Dear Editor
Septic arthritis of sternoclavicular joint comprises approximately <1% of all joint infections.Citation1,2 Common in elderly, but in intravenous drug abusers, it often occurs in the young.Citation1–3 The development of acute kidney injury (AKI) in association with this entity is very rare. We present herein the management of one such patient. A 51 year-old male presented to the emergency department with high-grade fever and progressive tender swelling at the base of the neck extending to the right of the chest wall. He was toxic, hypotensive, oliguric, and dyspneic at the time of presentation. Laboratory evaluation revealed anemia [hemoglobin (Hb)—8.6 g%], polymorphonuclear leukocytosis [total counts (TC)—17,800/mm3], thrombocytopenia (5700/mm3), and severe renal failure [blood urea (B.urea)—215 mg%, serum creatinine (s.cr)—6.4 mg%] with bland urinary sediment. Ultrasound of the abdomen revealed normal-sized kidneys with no obstruction. In view of sudden onset renal failure with rapid progression to severity [risk injury failure loss end-stage (RIFLE)3/acute kidney injury network (AKIN)-3] despite fluid resuscitation, bland urinary sediment, and normal-to-enlarged echogenic kidneys with no obstruction on ultrasound, the possibility of intrinsic renal failure secondary to acute tubular necrosis was considered. Plain chest X-ray showed chest wall abscess with air pockets. Plain computed tomography of the chest was suggestive of chest wall abscess extending to mediastinum with air pockets. Incision and drainage of pus was performed. Pus and blood cultures grew Escherichia coli and were treated with piperacillin/tazobactam as per the sensitivity. Follow-up contrast computed tomography done 2 weeks later revealed bony destruction of clavicle and sternoclavicular joint involvement (). The patient was supported by hemodialysis (HD) for AKI. After seven sessions of HD, he improved from AKI (s.cr—1.9 mg%). In view of sternoclavicular joint and medial end of clavicular bone destruction, bone resection surgery was suggested; however, he got discharged on request and was lost to follow-up subsequently.
Figure 1. Computed tomography (plain) showing abscess in the chest wall extending to mediastinum with multiple air pockets.
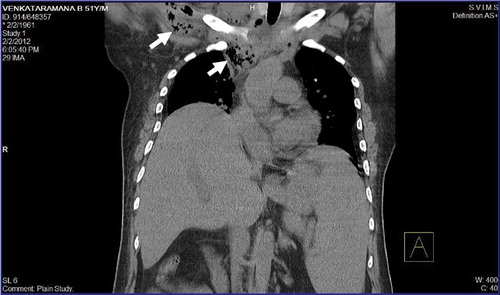
Figure 2. Follow-up computed tomogram showing right sternoclavicular joint arthritis with bony destruction of manubrium and destruction following drainage of pus.

The sternoclavicular joint is a synovium-lined joint composed of inferior medial clavicular head, superiorly lateral notch of the manubrium, and the cartilage of first rib. The joint capsule is reinforced by the strong anterior and posterior sternoclavicular ligaments. As a result, the joint space is minimal and is not freely distensible.Citation1,3 In such a situation when infection occurs, it results in local destruction very quickly and because of the mounting pressure in the joint space hematogenous and lymphatic spread is rapid and potentially life threatening. The often reported complications are chest wall abscess (25%), mediastinitis (13%), empyema, septicemia (62%), and shock.Citation1,3 Immunocompromised states such as chronic renal failure, diabetes, long-term steroid use, malnutrition, and intravenous drug abuse are the predisposing factors.Citation1–4 In addition to the broad-spectrum antibiotic coverage and drainage of the pus, the presence of bony destruction is an indication of resection surgery ().Citation3,5 Advanced imaging modalities such as computed tomography/magnetic resonance imaging are invaluable in the diagnosis and follow-up. Often this entity needs prolonged antibiotic coverage for 4–6 weeks.Citation3
In conclusion, this presentation represents a serious form of right sternoclavicular joint infection with local complications such as chest wall abscess, mediastinitis, and systemic complications such as hypotension and severe AKI. Infection responded to prolonged usage of higher generation antibiotics following the drainage of pus. Bony resection could not be done as the patient did not consent. He recovered from AKI (RIFLE 3/AKIN-3) following seven sessions of HD. Our literature review did not show an association of septic arthritis of sternoclavicular joint with severe renal failure needing dialysis supports and hence our interest in reporting this entity.
Chennu Krishna Kishore
Department of Nephrology, SrivenkateswaraInstitute of Medical Sciences (SVIMS), Tirupati, India
Email: [email protected]
Sriramnaveen Parvathina
Department of Nephrology, SrivenkateswaraInstitute of Medical Sciences (SVIMS), Tirupati, India
Email: [email protected]
Boreddy Varalakshmi
Department of Nephrology, SrivenkateswaraInstitute of Medical Sciences (SVIMS), Tirupati, India
Email: [email protected]
Bodagala Vijayalakshmi
Department of Radiodiagnosis, SrivenkateswaraInstitute of Medical Sciences (SVIMS), Tirupati, India
Email: [email protected]
Amancharla Yadagiri Lakshmi
Department of Radiodiagnosis, SrivenkateswaraInstitute of Medical Sciences (SVIMS), Tirupati, India
Email: [email protected]
Vishnubotla Sivakumar
Department of Nephrology, Srivenkateswara Institute of Medical Sciences (SVIMS), Tirupati, India
Email: [email protected]
References
- Pradhan C, Watson NFS, Jagasia N, Chari R, Patterson JE. Bilateral sternoclavicular joint septic arthritis secondary to indwelling central venous catheter: a case report. J Med Case Rep. 2008;2:131.
- Mikroulis DA, Verettas DA, Xarchas KC, Lawal LA, Kazakos KJ, Bougioukas GJ. Sternoclavicular joint septic arthritis and mediastinitis: a case report and review of literature. Arch Orthop Trauma Surg. 2008;128:185–187.
- Ross JJ, Shamsuddin H. Sternoclavicular septic arthritis: review of 180 cases Medicine. 2004;83(3):139–148.
- Ryan S, O’ Donoghue G, Stokes M. A case of anterior chest wall pain in an intravenous drug user. Infect Dis Clin Pract. 2008;16:307–308.
- Song HK, Sloane Guy T, Kaiser LR, Shrager JB. Current presentation and optimal management of sternoclavicular joint infections. Ann Thorac Surg. 2002;73:427–431.