Abstract
Objectives. To estimate the possible economic benefit of a sequential testing strategy with NT-proBNP to reduce the number of echocardiographies.
Methods. Retrospective study in a third-party payer perspective. The costs were calculated from three Swedish counties: Blekinge, Östergötland, and Uppland. Two cut-off levels of NT-proBNP were used: 400 and 300 pg/mL. The cost-effectiveness of the testing strategy was estimated through the short-term cost avoidance and reduction in demand for echocardiographies.
Results. The estimated costs for NT-proBNP tests and echocardiographies per county were reduced by 33%–36% with the 400 pg/mL cut-off and by 28%–29% with the 300 pg/mL cut-off. This corresponded to a yearly cost reduction of approximately €2–5 million per million inhabitants in these counties.
Conclusion. The use of NT-proBNP as a screening test could substantially reduce the number of echocardiographies in the diagnostic work-up of patients with suspected cardiac failure, as well as the associated costs.
Introduction
Heart failure (HF) is a major challenge for the health care system (Citation1). It is the most common diagnosis among elderly inpatients, and it affects a large number of patients (Citation2). Approximately 14 million persons suffer from heart failure in Europe, and 4.8 million US citizens are estimated to have congestive heart failure (Citation3). HF is a complex syndrome that is caused by abnormalities of cardiac function or structure that impair the ability of the heart to fill or eject blood (Citation4). HF is expensive with average HF admission costs of $7,000–13,000 (Citation5) and associated with a significant mortality (Citation6). The death rates within 1 month are between 7% and 15% (Citation7). The number of HF patients is expected to grow as well as the costs as the population ages with increased life expectancy.
Echocardiography is used to diagnose cardiovascular diseases, and it is one of the most widely used diagnostic tests for HF (Citation8,9). An echocardiogram is labor-intensive and thus expensive in comparison with biochemical markers. To alleviate the cost of echocardiograms, investigators have been examining disease management strategies that rely on serum or plasma biomarkers that could be used to rule out HF. The most studied HF biomarkers are the B-type natriuretic peptides (BNP) that are synthesized by the left and right atriums in response to cardiomyocyte stretching (Citation10).
The human BNP gene encodes a 108-amino acid prohormone named proBNP (Citation11). ProBNP is cleaved into a biologically active 32-amino acid C-terminal polypeptide (BNP) and a 76-amino acid N-terminal fragment termed NT-proBNP (Citation10). Both these polypeptides are released into the circulation and can be detected in blood samples. There are commercial assays for both BNP and NT-proBNP, and both polypeptides have been shown to be biomarkers for HF. In Sweden, there are more laboratories using NT-proBNP than BNP. Thus, even if the clinical utilization of the two markers is similar, we focused the present study on NT-proBNP.
The aim of the study was to use cost minimization analysis to assess the cost-effectiveness of using NT-proBNP in a sequential testing strategy to minimize the demand for echocardiographies. We used patient data from three counties in Sweden to calculate the cost for a negative NT-proBNP result (rule-out) and compared this with the cost of an echocardiography.
Materials and methods
Patients
The study was performed retrospectively and was based on the initial NT-proBNP test results of 14,346 patients. Data were extracted from the laboratory information system of three clinical chemistry laboratories in Sweden: Blekinge (Karlskrona), Östergötland (Linköping), and Uppland (Uppsala) during the first 6 months of 2011. In total, 14,346 initial NT-proBNP tests were analyzed: 2,355 tests in Blekinge, 5,017 tests in Östergötland, and 6,974 tests in Uppland. Approximately as many men as women were investigated. Sub-categorization of the patients into age groups with 20-year spans from 0 to 100 years of age revealed that, in relation to age distribution, about half of the tests were ordered for patients 61–80 years of age, followed by those for patients 81–100 years of age who constitute about one-third of the tests. The costs of NT-proBNP tests and echocardiography investigations used in this study were retrieved from the official fee schedule of Blekinge County for 2011.
Cost estimates
Two pathways in a sequential testing strategy were compared: echocardiography for all patients with suspected heart failure, versus initial investigation with NT-proBNP to rule out patients without heart failure followed by echocardiography in patients with NT-proBNP results above the respective cut-off levels. The two cut-offs chosen to calculate the costs are presented in . Patients with NT-proBNP results corresponding to ‘HF unlikely' were considered as not having heart failure and no echocardiography should be performed, whereas in patients with NT-proBNP levels corresponding to ‘Uncertain diagnosis' or ‘HF likely', echocardiography should be performed. A cost minimization analysis was performed to calculate the potential cost avoidance and reduction in the number of required echocardiographies, which the sequential testing strategy would achieve in a third-party payer perspective. Costs were expressed in euros at 2011 values (approximate exchange rates: €1 = SEK 9 = US$1.3). The cost of an NT-proBNP test at Blekinge County Hospital in 2011 was €33 and for an echocardiography investigation €236. There was no need to discount costs over time as all measured costs occurred within a short time period.
Table I. NT-proBNP (ng/L) cut-off levels used in the current study.
The cost of direct referral for echocardiography for all patients with suspected HF (n population × price of echocardiography) was compared to the cost of using NT-proBNP tests as initial screening investigation, followed by echocardiography in those patients who initially tested above the cut-offs. To calculate this, each patient was labeled with two different costs according to the two chosen cut-offs. Cost neutrality would occur when the cost of echocardiography equaled the cost of the screening test plus the cost of echocardiography in those patients with screening tests above the cut-off values.
Results
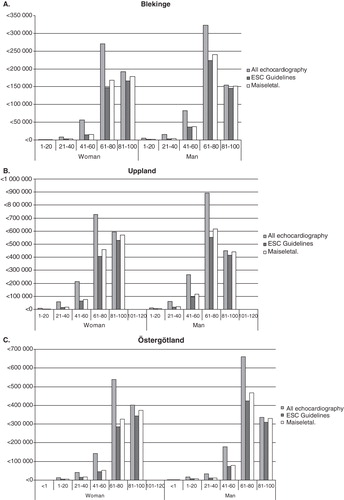
The distribution of test results was very similar in both sexes, and NT-proBNP increased with age as expected. The characteristics of the data set are presented in . Excluding the diagnosis of HF through NT-proBNP screening using the cut-off levels previously mentioned could potentially reduce the costs of diagnostic investigations with up to 30%, depending on the cut-off used. Depending on the cut-off chosen, potential yearly cost savings amounted to approximately €300,000–370,000 in Blekinge, €960,000–1,175,000 in Uppland, and €690,000–840,000 in Östergötland, respectively (). By dividing these numbers with population statistics for the different counties, we could roughly estimate the cost savings per capita to €2–3 per year. Extrapolating these figures on a national level could thus mean potential cost savings for the Swedish health care system corresponding to €19–28 million yearly. Cost estimates for the different screening strategies broken down in different age groups are shown in . This figure shows that a major part of the cost savings was noted among both men and women in the age groups 41–80 years, and to a lesser extent in the younger, and older, patients.
Table II. Cost savings based on the two cut-off levels.
Figure 1. Cost estimates for the different screening strategies broken down according to sex and age groups, A: in Blekinge; B: in Uppland; C: in Östergötland.
Discussion
Heart failure is one of the most important public health problems in the developed world. Despite the introduction of new treatments, heart failure is associated with high costs and poor outcomes with approximately 50% mortality within 5 years of the initial diagnosis (Citation2). The number of HF patients in the United States is nearly 6 million, and the health care cost exceeds $39 billion (Citation12). The incidence of HF increases with age (Citation13). There are also sex-related and race-related differences in HF incidence (Citation14,15). The highest HF incidence is observed in white men > 85 years of age with an annual incidence of 65/1,000 population (Citation12). Many of the patients have non-specific symptoms, which makes it difficult to distinguish HF from other conditions. Thus, many patients have undiagnosed HF. It is important to find these patients and treat them. We thus need a screening assay that can be used to screen for/rule out heart failure. The most widely used test for HF in Sweden is NT-proBNP/BNP, which in national guidelines are recommended to be used as a rule-out test for HF (http://www.socialstyrelsen.se/Lists/Artikelkatalog/Attachments/8592/2008-102-7_20081028.pdf). If the patient has increased levels of NT-proBNP it is recommended that echocardiography is performed, which is considered necessary to establish the diagnosis in HF.
We have compared the cost for using NT-proBNP in a sequential testing strategy to minimize the demand for echocardiographies with the cost for echocardiography testing alone.
We found no significant difference in NT-proBNP requests between male and female patients despite previous reports on higher incidence of HF in white males. With a strict sequential testing strategy, a substantial cost reduction could be achieved (). A major part of the cost savings was noted among both men and women in the age groups 41–80 years, and to a lesser extent in the younger, and older patients. Especially in patients above 80 years of age, fewer individuals are expected to have NT-proBNP levels below the cut-off levels, since NT-proBNP is known to increase with increasing age. Thus, in the oldest group of patients, it may not be cost-efficient to implement a strict sequential testing strategy for diagnosing HF. However, previous studies have shown a great prognostic value for NT-proBNP in all age groups, and it may still be valuable to have NT-proBNP tested at an early stage (Citation16,17). In addition, NT-proBNP testing can be used for monitoring HF treatment, and lately several reports have indicated that NT-proBNP also can be used for guiding treatment of HF towards a target value (Citation16,17).
This study does not take into account that in a minor proportion of patients there may be other reasons for referring to echocardiography investigations, such as abnormal findings in the physical examination (e.g. heart murmurs) or ECG findings, that merit further investigations (Citation18). On the other hand, in our communication with cardiologists, it has often been mentioned that many echocardiographies with normal results could have been avoided by prior testing with NT-proBNP, and unexpected pathological findings in patients with normal NT-proBNP are very rare (personal communication).
Conclusion
In summary, by obtaining patient data from three different counties in Sweden, costs for a negative NT-proBNP result (rule-out), could be compared with the cost of echocardiographies, and we found that a strict sequential testing strategy, minimizing the demand for echocardiographies, could potentially yearly save €2–3 per capita. In Sweden, by strictly implementing this simple screening strategy, the health care system could potentially save €19–28 million per year.
Declaration of interest: This study was financially supported by the Uppsala Hospital Research Fund. Dr Ingvar Rydén is currently employed by Roche Diagnostics as Medical Advisor. The authors alone are responsible for the content and writing of the paper.
Related Research Data
References
- Bhardwaj A, Januzzi JL Jr. Natriuretic peptide-guided management of acutely destabilized heart failure: rationale and treatment algorithm. Crit Pathw Cardiol. 2009;8:146–50.
- Roger VL, Go AS, Lloyd-Jones DM, Adams RJ, Berry JD, Brown TM, Heart disease and stroke statistics–2011 update: a report from the American Heart Association. Circulation. 2011;123:e18–e209.
- On the horizon in heart failure. Lancet. 2011;378:637.
- Brutsaert DL. Cardiac dysfunction in heart failure: the cardiologist's love affair with time. Prog Cardiovasc Dis. 2006;49:157–81.
- Ross JS, Chen J, Lin Z, Bueno H, Curtis JP, Keenan PS, Recent national trends in readmission rates after heart failure hospitalization. Circ Heart Fail. 2010;3:97–103.
- Kociol RD, Horton JR, Fonarow GC, Reyes EM, Shaw LK, O'Connor CM, Admission, discharge, or change in B-type natriuretic peptide and long-term outcomes: data from Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure (OPTIMIZE-HF) linked to Medicare claims. Circ Heart Fail. 2011;4:628–36.
- Schlendorf KH, Kasper EK. Use of novel and conventional biomarkers for management of patients with heart failure. Curr Treat Options Cardiovasc Med. 2011;13:475–88.
- Dokainish H. Combining tissue Doppler echocardiography and B-type natriuretic peptide in the evaluation of left ventricular filling pressures: review of the literature and clinical recommendations. Can J Cardiol. 2007;23:983–9.
- Mant J, Doust J, Roalfe A, Barton P, Cowie MR, Glasziou P, Systematic review and individual patient data meta-analysis of diagnosis of heart failure, with modelling of implications of different diagnostic strategies in primary care. Health Technol Assess. 2009;13:1–207; iii.
- Hino J, Tateyama H, Minamino N, Kangawa K, Matsuo H. Isolation and identification of human brain natriuretic peptides in cardiac atrium. Biochem Biophys Res Commun. 1990;167:693–700.
- Sudoh T, Maekawa K, Kojima M, Minamino N, Kangawa K, Matsuo H. Cloning and sequence analysis of cDNA encoding a precursor for human brain natriuretic peptide. Biochem Biophys Res Commun. 1989;159:1427–34.
- Norton C, Georgiopoulou VV, Kalogeropoulos AP, Butler J. Epidemiology and cost of advanced heart failure. Prog Cardiovasc Dis. 2011;54:78–85.
- Oudejans I, Mosterd A, Bloemen JA, Valk MJ, van Velzen E, Wielders JP, Clinical evaluation of geriatric outpatients with suspected heart failure: value of symptoms, signs, and additional tests. Eur J Heart Fail. 2011;13:518–27.
- Lee KH, Kim JY, Koh SB, Lee SH, Yoon J, Han SW, N-terminal pro-B-type natriuretic peptide levels in the Korean general population. Korean Circ J. 2010;40:645–50.
- Michtalik HJ, Yeh HC, Campbell CY, Haq N, Park H, Clarke W, Acute changes in N-terminal pro-B-type natriuretic peptide during hospitalization and risk of readmission and mortality in patients with heart failure. Am J Cardiol. 2011;107:1191–5.
- Januzzi JL, van Kimmenade R, Lainchbury J, Bayes-Genis A, Ordonez-Llanos J, Santalo-Bel M, NT-proBNP testing for diagnosis and short-term prognosis in acute destabilized heart failure: an international pooled analysis of 1256 patients: the International Collaborative of NT-proBNP Study. Eur Heart J. 2006;27:330–7.
- Januzzi JL Jr, Rehman SU, Mohammed AA, Bhardwaj A, Barajas L, Barajas J, Use of amino-terminal pro-B-type natriuretic peptide to guide outpatient therapy of patients with chronic left ventricular systolic dysfunction. J Am Coll Cardiol. 2011;58:1881–9.
- Kelder JC, Cramer MJ, van Wijngaarden J, van Tooren R, Mosterd A, Moons KG, The diagnostic value of physical examination and additional testing in primary care patients with suspected heart failure. Circulation. 2011;124:2865–73.
- Dickstein K, Cohen-Solal A, Filippatos G, McMurray JJ, Ponikowski P, Poole-Wilson PA, ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2008: the Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2008 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association of the ESC (HFA) and endorsed by the European Society of Intensive Care Medicine (ESICM). Eur Heart J. 2008;29:2388–442.
- McIntyre HF. Leveraging guidelines: understanding heart failure, organizing care. Commentary on the 2010 NICE chronic heart failure guideline update. Eur J Heart Fail. 2011;13:14–17.
- Maisel A, Mueller C, Adams K Jr, Anker SD, Aspromonte N, Cleland JG, State of the art: using natriuretic peptide levels in clinical practice. Eur J Heart Fail. 2008;10:824–39.