Abstract
A 49-year-old man with a medical history of polycystic kidney disease was presented to the emergency department with fever and left flank pain. Abdominal examination revealed an enlarged and painful left kidney. The C-reactive protein level was significantly high and the magnetic resonance imaging revealed areas of abnormal intensity and fluid–fluid levels in renal cysts. Brucella abortus was yielded from both blood and cyst fluid culture. Standard therapy (rifampicin plus doxycycline) of brucellosis was started, but the clinical and laboratory signs subsided after the addition of ciprofloxacin. There was no need for aspiration of infected cyst fluid. Hereby, according to the medical database search, we report that the first renal cyst infection caused by B. abortus was successfully treated with triple antibiotic therapy.
INTRODUCTION
Polycystic kidney disease (PKD) is one of the most common inherited renal disorders.Citation1 The most remarkable characteristic of PKD is the occurrence of numerous renal cysts, resulting in enlargement of the kidneys. It affects one in 500–1000 individuals and accounts for 4–10% of end-stage renal disease.Citation2 Patients with PKD sometimes develop complications (such as infection and bleeding). Among these complications, cyst infections are relatively infrequent but are associated with serious outcomes.Citation3 Fever and abdominal pain are the main symptoms of cyst infection, but radiological and laboratory assessment is also required for the definite diagnosis. Pathogens are typically bowel flora such as Escherichia coli and retrograde infection of renal cysts via the ureter from the bladder is the main route of infection.Citation2 However, unusual pathogens reported as the etiological agent in cyst infection suggest alternate route in infection.Citation3,4 Debate is also present for the treatment of cyst infection. Antibiotics with well penetrating capability have brought new treatment modality into such infections. Here we describe a case of renal cyst infection caused by Brucella abortus, which was successfully treated with antibiotics.
CASE REPORT
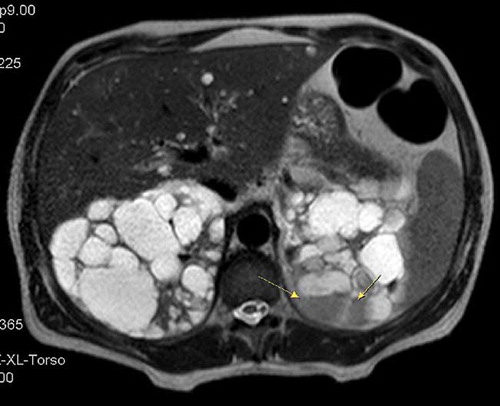
A 49-year-old man with a medical history of PKD was presented to the emergency department with 10 days of fever and left flank pain. Except for a family history of PKD, there was no other remarkable information in his medical history. On admission, his vital signs were as follows: temperature 39°C, blood pressure 140/80 mm Hg, and pulse rate 75 beats/min. Abdominal examination revealed hepatomegaly and enlarged kidneys. The flank pain was exacerbated by the palpation of left kidney. The results of the remainder of the physical examination were unremarkable. Laboratory studies showed hemoglobin 12.8 g/dL, white blood cells (WBC) 6270/μL, platelet count 254,000/μL, blood urea nitrogen 52 mg/dL, creatinine 1.27 mg/dL, aspartate aminotransferase (AST) 23 IU/L, alanine aminotransferase (ALT) 29 IU/L, alkaline phosphatase (ALP) 46 IU/L, gamma-glutamyl transferase (GGT) 48 IU/L, lactate dehydrogenase (LDH) 219 IU/L, total protein 6.3 mg/dL, albumin 3.1 mg/dL, C-reactive protein (CRP) 208 mg/L, and erythrocyte sedimentation rate (ESR) 68 mm/h. The urine sediment was normal. According to medical history, clinical presentation, and laboratory results cyst infection was the initial diagnosis. High-CRP value was in favor of cyst infection. Abdominal magnetic resonance imaging (MRI) was also ordered to differentiate the diagnosis. MRI showed thick-walled, heterogeneous cysts slightly hyperintense on T1-weighted MR images and with peripheral enhancement after gadolinium injection (). A cyst in the left kidney with a fluid–fluid level was also suggestive of infected cyst on T2-weighted image (). On the diagnosis of cyst infection, empirical antibiotic with intravenous (IV) ceftriaxone (2 g/24 h) was prescribed after obtaining urine and blood cultures. The urine culture showed no bacterial growth and the patient remained febrile with the antibiotic treatment. On the sixth day of the treatment, blood culture yielded B. abortus. Wright agglutination test was also detected positive for 1/320 titers. Requestioning the patient history revealed the consumption of unpasteurized milk and cheese. The treatment regimen was changed to doxycycline (100 mg/12 h) plus rifampicin (900 mg/day). Patient’s symptoms were continued and the CRP values did not decline despite the 10 days of treatment with modified antibiotic regimen. An ultrasound-guided needle aspiration fluid was obtained for etiological diagnosis of cyst infection, and B. abortus was also isolated from the specimen. Upon this IV, ciprofloxacin (400 mg/12 h) was added to the treatment regimen. After a couple of days with this triple antibiotic therapy, the symptoms subsided and the CRP levels started to decrease. At the end of the second week of efficient therapy, clinical and laboratory response was completely achieved. At this point, the patient was discharged from the hospital and the treatment was continued with oral antibiotics until the end of the sixth week of the therapy.
Figure 1. Postgadolinium T1-weighted image shows slightly hyperintense cyst (arrow) with peripheral contrast enhancement.
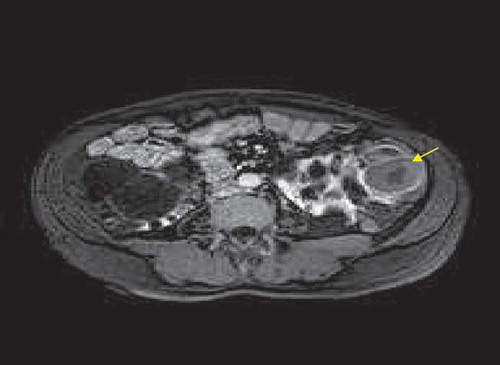
Figure 2. T2-weighted image shows fluid–fluid level (arrow) in the cyst that is located in the upper pole of the left kidney.
DISCUSSION
Cyst infection is a well-recognized complication of PKD and has been reported to be the second most common cause of death in this group of patients.Citation5 Many microorganisms have been reported as the etiological agent but digestive tract microorganisms especially E. coli accounts for the majority.Citation6 In this case, the cause of cyst infection was B. abortus. Brucella spp. is an intracellular Gram-negative bacterium and is the causative agent of brucellosis. Brucellosis is a zoonotic infection transmitted to humans by contact with fluids from infected animals (sheep, cattle, goats, or other animals) or derived food products such as unpasteurized milk and cheese. It has high morbidity for humans and is an important cause of public health problems in many developing countries. Almost every organ system involvement has been reported with Brucella spp., but the renal cyst infection was somewhat novel. The available databases were searched for the association of Brucella spp. and renal cyst infection. “Brucella” and “PKD” were the search terms. There was no search result and it seems that renal cyst infection due to Brucella spp. would be the first report. Accordingly, this case reveals that infecting agents other than bowel flora may be the causative agent of renal cyst infection. The involvement of renal cyst may be a part of the systemic illness caused by such microorganisms, but the marked symptoms will possibly focus the physician to cyst infection with a resulting inappropriate antibiotic prescription. This points that, microorganisms such as Brucella spp. should be held in differential diagnosis of cyst infection in patient living in endemic areas. Ascending route through urinary tract is the most accepted concept for the development of cyst infection. Consequently, microorganism isolated from the urinary tract is commonly recognized as the responsible agent. But, the present and some reported cases show that infection paths other than urinary tract are present.Citation4 After ingestion or inoculation, Brucella spp. invade the mucosa, where polymorphonuclear leukocytes and activated macrophages mediate immune responses to eradicate the bacteria. However, Brucella can multiply and survive intracellularly.Citation7 They are then transported intracellularly via the lymphatics to organs rich in reticuloendothelial cells, and from there travel to other organs and tissues, where they can cause infection. Accordingly, although the precise infectious route was unidentified, hematogenous seeding of the cyst was the most probable way of infection. Hence, cyst fluid aspiration should be preferred for culture in patients without obvious urinary infection findings (such as dysuria, pollakiuria, and pyuria) and for those nonresponding to antibiotic therapy. The treatment of renal cyst infection is often difficult and there is a high treatment failure rates despite prolonged appropriate antibiotic therapy. Percutaneous or surgical drainage of the infected cyst is often an applied procedure in such cases to avoid a fatal outcome.Citation8 But some antibiotics with their high penetrating capability to renal cysts have raised a noninvasive treatment option in such infections. Intracystic antibiotic diffusion and accumulation vary widely and probably depend on passive diffusion as well as active transepithelial transport. Among the antibiotics, quinolones are usually favored because of their lipophilic properties that lead to an increased diffusion in infected cysts and their bactericidal activity.Citation9,10 But the problem with quinolones is the growing resistance to these antibiotics. The frequent and inappropriate prescription of quinolones to community-based patients has raised the problem to current situation.Citation11 In areas faced with this fact, the empirical antibiotic preference for urinary tract infection has changed from quinolones to β-lactams (such as broad-spectrum cephalosporins). This was the reason for initial ceftriaxone therapy in our case. Nevertheless, according to the available data, quinolones seem to be the best option for cyst infection and precedence should be given to these drugs after establishing the antibiotic susceptibility. This approach may also be feasible for the treatment of cyst infections caused by nonEnterobacteriaceae microorganisms like Brucella spp. The recommended first-line therapy for brucellosis includes streptomycin or doxycycline in combination with rifampicin.Citation12 Although there are some cases seriesly reporting successful outcomes with quinolone including regimen, it is not supported by randomized clinical studies.Citation13,14 Even so, the long duration of unresponsiveness to doxycycline plus rifampicin pushed us also to add ciprofloxacin to the treatment according to the available antibiotic properties and reported case series. However, the success achieved with the applied therapy should be supported by randomized studies to recommend quinolones in the first-line therapy for cyst infections.
Declaration of interest: The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the article.
REFERENCES
- Sklar AH, Caruana RJ, Lammers JE, Strauser GD. Renal infections in autosomal dominant polycystic kidney disease. Am J Kidney Dis. 1987;10:81–88.
- Sallee M, Rafat C, Zahar JR, . Cyst infections in patients with autosomal dominant polycystic kidney disease. Clin J Am Soc Nephrol. 2009;4:1183–1189.
- Tsuchiya Y, Ubara Y, Suwabe T, . The renal cyst infection caused by Salmonella enteritidis in a patient with autosomal dominant polycystic kidney disease: how did this pathogen come into the renal cysts? Clin Exp Nephrol. 2011;15:151–153.
- Yang CC, Chuang FR, Chen JB, Lee CT, Wu CH. A potential salvage therapy for refractory renal cyst infection in patients with autosomal dominant polycystic kidney disease. Clin Exp Nephrol. 2012;16:183–184.
- Fick GM, Johnson AM, Hammond WS, Gabow PA. Causes of death in autosomal dominant polycystic kidney disease. J Am Soc Nephrol. 1995;5:2048–2056.
- Migali G, Annet L, Lonneux M, Devuyst O. Renal cyst infection in autosomal dominant polycystic kidney disease. Nephrol Dial Transplant. 2008;23:404–405.
- Fugier E, Pappas G, Gorvel JP. Virulence factors in brucellosis: implications for aetiopathogenesis and treatment. Expert Rev Mol Med. 2007;9:1–10.
- Torres VE, Harris PC. Autosomal dominant polycystic kidney disease: the last 3 years. Kidney Int. 2009;76:149–168.
- Elzinga LW, Golper TA, Rashad AL, Carr ME, Bennett WM. Ciprofloxacin activity in cyst fluid from polycystic kidneys. Antimicrob Agents Chemother. 1988;32:844–847.
- Hiyama L, Tang A, Miller LG. Levofloxacin penetration into a renal cyst in a patient with autosomal dominant polycystic kidney disease. Am J Kidney Dis.2006;47:e9–e13.
- Kurtaran B, Candevir A, Tasova Y, . Antibiotic resistance in community-acquired urinary tract infections: prevalence and risk factors. Med Sci Monit. 2010;16:CR246–CR251.
- Bossi P, Tegnell A, Baka A, Bichat guidelines for the clinical management of brucellosis and bioterrorism-related brucellosis. Euro Surveill. 2004;9:E15–E16.
- Falagas ME, Bliziotis IA. Quinolones for treatment of human brucellosis: critical review of the evidence from microbiological and clinical studies. Antimicrob Agents Chemother. 2006;50:22–33.
- Solis Garcia del Pozo J, Solera J. Systematic review and meta-analysis of randomized clinical trials in the treatment of human brucellosis. PLoS One. 2012;7:e32090.