
Abstract
Objective: Tubulointerstitial fibrosis is one of the strongest independent predictive factors in determining the prognosis in IgA nephritis. Recently, software-based quantitative measurement of interstitial fibrosis with Sirius Red staining has entered the practice. The objective of this study was to investigate the prognostic value of measurement of interstitial nephritis with this method in IgA nephritis. Method: Forty-three patients diagnosed with IgA nephritis with renal biopsy between the years 2005 and 2009 were included in this retrospective observational study. The diagnostic biopsies of 37 patients were examined. Basal data included age, gender, creatinine level, glomerular filtration rate (GFR), presence of proteinuria, hypertension, glomerulosclerosis, mesangial proliferation, and interstitial fibrosis and fibrosis index calculated by the measurement of computed images of Sirius Red positive areas. Final visit included evaluation of development of end-stage renal disease (ESRD), and GFR (whether = 60 mL/min or <60 mL/min). Results: Numbers of patients with hypertension (75% vs. 34.5%; p = 0.050), ESRD development (62.5% vs. 20.7%, p = 0.035), GFR <60 mL/min (87.5% vs. 31%; p = 0.007) were greater; and basal GFR (34.25 ± 25.29 vs. 64.14 ± 35.34; p = 0.048) was lower in high-intensity interstitial fibrosis group (>1000 μm2) compared to low-intensity interstitial fibrosis group (≤1000 μm2). Conclusion: Quantitative analysis of computed imaging of areas of Sirius Red positive tubulointerstitial fibrosis might serve as an effective novel method to determine the prognosis in IgA nephritis.
Introduction
IgA nephritis is one of the most common primary glomerulonephritis worldwide.Citation1 Although known as a benign condition, end-stage renal disease (ESRD) requiring renal replacement therapy develops in about 10–20 years in about 15–25% of patients.Citation2 Therefore, various histological and clinical parameters have been defined to determine patients at high risk of progressive disease. Factors of poor prognosis include presence of renal dysfunction at the time of diagnosis, prolonged severe proteinuria, lack of macroscopic hematuria episodes, hypertension and familial disease, and age.Citation3,Citation4 Histopathologically, glomerulosclerosis (global/segmental or both) and tubulointerstitial fibrosis constitute the strongest independent predictive factors of progressive disease.Citation5–8
Sirius Red staining has recently entered the nephrology practice, particularly in evaluating interstitial fibrosis of chronic allograft nephropathy following transplantation. It is chosen especially for its selectivity to collagen type 1 and 3. Areas with Sirius Red staining indicative of interstitial fibrosis have been calculated quantitatively with computer software in chronic allograft nephropathy; and it has been demonstrated that high intensity interstitial fibrosis correlated with glomerular filtration rate (GFR).Citation9,Citation10 Inter-observer variability of pathologists encountered in semi-quantitative analyses, such as Banff, might be prevented with this quantitative measurement.Citation10 There are two studies in literature evaluating interstitial fibrosis with Sirius Red staining.Citation11,Citation12 One of these studies is the quantitative morphometric measurement of Lupus nephritis with pico Sirius Red staining. Nuclear, collagenous matrix, and fibrillary area indexes have been measured in this study; and it has been demonstrated that greater nuclear index correlated with clinical parameters of disease activation, greater collagenous matrix index indicated relapse and progression to ESRD, and fibrillary index was associated with doubling of serum creatinine and relapse.Citation12 However, according to our research there are no studies in the literature on the use of Sirius Red staining to evaluate interstitial fibrosis in IgA nephritis. Our objective was to determine the efficacy of this quantitative histopathological method in establishing the prognosis of IgA nephritis.
Materials and methods
This was a retrospective observational study examining patients with IgA nephritis diagnosed with renal biopsy at the Department of Nephrology, Izmir Ataturk Training and Research Hospital between the years 2005 and 2009. Forty-three patients with at least one year of follow-up and no history of renal replacement therapy at the time of diagnosis were included. One patient was excluded for a follow-up time shorter than one year, and two patients were excluded because of a diagnosis of systemic lupus erythematous (SLE), according to biopsy results and serological marker positivity (ANA, anti-ds DNA). The biopsy preparations were lost in three patients. Evaluation of the clinical parameters was performed in 40 patients, and histopathological evaluation was performed in 37 patients.
Demographic and basal laboratory data were determined as sex, age at diagnosis, serum creatinine, GFR, proteinuria, and arterial hypertension (>140/90 mmHg). Proteinuria was calculated as the protein/creatinine ratio in spot urine specimen. GFR was calculated by the Modification of Diet in Renal Disease (MDRD) equation.Citation13
Examination of the computer-based medical records demonstrated that patients with <1 g/day proteinuria and normal renal function tests were followed without any treatment, patients with ≥1 g/day proteinuria and hypertension were treated with ACE inhibitor and/or angiotensin II receptor blocker, and patients with crescentic glomerulonephritis or nephrotic syndrome were treated with steroids and immunosuppressive agents.
Results of biopsy examinations performed at the time of diagnosis were obtained from the archives of pathology laboratory. These cross sections had been stained with hematoxylin eosin in addition to mason trichrome, periodic acid-Schiff, and methenamine silver. Immuno fluorescein microscopic examination included administration of fibrinogen, IgG, IgA, IgM, C3, C1q, Kappa and Lambda, and diagnosis was established by evaluating glomerular deposition. Biopsy samples were re-evaluated by the basal IgA Oxford classification.Citation14 Evaluation by the Oxford criteria could be performed in 33 out of 37 study patients due to the presence of two or less glomeruli in cross sections.
Single cross sections obtained from paraffin blocks were stained with the Sirius Red stain using the Putchler’s picro Sirius Red method.Citation15 Two solutions were prepared in this staining process. First, 0.5 g Sirius Red F3B (Aldrich Chemicals) was saturated with 500 mL of picric acid solution. Additionally, 1 liter of distillated water was turned acidic with 5 mL of acetic acid. All preparations were bathed in the first solution prepared with Sirius Red for 14 hours, and then washed twice with the acidified water. The solution left on the preparation was cleared with drying paper and preparation was dehydrated with 100% ethanol for three times. The preparation was cleaned with xylene and mountain resin.
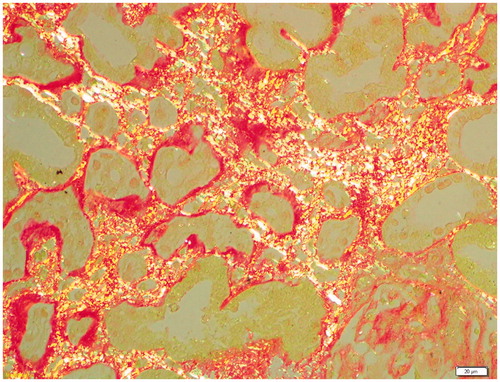
Stained preparations were evaluated under light microscopy (Olympus BX51). Under the light microscopy, collagen was observed as red, cytoplasm as yellow, and nucleus as black. Later, figures of Sirius Red stained preparations were obtained with polarized attachment of light microscopy ( and ). Areas with Sirius Red positive staining were stored at computer media with the Olympus DP72 Capture Interface software. Under the polarized attachment, thin fibrils (Type 1 and 3 collagen fibrils) of Sirius Red stained areas appeared green, whereas thick fibrils had yellow or orange double fringe appearance. Areas with the most intense Sirius Red staining in tubulointerstitial space in cortical and/or corticomedullary renal biopsy specimens were determined under 40× magnification of light microscopy in each case. All images were transferred to an associated computer containing the Olympus DP72 Capture Interface software. Unit space of the visualized area was determined in the computer screen. An area of 90,855 µm2 was determined for each preparation. A quantitative value for interstitial fibrosis was obtained by measuring the areas with Sirius Red staining and yellow-green double fringe within the unit space. Ratio of these Sirius Red positive areas and cortical unit spaces was calculated in percentages and termed as the fibrosis index.Citation12
Figure 1. Sirius Red stained interstitial space, normal light microscopy appearance.
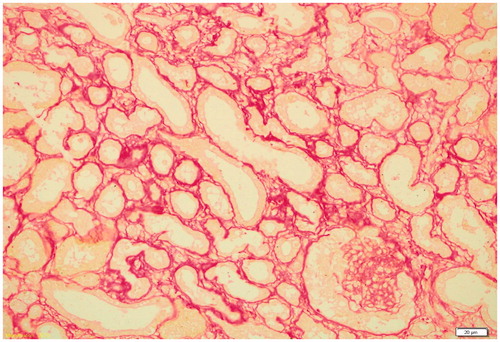
Figure 2. Yellow-green reflecting appearance of the same preparation under the polarized attachment.
Patients were classified according to development of ESRD, which was defined as chronic repetitive dialysis. Patients were also grouped as low- and high-intensity interstitial fibrosis according to the quantitative measurement with Sirius Red staining. Basal clinical and histopathological data were compared between these groups.
All statistical analyses were performed with the Statistical Package for Social Sciences (SPSS) Graduate Pack 14.0 (SPSS Inc., Chicago, IL). Continuous variables were evaluated with the Mann–Whitney U test, and categorical variables were evaluated with the Chi square test. Analyses with single and multiple variables were compared with logistic regression analyses and a p value of <0.05 was considered statistically significant.
Results
The study population consisted of 40 patients including 19 females and 21 males. The majority of patients (75%) were younger than 40 years old. Mean duration of follow-up was 32.8 (12–144) months. Mean GFR at the time of diagnosis was 55.75 ± 35.02 mL/min. Seventy percent of the patients had >1 g/day proteinuria. Clinical and pathological data of the patients at the time of renal biopsy are presented in .
Table 1. Clinical and pathological data of the patients at the time of renal biopsy.
Evaluation of renal prognosis by the basal clinical and laboratory features revealed that the rate of development of ESRD was greater in patients with lower GFR, higher creatinine, and proteinuria at the time of diagnosis (). Age and sex, on the other hand, had no influence on renal prognosis.
Quantitative evaluation with Sirius Red was performed on the biopsy specimens of 37 patients. The preparations of four patients which were excluded from the Oxford classification were included in the latter because no glomeruli are needed for the evaluation of interstitial fibrosis. Accordingly, more Sirius Red positive areas were determined in patients who developed ESRD compared to those without ESRD in the final follow-up (1232.75 vs. 723.24; p = 0.344). Fibrosis index, calculated by the ratio of Sirius Red positive areas and unit space, was also greater in patients developing ESRD (1.32% vs. 0.73%; p = 0.434). Two groups were formed by calculating the 1000 µm2 threshold value of Sirius Red positive areas in the ROC curve. Groups were defined as high intensity (>1000 µm2) and low intensity (≤1000 µm2). Patients in the greater and low-intensity groups were compared in terms of age, sex, presence of hypertension, basal proteinuria, basal creatinine, basal GFR, histopathological features, renal survival, and number of patients with GFR <60 mL/min ().
Table 2. Clinical and histopathological features of groups with high and low intensity.
Significant difference was determined between patients with high- and low-intensity in terms of the presence of hypertension, basal GFR, renal survival, and number of patients with GFR <60 mL/min. The greater rates of hypertension (75% vs. 34.5%; p = 0.05), ESRD (62.5% vs. 20.7%; p = 0.035), and GFR <60 mL/min (87.5% vs. 31%; p = 0.035) were determined in the group with high intensity. Basal GFR was 34.25 mL/min in the high compared to 64.14 mL/min in the low-intensity groups (p = 0.048).
Discussion
Our study shows that evaluating interstitial fibrosis quantitatively with Sirius red staining in patients with IgA nephropathy may be used in the prognosis of the disease. We found that development of ESRD was higher in the high-intensity interstitial fibrosis group than the low-intensity group.
IgA nephritis, although known as a benign disorder, leads to ESRD in 10–20 years in 15–25% of the patients.Citation2,Citation16 Therefore, determination and early treatment of patients at risk of poor prognosis is important.
Several histological and clinical parameters aimed at determining patients at high risk of progressive disease have been defined. Impaired renal functioning at the time of diagnosis, prolonged, severe proteinuria, lack of episodes of macroscopic hematuria, presence of hypertension, familial disease, and age have been defined as poor prognostic factors. In terms of histological parameters, strongest independent predictive factors of progressive disease are glomerular sclerosis and tubulointerstitial fibrosis.Citation3,Citation4
Similar to all chronic renal diseases, interstitial fibrosis secondary extracellular matrix deposition in the interstitium have been long known to cause renal failure in IgA nephritis. Glomerular sclerosis which is not seen in the renal biopsy specimens at the onset of disease is observed when the GFR decreases and proteinuria increases.Citation17 Studies on patients with renal transplantation have demonstrated that quantitative measurement of interstitial fibrosis is a deterministic marker in the prognosis of transplanted kidney and might replace other markers of interstitial fibrosis.Citation10
Today, Sirius Red method is one of the few morphometric measurements of interstitial fibrosis.Citation10,Citation12 There are few studies evaluating renal prognosis with this method in glomerulonephritis. It has been demonstrated that the quantitative results obtained in Lupus nephritis correlate significantly with disease activation, relapse, progression to terminal renal failure, and doubling of serum creatinine.Citation12
According to our research, this is the first study in literature evaluating interstitial fibrosis in IgA nephritis quantitatively. Another study on glomerular disease is the single-centered cohort study of Hunter et al. on patients with lupus nephritis.Citation12 Novel paraffin cross sections were obtained from the original biopsy specimens of each case and stained with picro Sirius Red. Four indices were defined in the picro Sirius Red stained preparations: tubular index, nuclear index, collagenous matrix index, fibrillary index. Finally, it has been reported that greater nuclear index correlated with clinical parameters (proteinuria, creatinine clearance, serum albumin levels) of disease activation, greater collagen matrix index was a marker of relapse and progression to ESRD, and that fibrillary index was a marker of relapse and progressive disease assessed by serum creatinine doubling rate. Hence, Hunter et al. have suggested that these easily measured quantitative indices might be used to predict the renal prognosis at the onset of disease process.
IgA nephritis and lupus nephritis cannot be compared directly because these two differ significantly in terms of pathogenesis and clinical features. IgA nephritis is a disorder of the alternative complement, particularly the mannose-binding lectin pathway; whereas, lupus nephritis is a disorder of the classical complement pathway. One is a rather slowly progressive disease, whereas the other courses with relapses. However, interstitial fibrosis is the common pathogenetic ending in all glomerulonephritis. Therefore, demonstration of the prognostic role of quantitative evaluation of interstitial nephritis in lupus nephritis with Sirius Red staining has given us a lead in this study.
Evaluation of interstitial fibrosis with the picric Sirius method in IgA nephritis has first been investigated in this study. Due to the distinct disease course of lupus nephritis, Hunter et al. have examined not only the interstitial fibrosis, but also nuclear index, tubular index, and collagen matrix index. The fibrillary index of the latter study and fibrosis index of our study might be comparative. Higher fibrillary index has indicated higher serum doubling rate suggestive of progressive disease. Similarly, higher fibrosis index was determined in groups of patients developing ESRD and with GFR <60 mL/min. However, this result was not statistically significant.
In groups of high and low Sirius Red staining intensity, number of patients with hypertension was significantly higher (75% vs. 34.5%; p = 0.05) and basal GFR value was significantly lower (34.25 vs. 64; p = 0.048) in the group with high intensity. Similarly, number of patients developing ESRD (62.5% vs. 20.7%; p = 0.035) and with GFR <60 mL/min (87.5% vs. 31%; p = 0.007) were significantly higher in the high-intensity group. Accordingly, poorer prognosis should be expected with greater intensity of interstitial fibrosis measured with the Sirius Red method. Basal GFR and presence of hypertension also correlate with Sirius Red intensity.
Briefly, this is the only study of quantitative evaluation of interstitial fibrosis in IgA nephritis. Although it is difficult to make a comparison with previous studies of quantitative evaluation of interstitial fibrosis—mostly chronic allograft nephropathy studies—it does appear to be a significant marker of renal prognosis, when interstitial fibrosis is considered as a common issue of chronic renal diseases. Therefore, further prospective studies with more patients and longer duration of follow-up should be performed following this preliminary study.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
- Levy M, Berger J. Worldwide perspective of IgA nephropathy. Am J Kidney Dis. 1988;12:340–347
- Smith AC, Feehally J. New insights into the pathogenesis of IgA nephropathy. Pathogenesis of IgA nephropathy. Springer Semin Immunopathol. 2003;24(4):477–493
- Reich HN, Troyanov S, Scholey JW, et al. Remission of proteinuria improves prognosis in IgA nephropathy. J Am Soc Nephrol. 2007;18:3177–3183
- Haas M, Rahman MH, Cohn RA, et al. IgA nephropathy in children and adults: comparison of histologic features and clinical outcomes. Nephrol Dial Transplant. 2008;23:2537–2545
- D’ Amico G. Natural history of idiopathic IgA nephropathy: role of clinical and histological prognostic factors. Am J Kidney Dis. 2000;36:227–237
- D’Amico G. Natural history of idiopathic IgA nephropathy and factors predictive of disease outcome. Semin Nephrol. 2004;24:179–196
- Lee SM, Rao VM, Franklin WA, et al. IgA nephropathy: morphologic predictors of progressive renal disease. Hum Pathol. 1982;13:314–322
- Daniel L, Saingra Y, Giorgi R, et al. Tubular lesions determine prognosis of IgA nephropathy. Am J Kidney Dis. 2000;35:13–20
- Diaz Encarnacion MM, Griffin MD, Slezak JM, Bergstralh EJ, Stegall MD. Correlation of quantitative digital image analysis with the glomerular filtration rate in chronic allograft nephropathy. Am J Transplant. 2004;4(2):248–256
- Grimm PC, Nickerson P, Gough J, et al. Computerized image analysis of Sirius Red-stained renal allograft biopsies as a surrogate marker to predict long-term allograft function. J Am Soc Nephrol. 2003;14(6):1662–1668
- Liu J, Liang H, Liu CS. Expression of transforming growth factor-beta1 in renal fibrosis of human mesengial proliferative glomerulonephritis. Zhejiang Da Xue Xue Bao Yi Xue Ban. 2004;33(1):46–50, 54
- Hunter MG, Hurwitz S, Bellamy CO, Duffield JS. Quantitative morphometry of lupus nephritis: the significance of collagen, tubular space, and inflammatory infiltrate. Kidney Int. 2005;67(1):94–102
- Levey AS, Coresh J, Greene T, et al. Using standardized serum creatinine values in the modification of diet in renal disease study equation for estimating glomerular filtration rate. Ann Intern Med. 2006;145(4):247–254
- Cattran DC, Coppo R, Cook HT, et al. The Oxford classification of IgA nephropathy: rationale, clinicopathological correlations, and classification. Kidney Int. 2009;76:534–545
- Sweat F, Putchler H, Rosenthal SI. Sirius red F3BA as stain for connective tissue. Archs Pathol. 1964;78:69–72
- Yang NS, Wu QQ, Du Y, et al. Risk factors affecting the long-term outcome of IgA nephropathy. Zhonghua Nei Ke Za Zhi. 2005;44(8):597–600
- Haas M. Histological subclassification of IgA nephropathy: a clinicopathologic study of 244 cases. Am J Kidney Dis. 1997;29:829–842