Abstract
Atherosclerosis is the most common cause of cardiovascular morbidity in end-stage renal disease (ESRD) patients and carotid intima–media thickness (IMT) is an early independent predictor of atherosclerosis. The aim of this study is to compare the continuous ambulatory peritoneal dialysis (CAPD) and the maintenance hemodialysis (MHD) for carotid IMT in Chinese ESRD patients. A total of 72 CAPD patients, 92 MHD patients, and 50 age- and sex-matched healthy controls were included. Dialysis patients were divided into five subgroups according to dialysis duration: 3–6, 7–12, 13–59, 60–119, and 120–179 months. Carotid IMT and carotid plaques were detected for each patient. The carotid IMT and total plaque detection rate in the CAPD and MHD groups were considerably higher than in the healthy control group (p < 0.01). No significant difference was found in the carotid IMT and total plaque detection rate between the CAPD group and the MHD group (p > 0.05). However, after stratification by dialysis duration, the total carotid IMT in the CAPD subgroup was higher than in the MHD subgroup in dialysis duration of 60–119 and 120–179 months (p < 0.05), and there was no significant difference in the total plaque detection rate between the CAPD and MHD subgroups in the same dialysis duration (p > 0.05). Our study showed that both CAPD and MHD affect carotid IMT in Chinese ESRD patients, and the degree of atherosclerosis in CAPD patients might be higher than that in MHD patients after 5 years of dialysis.
INTRODUCTION
Cardiovascular disease (CVD) is the leading cause of mortality in uremic patients undergoing dialysis.Citation1–3 The mortality rate secondary to CVD is 10–30 times higher in dialysis patients when compared with healthy matched subjects.Citation3–5 Atherosclerosis is the major pathological basis of CVD.Citation3 Carotid intima–media thickness (IMT) is an early independent predictor of atherosclerosis.Citation6,7 Therefore, IMT measurement has been proposed as a method for establishing risk stratification for cardiovascular and cerebrovascular disease events.
The suitable dialysis method for end-stage renal disease (ESRD) patients is a choice between peritoneal dialysis (PD) and hemodialysis (HD). Several studies have tried to assess differences in survival between patients undergoing continuous ambulatory peritoneal dialysis (CAPD) and those undergoing maintenance hemodialysis (MHD); however, the influence of dialysis methods on the survival of patients with ESRD remains controversial.Citation8–14 In addition, studies investigating the effect of the two dialysis methods on carotid IMT in long-term dialysis patients are rare.Citation15
Thus, this study investigates the carotid IMT in Chinese ESRD patients undergoing CAPD or MHD, to determine which dialysis method has a lower occurrence of atherosclerosis. The results of this study could help patients select the appropriate dialysis method, promote long-term survival rate in uremic patients, and finally extend the life span of patients.
SUBJECTS AND METHODS
Subjects
From July 2008 to January 2012, 164 ESRD patients and 50 age- and sex-matched healthy controls were consecutively recruited from the First Affiliated Hospital of Huzhou Teachers College and the First Affiliated Hospital of Zhejiang University. ESRD was diagnosed according to the K/DOQI (Kidney Disease Outcomes Quality Initiative) CKD classification.Citation16 Patients <16 years or >80 years, those with lupus nephritis or diabetic nephropathy, or uremic patients with diabetes mellitus were excluded from the study. Details of accompanying diseases in ESRD patients were as follows: chronic glomerulonephritis (n = 128), hypertension and renal arteriosclerosis (n = 10), polycystic kidney disease (n = 7), obstructive nephropathy (n = 6), hyperuricemic nephropathy (n = 6), multiple myeloma (n = 2), and other chronic kidney diseases (such as Alport syndrome, solitary kidney, and unilateral renal resection; n = 5). ESRD patients were divided into CAPD group (n = 72) and MHD group (n = 92) according to the dialysis method. All patients were using the same dialysis modality for at least 3 months. The median duration of dialysis was 12 months (3–148) in the CAPD group and 20 months (3–179) in the MHD group. Patients in the CAPD and MHD groups were divided into five subgroups according to the dialysis duration: 3–6, 7–12, 13–59, 60–119, and 120–179 months. The study complied with the Declaration of Helsinki (1964). All patients participating in this study gave their written informed consent, the protocol for which was approved by all hospital ethics committees.
Methods
Dialysis methods
CAPD patients used three to five bags of PD solution containing 1.5% glucose per day. Hypercalcemic patients used 1.5% glucose low-calcium PD solution. In patients with less ultrafiltration, PD solution containing 2.5% glucose was used. All the PD solution was made by Baxter Healthcare Limited Company (Guangzhou, China). MHD lasted for 4–5 hours each time with an ordinary dialyzer and polysulfone, and the patient received dialysis two to three times per week. Most of the MHD patients received hemodiafiltration twice a month.
Carotid ultrasonography
The carotid arteries were evaluated in all patients with a color Doppler ultrasonic diagnostic apparatus (HDI 5000, Philips Bothell, WA, USA) using a 7.0–10.0 MHz linear array transducer. Subjects were examined in the supine position. The common carotid artery was examined from the internal extremity of the clavicle and scanned in multiple longitudinal and transverse planes to determine the best view perpendicular to the vessel wall for measuring IMT. The IMT at a site approximately 1 cm proximal to the carotid sinus was measured, and then the averages of three measurements for each side were obtained. The average carotid IMT (a-IMT) and the total carotid IMT (t-IMT) were the arithmetic mean and the sum of right and left averages, respectively. Carotid plaque was defined as the localized IMT of >1 mm and at least 100% increase in the thickness, compared with the adjacent wall segments.Citation17 All ultrasonographic examinations were performed by two experienced sonographers, who were kept unaware of other data.
Clinical data
Patients’ general information included gender, age, dialysis duration, blood pressure, body mass index (BMI), and laboratory parameters [serum creatinine (Scr), urea nitrogen (BUN), total cholesterol (TC), triglycerides (TG), fasting blood glucose (FBG), calcium, phosphorus, albumin, etc.]. Laboratory parameters were measured using an automatic biochemistry analyzer (Hitachi 7600, Hitachi, Tokyo, Japan). The clinical data of CAPD patients were taken in an outpatient clinic during follow-up, and those of MHD patients were taken before dialysis therapy. The factional urea clearance (Kt/V) value of CAPD patients was calculated by the PD ADEQUEST 2.0 software (Baxter Company, Guangzhou, China). The Kt/V value of MHD patients was calculated by the single-compartment model of Daugirdas II formula.Citation18 The average Kt/V value of both the CAPD and MHD groups reached the standard of the K/DOQI guideline.
Statistical Methods
Data were presented as mean ± SD, medians (range), or percentages, as appropriate. Independent samples t-test or one-way ANOVA or nonparametric test was used to compare the quantitative variables between groups, whichever was appropriate. The χCitation2 test was used to compare the qualitative variables. Statistical analyses were performed using SPSS package (SPSS Inc., for Windows, Version 13.0, Chicago, IL, USA). A p-value <0.05 was considered statistically significant.
RESULTS
There were no significant differences among CAPD, MHD, and control groups in gender, age, BMI, TG, FBG, and calcium levels (p > 0.05). The other parameters, such as blood pressure, C-reactive protein (CRP), Scr, BUN, albumin, phosphorus, intact parathormone (i-PTH), and hemoglobin levels, were significantly different in the control group than in the patient groups, as expected (p < 0.05) (). There were no differences between the CAPD and MHD group in gender, age, BMI, systolic blood pressure, TG, FBG, CRP, Scr, BUN, calcium, phosphorus, i-PTH, hemoglobin, and dialysis duration (p > 0.05). Diastolic blood pressure (DBP), mean arterial pressure (MAP), and TC levels were higher in the CAPD group than in the MHD group (p < 0.05). Plasma albumin levels were lower in the CAPD group than in the MHD group (p < 0.05). The Kt/V values of the patients were 2.08 ± 0.48 for CAPD patients and 1.58 ± 0.42 for MHD patients ().
Table 1. Comparison of the baseline characteristics among CAPD, MHD, and control groups.
The t-IMT was 1.72 ± 0.34, 1.68 ± 0.53, and 1.19 ± 0.36 mm; the a-IMT was 0.87 ± 0.22, 0.85 ± 0.32, and 0.59 ± 0.18 mm; and the total plaque detection rate was 47.22%, 41.30%, and 16.00% in the CAPD, MHD, and control groups, respectively. The t-IMT, a-IMT, and total plaque detection rate in the CAPD and MHD groups were considerably higher than in the healthy control group at the same age (p < 0.01). No significant difference was found between the CAPD and MHD groups in the t-IMT (p = 0.545), a-IMT (p = 0.540), and total plaque detection rate (p = 0.480) ().
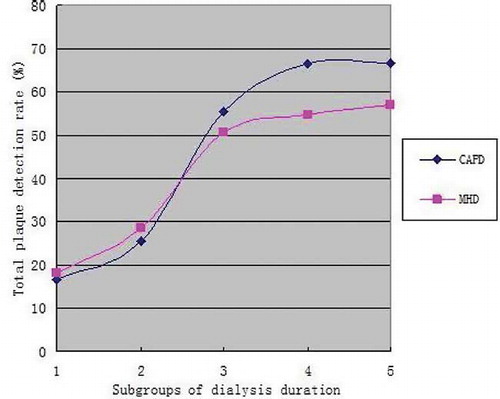
According to the comparison between the subgroups of CAPD patients, the t-IMT and a-IMT were obviously higher in the 60–119 and 120–179 months groups than in the 3–6 months group (p < 0.05). The total plaque detection rates of CAPD patients in the 13–59, 60–119, and 120–179 months groups were higher than in the 3–6 months group (p < 0.05) (). Between the subgroups of MHD patients, the t-IMT in the 60–119 months group was obviously higher than in the 3–6 months group (p < 0.05). The total plaque detection rates in the 13–59, 60–119, and 120–179 months groups were higher than in the 3–6 months group (p < 0.05) ().
Table 2. Comparison of carotid IMT and total plaque detection rate in CAPD and MHD subgroups of different dialysis duration.
After stratification by dialysis duration, the t-IMT, a-IMT, and total plaque detection rate were similar between the CAPD and MHD subgroups in 3–6, 7–12, and 13–59 months (p > 0.05). In the dialysis duration of 60–119 and 120–179 months, the t-IMT in the CAPD subgroup was significantly higher than in the MHD subgroup (p < 0.05). The a-IMT was significantly different in the CAPD subgroup than in the MHD subgroup in 120–179 months (p < 0.05), but it was insignificant in 60–119 months (p > 0.05). The total plaque detection rate was higher in the CAPD subgroup than in the MHD subgroup in 60–119 and 120–179 months, but the differences were insignificant (p > 0.05) (, ).
Figure 1. Comparison of total carotid IMT between CAPD and MHD subgroups.
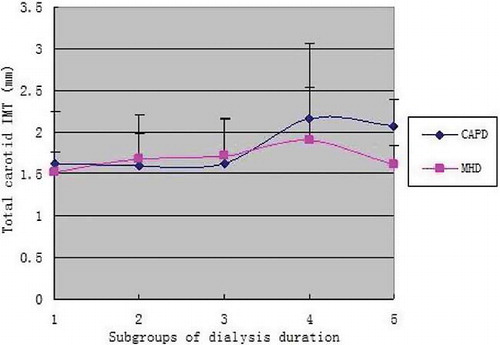
Figure 2. Comparison of average carotid IMT between CAPD and MHD subgroups.
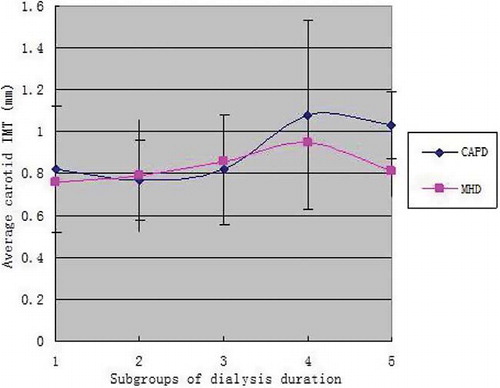
Figure 3. Comparison of total plaque detection rate between CAPD and MHD subgroups.
Note: Subgroups of dialysis duration. 1: 3–6 months, 2: 7–12 months, 3: 13–59 months, 4: 60–119 months, 5: 120–179 months.
DISCUSSION
Atherosclerosis is the most common cause of cardiovascular morbidity in ESRD patients. In the process of atherosclerosis occurrence and development, the intima–media is the earliest affected site, and plaque formation is the most obvious characteristic of atherosclerosis.Citation19 Considering the fact that both carotid and coronary vessels have equivalent risks for developing atherosclerosis,Citation20 increased carotid IMT of uremic patients is a harbinger of coronary atherosclerosis and a prognostic factor for cardiovascular and cerebrovascular accidents.
In our study, carotid IMT is increased and carotid plaque is more frequent in patients undergoing dialysis when compared with controls, indicating that uremic dialysis patients had significant atherosclerotic lesions in the early stage. In addition, no significant difference is found in carotid IMT and plaque detection rate between the CAPD group and MHD group, which is consistent with the findings of Yilmaz et al.Citation21 When dialysis duration is increased, the t-IMT, a-IMT, and total plaque detection rate of CAPD and MHD patients obviously increased, especially after 60 months. These results indicate that the risk of atherosclerosis development is high after 5 years of dialysis, in both CAPD patients and MHD patients.
Our study found no statistically significant difference in carotid IMT and total plaque detection rate between CAPD and MHD patients during the first 59 months of dialysis treatment. After the dialysis duration of 60 months, although there was no difference in total plaque detection rate, there was a trend for a higher carotid IMT associated with CAPD when compared with MHD, especially for t-IMT. The reason might be that because of long-term use of glucose PD solution in PD patients, residual renal function decreases with increasing PD duration, and peritoneal ultrafiltration function declines because of the increase of peritoneal angiogenesis and permeability, which results in higher blood pressure, heart enlargement, heart failure, and other complications accelerating atherosclerosis in CAPD patients.
Our results are different from a recent study reported by Mutluay et al.Citation15 who described that HD has a worse influence on the progression of atherosclerosis than CAPD because the foreign membrane reaction in HD patients may lead to higher carotid IMT and more frequent carotid plaque. Differences in the race, sample size, selection criteria, and research strategy for the studies may partially account for these discrepancies.
It might be argued that our results could be attributed to a statistical error caused by the relatively small sample size, but it does not seem to be the case since a prospective study has observed that HD has a late survival advantage over PD [mortality was greater among PD patients with an adjusted PD/HD hazard ratio of 1.57 (95% confidence interval, 0.97–2.53) after 2 years].Citation9 Moreover, our study shows that the DBP and MAP of the CAPD group were obviously higher than those of the MHD group. The main factors affecting blood pressure were cardiac output and peripheral resistance. Peripheral resistance continued to increase only if atherosclerosis occurred in the small artery. The increased peripheral resistance could lead to increased DBP, and high DBP might reflect small artery sclerosis. The results of blood pressure in this study also showed that the degree of small artery sclerosis was obviously higher in CAPD patients than in MHD patients.
In conclusion, our study showed that both CAPD and MHD affect carotid IMT in Chinese ESRD patients, and the degree of atherosclerosis in CAPD patients might be higher than in MHD patients after 5 years of dialysis. This study is limited by the small sample size and the cross-sectional nature, thus a large-scale, multicenter, and prospective randomized study is required to confirm our results.
ACKNOWLEDGMENTS
This study was supported financially by the Zhejiang Province Science Project (2009B154).
Declaration of interest: The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
REFERENCES
- Coresh J, Astor B, Sarnak MJ. Evidence for increased cardiovascular disease risk in patients with chronic kidney disease. Curr Opin Nephrol Hypertens. 2004;13(1):73–81.
- Perazella MA, Khan S. Increased mortality in chronic kidney disease: A call to action. Am J Med Sci. 2006;331(3):150–153.
- Sarnak MJ, Levey AS, Schoolwerth AC, . Kidney disease as a risk factor for development of cardiovascular disease: A statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Circulation. 2003;108(17):2154–2169.
- Ronco C, Chionh CY, Haapio M, Anavekar NS, House A, Bellomo R. The cardiorenal syndrome. Blood Purif. 2009; 27(1):114–126.
- Moe SM, Chen NX. Pathophysiology of vascular calcification in chronic kidney disease. Circ Res. 2004;95(6):560–567.
- Bots ML, Baldassarre D, Simon A, . Carotid intima-media thickness and coronary atherosclerosis: Weak or strong relations? Eur Heart J. 2007;28(4):398–406.
- Lorenz MW, Markus HS, Bots ML, Rosvall M, Sitzer M. Prediction of clinical cardiovascular events with carotid intima-media thickness: A systematic review and meta-analysis. Circulation. 2007;115(4):459–467.
- Fenton SS, Schaubel DE, Desmeules M, . Hemodialysis versus peritoneal dialysis: A comparison of adjusted mortality rates. Am J Kidney Dis. 1997;30(3):334–342.
- Foley RN, Parfrey PS, Harnett JD, . Mode of dialysis therapy and mortality in end-stage renal disease. J Am Soc Nephrol. 1998;9(2):267–276.
- Stack AG, Molony DA, Rahman NS, Dosekun A, Murthy B. Impact of dialysis modality on survival of new ESRD patients with congestive heart failure in the United States. Kidney Int. 2003;64(3):1071–1079.
- Bloembergen WE, Port FK, Mauger EA, Wolfe RA. A comparison of mortality between patients treated with hemodialysis and peritoneal dialysis. J Am Soc Nephrol. 1995;6(2):177–183.
- Ganesh SK, Hulbert-Shearon T, Port FK, Eagle K, Stack AG. Mortality differences by dialysis modality among incident ESRD patients with and without coronary artery disease. J Am Soc Nephrol. 2003;14(2):415–424.
- Sanabria M, Munoz J, Trillos C, . Dialysis outcomes in Colombia (DOC) study: A comparison of patient survival on peritoneal dialysis vs hemodialysis in Colombia. Kidney Int Suppl. 2008;108:S165–S172.
- Locatelli F, Marcelli D, Conte F, . Survival and development of cardiovascular disease by modality of treatment in patients with end-stage renal disease. J Am Soc Nephrol. 2001;12(11):2411–2417.
- Mutluay R, Degertekin CK, Poyraz F, . Dialysis type may predict carotid intima media thickness and plaque presence in end-stage renal disease patients. Adv Ther. 2012;29(4): 370–382.
- National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: Evaluation, classification, and stratification. Am J Kidney Dis. 2002;39(2 Suppl. 1):S1–S266.
- Lemne C, Jogestrand T, de Faire U. Carotid intima-media thickness and plaque in borderline hypertension. Stroke. 1995;26(1):34–39.
- Daugirdas JT. Second generation logarithmic estimates of single-pool variable volume Kt/V: An analysis of error. J Am Soc Nephrol. 1993;4(5):1205–1213.
- Pasierski T, Sosnowski C, Szulczyk A, Leszczynski L, Rewicki M. [The role of ultrasonography of the peripheral arteries in diagnosing coronary artery disease]. Pol Arch Med Wewn. 2004;111(1):21–25.
- Jadhav UM, Kadam NN. Carotid intima-media thickness as an independent predictor of coronary artery disease. Indian Heart J. 2001;53(4):458–462.
- Yilmaz FM, Akay H, Duranay M, . Carotid atherosclerosis and cardiovascular risk factors in hemodialysis and peritoneal dialysis patients. Clin Biochem. 2007;40(18): 1361–1366.