
Abstract
Background The purpose of this study is to elucidate incidence, mortality, survival, and prevalence of kidney cancer in elderly persons compared with younger persons in Denmark.
Material and methods Cancer of the kidney was defined as ICD-10 code DC 64. Data derived from the NORDCAN database with comparable data on cancer incidence, mortality, prevalence and relative survival in the Nordic countries, where the Danish data were delivered from the Danish Cancer Registry and the Danish Cause of Death Registry with follow-up for death or emigration until the end of 2013.
Results The proportion of patients diagnosed with kidney cancer over the age of 70 years has decreased from 43% in 1980 to 32% in 2012 in men and remained almost constant in women, around 50%. Incidence rates were at least five times higher in men aged 70 years more but there was no particular trend with time. In men aged less than 70 years, the incidence rates started increasing around 2000. The incidence rates were lower in women but with a similar pattern as in men. Mortality rates remained stable over time in persons aged 70 years or more while they decreased with time in younger women. Both the one- and the five-year relative survival increased steadily over time for all age groups but the survival was lower for patients aged 70 years or more than for younger patients. The prevalence increased three times from 1559 patients being alive after kidney cancer in1980 to 4713 in 2012.
Conclusion A challenge in managing kidney cancer in the elderly is to establish interdisciplinary collaborations between different specialties, such as surgeons, clinical oncologists, and geriatricians to be able to deliver the best possible care in the future.
The incidence of kidney cancer increased dramatically during the past two decades in the Nordic countries [Citation1] as well in the US and Western Europe [Citation2]. This increase reflects mainly smaller tumors and is thought to be due to increased use of abdominal imaging, such as computed tomography (CT) and renal ultrasound [Citation3,Citation4].
A number of risk factors have been identified for developing kidney cancer, such cigarette smoking, obesity, hypertension, and antihypertensive medication, but the etiology remains unknown [Citation5]. There are believed to be three major inherited forms of renal cell cancer, von Hippel-Lindau-associated, familial clear cell, and hereditary papillary renal cell carcinoma (HPRC), which together account for a small proportion of kidney cancers. All three familial syndromes are inherited dominantly and tend to arise at a much younger age than sporadic cases [Citation6].
The current guidelines for the treatment of kidney cancer cover all age groups without taking into account the specific problems faced by elderly patients, such as significant comorbid conditions and polypharmacy [Citation7]. The gold standard for managing kidney cancer is a radical or partial nephrectomy. However, minimally invasive/percutaneous nephron sparing techniques have been developed in the last decade to manage smaller renal masses, including thermal ablation via radiofrequency and cryotherapy [Citation8]. It is hoped that such minimally invasive techniques may lead to more elderly persons being offered curative surgery.
The purpose of this study is to elucidate incidence, mortality, survival, and prevalence of kidney cancer in elderly persons compared with younger persons in Denmark.
Material and methods
Cancer of the kidney was defined as ICD-10 code DC 64. A more detailed description of the materials and methods appear elsewhere [Citation9]. In brief, data were derived from the NORDCAN database, which has comparable data on cancer incidence, mortality, prevalence, and relative survival rates in the Nordic countries, where the Danish data were derived from the Danish Cancer Registry and the Danish Cause of Death Registry with follow-up for death or emigration until the end of 2013. This study focuses on the elderly population with age categorized as 0–69, 70–79, 80–89 and 90 + years.
For incidence and mortality, age group-specific numbers and rates per 100 000 person years are shown in tables and graphs with calendar periods for time of diagnosis 1978–1982, 1988–1992, 1998–2002, 2003–2007, 2010, 2011 and 2012. Prevalence is defined as the number of cancer patients (including cured patients as well) with that specific diagnosis still alive and is shown in tables by the end of 1980, 1990, 2000, 2005, 2010, 2011 and 2012.
Sex- and age-specific one- and five-year relative survival proportion ratios were calculated for each of the diagnostic groups for the age groups 0–69, 70–79, 80–89 and 90 + years and for the five-year periods of diagnosis 1968–1972, 1973–1977, …, 2003–2007 and 2008–2012. Relative survival for a group of cancer patients is calculated as the observed overall survival (where all causes of death are considered events) divided by the expected survival for a group from the Danish population with the same age, gender, and year of birth. Actuarial method is used for observed survival and Ederer II method for expected survival [Citation10]. Relative survival can be interpreted as the survival if the cancer was the only cause of death. For the most recent period, 2008–2012, not all patients can be followed up for death in five years and so we used hybrid methods where we supplemented the survival experience from cancer patients diagnosed in earlier years [Citation11].
Results
The average annual number of new cases of kidney cancer increased in men from 267 in 1980 to 467 in 2012 and in women from 216 to 264, corresponding to an increase in men by 75% and 22% in women (). The proportion of patients diagnosed over the age of 70 years has decreased from 43% in 1980 to 32% in 2012 in men and remained more or less constant in women, around 50%. The average annual number of deaths from kidney cancer remained stable in men, 166 in 1980 and 174 in 2012, but decreased in women from 152 in 1980 to 115 in 2012 (). About 45% of deaths occurred in men aged more than 70 years while in women, the proportion increased over time reaching 71% in 2012.
Table I. Average annual number of new kidney cancers in Denmark, 1980–2012.
Table II. Average annual number of deaths from kidney cancer in Denmark, 1980–2012.
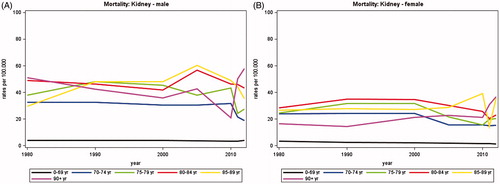
Adjusting for changes in population size and age, illustrates that the incidence rates were at least five times higher in men aged 70 years more but that there was no particular trend with time. In younger men aged less than 70 years, the incidence rates started increasing around 2000. The incidence rates were lower in women but with a similar pattern as in men. The mortality rates were also higher, about three times, in persons aged 70 years or more than in younger patients (). The rates remained stable over time in men and women aged 70 years or more while they decreased with time in younger women.
Figure 1. Incidence rates of kidney cancer in Denmark, 1980–2012, by age group. A. Males, B. Females.
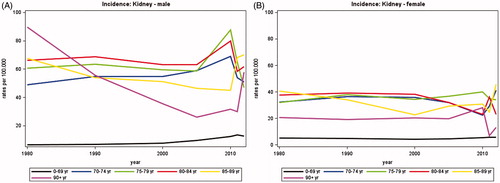
Figure 2. Mortality rates from kidney cancer in Denmark, 1980–2012, by age group. A. Males, B. Females.
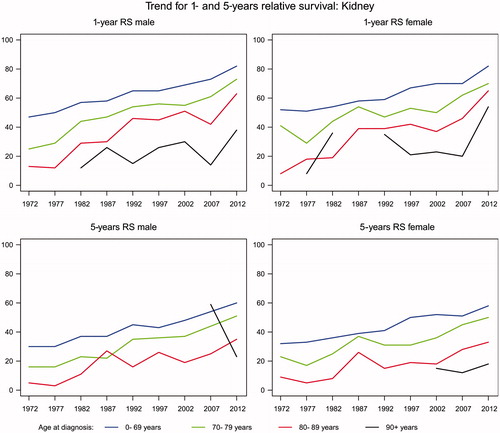
Both the one- and the five-year relative survival increased steadily over time for all age groups but the survival was lower for patients aged 70 years or more than for younger patients (). The one-year relative survival was 82% and the five-year relative survival around 60% in patients aged less than 70 years in 2008–2012 and the equivalent figures for those aged 70–89 were in the order of 73–63% and 50–35%. There were too few patients over 90 years to provide meaningful figures.
Figure 3. Trend for 1- 5 years relative survival after kidney cancer in Denmark.
The prevalence increased three times from 1559 patients being alive after kidney cancer in 1980 to 4713 in 2012 (). The proportion of persons aged 70 years or more remained quite constant around 39% in men and 50% in women.
Table III. Annual number of persons alive with kidney cancer in Denmark by 31 December, 1980–2012.
Discussion
From 1980 to 2012 incidence rates of kidney cancer have remained fairly constant in persons aged 70 years or more, but increased in younger persons (less than 70 years) since 2000. It has not been accompanied by an equivalent increase in the mortality rates. There are several possible reasons for these differences. One could be due to lifestyle differences, such as smoking. There is a marked difference in tobacco consumption in the Nordic countries with higher rates in the elderly compared to younger patients. Other examples of higher risk behaviors in the elderly population include higher rates of obesity and alcohol consumption. Sweden, as opposed Denmark and other European countries, since 1979 has seen a decrease in the incidence of kidney cancer and median tumor size. In Sweden, there has been an increased use of CT and ultrasound scans, which may account for the observation that tumor cases are being detected at an earlier stage. There has also been a decrease in smoking (35–17% for men and 29–19% for women). Moreover, the prevalence of being overweight or obese in Sweden is low compared to other countries. The observed differences in overall survival rates in the Nordic countries might, therefore, be due to differences in lifestyles, which have been preferentially adopted by the young rather than the more elderly population. This phenomenon has also been observed in other malignancies, such as lung, colon, and bladder cancers [Citation8].
Surgical aspects
In the present study the elderly over 70 years represented more than one-third of all kidney cancer patients and there is no definitive treatment guideline for this group. The challenge for the surgeon facing the elderly patient is getting validated methods to assess the patient’s functional and cognitive level, their nutritional status, comorbidities, and the impact of polypharmacy, all of which are common in the elderly. Therefore, interdisciplinary collaborations between different specialties, such as surgeons, clinical oncologists, and geriatricians are very important. This is highlighted by a report from Brassart et al. that demonstrated relatively high medical complication rates of 31%, surgical complications in 16%, and 6% mortality among patients over age 80 years undergoing a radical nephrectomy [Citation12].
Oncological aspects
The systemic treatments for metastatic kidney cancer have changed over the last decade from mainly immunotherapy towards targeted therapy with thyrosine kinase inhibitors (TKIs) and inhibitors of the mammalian target of rapamycin (mTOR-inhibitors). More patients with metastatic kidney cancer are now being offered systemic treatment and during 2006–2010, an improved overall survival rate was seen in a Danish complete national cohort of patients [Citation13]. In a univariate analysis, there was no difference in median overall survival for patients comparing those 63 years or younger to those over 63 years. Another retrospective database study showed no differences for patients who were 75 years or older regarding median treatment duration, median survival, or response rate [Citation14]. In a similar database study, there was no age difference in patients who were eligible or ineligible for clinical trials [Citation15]. In general, elderly patients are included in metastatic kidney cancer clinical trials, but age-specific data are missing regarding their toxicity, comorbidity, drug interactions, quality of life, and dose reduction. There is no recommendation of dose modification for elderly patients with metastatic kidney cancer [Citation16]. However, the healthcare costs of treating patients 65 years or older might be higher [Citation17]. More data focusing on elderly patients with metastatic kidney cancer treated with targeted therapies are clearly needed, but TKI or mTOR treatments should be offered to elderly patients on the same terms as younger patients.
In addition, particularly in the last 5 − 10 years, there have been substantial improvements in supportive care therapy for patients with metastatic kidney cancer, which would also tend to improve survival even for this group with the most advanced disease [Citation3,Citation4].
Conclusion
A challenge in managing kidney cancer in the elderly is to establish interdisciplinary collaborations between different specialties, such as surgeons, clinical oncologists, and geriatricians to be able to deliver the best possible care in the future.
Acknowledgments
We thank Niels Christensen and Anne Mette T. Kejs, Danish Cancer Society, Department of Documentation & Quality, for making the tabulations of incidence, mortality and prevalence, calculation of relative survival and trend graphs. The authors report no conflicts of interest.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
- Engholm G, Ferlay J, Christensen N, Bray F, Gjerstorff ML, Klint A, et al. NORDCAN – a Nordic tool for cancer information, planning, quality control and research. Acta Oncol 2010;49:725–36.
- Chow WH, Devesa SS, Warren JL, Fraumeni JF JrJr. Rising incidence of renal cell cancer in the United States. Jama 1999;281:1628–31.
- Janzen NK, Kim HL, Figlin RA, Belldegrun AS. Surveillance after radical or partial nephrectomy for localized renal cell carcinoma and management of recurrent disease. Urol Clin North Am 2003 Nov;30:843–52.
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, Murray T, et al. Cancer statistics, 2008. CA Cancer J Clin 2008;58:71–96.
- Lipworth L, Tarone RE, Lund L, Mclaughlin JK. Epidemiologic characteristics and risk factors for renal cell cancer. Clin Epidemiol 2009;1:33–43.
- Mclaughlin JK, Lipworth L, Tarone RE, William JB. Renal Cancer. Cancer Epidemiology and Prevention. David Schottenfeld and Joseph F. Fraumeni. Oxford University Press, Oxford Scholarship Online 2006. http://www.oxfordscholarship.com/view/10.1093/acprof:oso/978019-5149616.001.0001/acprof-9780195149616-chapter-57
- Ljungberg B, Bensalah K, Canfield S, Dabestani S, Hofmann F, Hora M, et al. EAU Guidelines on Renal Cell Carcinoma: 2014 Update. Eur Urol 2015;67:913–24.
- Lyrdal D, Aldenborg F, Holmberg E, Peeker R, Lundstam S. Kidney cancer in Sweden: a decrease in incidence and tumour stage, 1979–2001. Scand J Urol 2013;47:302–10.
- Ewertz M, Christensen K, Engholm G, Hansen O, Kejs AMT, Lund L, et al. Trends in cancer in the elderly population in Denmark, 1980-2012. Acta Oncol. (In press).
- Dickman PW, Sloggett A, Hills M, Hakulinen T. Regression models for relative survival. Stat Med 2004;23:51–64.
- Harris RJ, Bradburn MJ, Deek JJ, Harbord RM, Altman DG, Sterne JA. Fixed- and random effects meta-analysis. Stata J 2008;8:3–28.
- Brassart E, Lebdai S, Berger J, Traore S, Bernhard JC, Fardoun T, et al. Overall mortality after radical nephrectomy in patients aged over 80 years with renal cancer: a retrospective study on preoperative prognostic factors. Int J Urol 2012;19:626–32.
- Soerensen AV, Donskov F, Hermann GG, Jensen NV, Petersen A, Spliid H, et al. Improved overall survival after implementation of targeted therapy for patients with metastatic renal cell carcinoma: results from the Danish Renal Cancer Group (DARENCA) study-2. Eur J Cancer 2014;50:553–62.
- Khambati HK, Choueiri TK, Kollmannsberger CK, North S, Bjarnason GA, Vaishampayan UN, et al. Efficacy of targeted therapy for metastatic renal cell carcinoma in the elderly patient population. Clin Genitourin Cancer 2014;12:354–58.
- Heng DY, Choueiri TK, Rini BI, Lee J, Yuasa T, Pal SK, et al. Outcomes of patients with metastatic renal cell carcinoma that do not meet eligibility criteria for clinical trials. Ann Oncol 2014;25:149–54.
- Quivy A, Daste A, Harbaoui A, Duc S, Bernhard JC, Gross-Goupil M, et al. Optimal management of renal cell carcinoma in the elderly: a review. Clin Interv Aging 2013;8:433–42.
- Hagiwara M, Hackshaw MD, Oster G. Economic burden of selected adverse events in patients aged ≥65 years with metastatic renal cell carcinoma. J Med Econ 2013;16:1300–6.