citation23]. The World Health Organization defines rehabilitation of people with disabilities as a process aimed at enabling them to reach and maintain their optimal physical, sensory, intellectual, psychological and social functional levels [Citation24]. In order to provide feasible rehabilitation of patients with chronic myeloid leukaemia, the reason for the reduced work capacity should be examined, and interventions for preventing it should be studied. If impairment of functional level is non-preventable, and found to be a natural cause of disease and treatment, then WS employment must be seen as a reasonable solution for patients diagnosed with chronic myeloid leukaemia to maintain their optimal level of work ability.
Patient with multiple myeloma also had high relative risks of being granted WS employment due to permanently reduced work capacity. In a previous study we found that this patient group had a 12-fold higher risk of disability pension compared to the general population [Citation4]. In all, these two studies document that a diagnosis of multiple myeloma leads to considerably poor labour market prognosis, which might be explained by the chronic and progressive nature of this disease.
The lowest relative risks of being granted WS employment were found for patients with Hodgkin lymphoma. In a previous study we also found that this subgroup had the lowest risk of disability pension among patients diagnosed with haematological malignancies [Citation4]. One of the reasons for the relatively good labour market prognosis in this group is probably that in contrary to chronic myeloid lymphoma and multiple myeloma, Hodgkin lymphoma most often is a curable disease. The prognosis is good even though it depends on the stage of disease. Treatment consists of chemotherapy and radiotherapy and is usually completed within 3–6 months. The five-year survival rate for this subtype of haematological malignancies is 85% [Citation25]. Furthermore, this subgroup have the lowest median age among patients diagnosed with haematological malignancies (). This probably also enhance labour market prognosis. Based on the curable course of Hodgkin lymphomas, it is notable that even though this group of patients had the lowest relative risks of WS employment, six years after diagnosis the risk was still more than twice as high than in the reference cohort. This may indicate that the patients experience long-term late effects following treatment.
Strengths and limitations
One of the strengths of our study is the use of population-based registries with complete follow-up. This enabled us to describe the risk of being granted WS employment due to permanently reduced work capacity among patients with haematological malignancies in a relatively large unselected population. The design was prospective allowing us to evaluate temporal associations, and all patients between 19 and 55 years of age diagnosed between 2000 and 2007 were eligible for inclusion. The fact that information on all variables was obtained through registers reduced the risk for recall and selection bias.
It would though have been relevant to perform analyses stratified on, for example, age groups and social position in order to investigate if the associations differed according to these factors. However, due to the limited number of individuals in each haematological malignancy subgroup, we were not able to make these stratifications. Furthermore, it would have been relevant to include information on relapse of disease in the analyses, since this has been found to impact on labour market prognosis in previous studies [Citation26]. Unfortunately we did not have access to data on this information.
Future studies should focus on specific patient groups, such as patients with chronic myeloid leukaemia, in order to obtain more knowledge on mechanisms behind the relatively high risk of being granted WS employment in this patient group. Furthermore, studies with focus on other aspects of daily living for these patients are needed in order to investigate, if the diseases have further consequences on their function and everyday life.
Conclusion
In conclusion, patients with all eight subtypes of haematological malignancies had a higher risk of having their work capacity permanently reduced to an extent that they were granted WS employment compared to the reference cohort. The relative risks differed between the subtypes of haematological malignancies, and were highest for patients with chronic myeloid leukaemia.
The results of this study imply that clinicians should be aware that the risk of permanently reduced work capacity differs between subtypes of haematological cancer. This knowledge is important in order to initiate early targeted rehabilitation interventions aimed at maintaining appropriate labour market participation if possible. Even though effective treatment exists for patients with chronic myeloid leukaemia, a considerable proportion experience impaired function to a level that prevents them from having an ordinary job. Further research on the mechanisms behind this result is needed
Declaration of interest: This publication was supported by Cost Action IS1211 CANWON. This work has been supported by grants from The Danish Cancer Society (grant number R56-A3231), Aarhus University Hospital, The Health Insurance Foundation (grant number 2012B026), Public Health and Quality Improvement, Central Denmark Region. The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
- Carlsen K, Oksbjerg Dalton S, Frederiksen K, Diderichsen F, Johansen C. Cancer and the risk for taking early retirement pension: A Danish cohort study. Scand J Public Health 2008;36:117–25.
- Syse A, Tretli S, Kravdal O. Cancer’s impact on employment and earnings – a population-based study from Norway. J Cancer Surviv 2008;2:149–58.
- Torp S, Nielsen RA, Gudbergsson SB, Fossa SD, Dahl AA. Sick leave patterns among 5-year cancer survivors: A registry-based retrospective cohort study. J Cancer Surviv 2012;6:315–23.
- Horsboel TA, Nielsen CV, Andersen NT, Nielsen B, de Thurah A. Risk of disability pension for patients diagnosed with haematological malignancies: A register-based cohort study. Acta Oncol 2014:53:724–34.
- Park JH, Park EC, Park JH, Kim SG, Lee SY. Job loss and re-employment of cancer patients in Korean employees: A nationwide retrospective cohort study. J Clin Oncol 2008;26:1302–9.
- Roelen CA, Koopmans PC, Groothoff JW, van der Klink JJ, Bultmann U. Sickness absence and full return to work after cancer: 2-year follow-up of register data for different cancer sites. Psychooncology 2011;20:1001–6.
- Short PF, Vasey JJ, Tunceli K. Employment pathways in a large cohort of adult cancer survivors. Cancer 2005;103: 1292–301.
- de Boer AG, Verbeek JH, Spelten ER, Uitterhoeve AL, Ansink AC, de Reijke TM, et al. Work ability and return-to-work in cancer patients. Br J Cancer 2008;98:1342–7.
- Horsboel TA, Nielsen CV, Nielsen B, Jensen C, Andersen NT, de Thurah A. Type of hematological malignancy is crucial for the return to work prognosis: A register-based cohort study. J Cancer Surviv 2013;7:614–23.
- Bekendtgørelse om Fleksjob, BEK nr 978 af 05/08/2013.
- Lov om Social Pension, LBK nr 1005 af 19/08/2010.
- Pedersen CB. The Danish Civil Registration System. Scand J Public Health 2011;39(7 Suppl):22–5.
- Hjollund NH, Larsen FB, Andersen JH. Register-based follow-up of social benefits and other transfer payments: Accuracy and degree of completeness in a Danish interdepartmental administrative database compared with a population-based survey. Scand J Public Health 2007;35: 497–502.
- Parner ET, Andersen PK. Regression analysis of censored data using pseudo-observations. Stata J 2010;10:408–422.
- Baccarani M, Cortes J, Pane F, Niederwieser D, Saglio G, Apperley J, et al. Chronic myeloid leukemia: An update of concepts and management recommendations of European LeukemiaNet. J Clin Oncol 2009;27:6041–51.
- Gupta ND, Larsen M. Evaluating labour market effects of wage subsidies for the disabled – The Danish Flexjob Scheme. Copenhagen: The Danish National Centre for Social Research (SFI); 2010.
- Cella D, Nowinski CJ, Frankfurt O. The impact of symptom burden on patient quality of life in chronic myeloid leukemia. Oncology 2014;87:133–47.
- Efficace F, Baccarani M, Breccia M, Cottone F, Alimena G, Deliliers GL, et al. Chronic fatigue is the most important factor limiting health-related quality of life of chronic myeloid leukemia patients treated with imatinib. Leukemia 2013;27:1511–9.
- Hamerschlak N, de Souza C, Cornacchioni AL, Pasquini R, Tabak D, Spector N, et al. Quality of life of chronic myeloid leukemia patients in Brazil: Ability to work as a key factor. Support Care Cancer 2014;22:2113–8.
- Phillips KM, Pinilla-Ibarz J, Sotomayor E, Lee MR, Jim HS, Small BJ, et al. Quality of life outcomes in patients with chronic myeloid leukemia treated with tyrosine kinase inhibitors: A controlled comparison. Support Care Cancer 2013;21:1097–103.
- Syrjala KL, Martin PJ, Lee SJ. Delivering care to long-term adult survivors of hematopoietic cell transplantation. J Clin Oncol 2012;30:3746–51.
- Dalton SO, Bidstrup PE, Johansen C. Rehabilitation of cancer patients: Needed, but how? Acta Oncol 2011;50:163–6.
- Dalton SO, Johansen C. New paradigms in planning cancer rehabilitation and survivorship. Acta Oncol 2013;52:191–4.
- World Health Organization. World report on disability. Geneva: World Health Organization; 2011.
- Jansen L, Castro FA, Gondos A, Krilaviciute A, Barnes B, Eberle A, et al. Recent cancer survival in Germany: An analysis of common and less common cancers. Int J Cancer Epub 2014 Nov 7.
- Damkjaer LH, Deltour I, Suppli NP, Christensen J, Kroman NT, Johansen C, et al. Breast cancer and early retirement: Associations with disease characteristics, treatment, comorbidity, social position and participation in a six-day rehabilitation course in a register-based study in Denmark. Acta Oncol 2011;50:274–81.