
Abstract
Background: The prevalence of HTN varies considerably worldwide. This study was carried out to illustrate the prevalence of hypertension in a group of Iranian population based on the data gathered for Iranian Multi-centric Osteoporosis Studies (IMOS). Methods: This study analyzes the systolic and diastolic blood pressure from the IMOS, a multi-centric cross-sectional study carried out on apparently healthy men and women in urban areas of major Iranian cities to study bone health. Results: Overall, 26.21% of the studied cases were estimated to be hypertensive; the condition was more prevalent among older males. Each year increase in age was associated with 1.070 higher risk of developing hypertension. Conclusion: Hypertension is quite prevalent among Iranian population and the prevalence of the condition is rising in the context of progressive rise in age and BMI.
Introduction
Hypertension (HTN) is the most important cardiovascular risk factor worldwide, contributing to the burden imposed by one-half of patients with coronary heart disease and approximately two-thirds of those suffering from cerebrovascular problems.Citation1–3
The prevalence of HTN varies considerably worldwide, ranging from 11–30% in Latin America, 20–33% in Africa, 18–22% in the United States, 25–30% in Far East Asia, and 44% in some European countries.Citation4–8 The lowest rate is reported in rural areas in India (6.8% in females and 3.4% in males) whereas Poland has the highest mark (72.5% in females and 68.9% in males).Citation9
There is convincing evidence showing a global outbreak of the condition, partially attributable to the epidemic of overweight and obesity during the past two decades.Citation10 While the prevalence of the condition in many developing countries is estimated to be lower than that reported in countries such as the United States, England, and Finland, there is strong evidence indicating a growing outbreak in those countries.Citation4,Citation11,Citation12
Iran is a large country with around 70 million population of different ethnicities, cultures, lifestyles, and socioeconomic status, all of which play an important role in the development of HTN.Citation11,Citation13 Many studies have revealed that urbanization and the adaptation of westernized lifestyle, paced by economic growth and the changes noted in the age pyramid, has resulted in an epidemic of non-communicable chronic diseases (NCCD) such as obesity, metabolic syndrome and subsequently hypertension, diabetes, and eventually cardiovascular diseases in the country.Citation11,Citation14–16
This study was carried out to illustrate the prevalence of hypertension and determine the magnitude of the problem in a group of Iranians representative of the whole population.
Materials and methods
Case selection
The study used the data from the Iranian Multi-centric Osteoporosis Studies (IMOS), a multi-centric cross-sectional study carried out on apparently healthy men and women in urban areas of five great cities (Tehran, Tabriz, Mashhad, Shiraz, and Booshehr) with the main objective of investigating bone health.
Approximately, 5724 subjects met the inclusion criteria and gave their written consent to participate in the study. Blood pressure measurements were not available in 2088 subjects who were recruited in Shiraz and Mashhad; they were, therefore, assumed to be missing at random.
Details on the survey design and methods have been reported previously.Citation17 Briefly, the IMOS used a random cluster sampling design to draw five provincially representative, independent samples of healthy adults excluding those taking medications that could modify bone metabolism, those with hepatic or renal disorders, metabolic bone disease, hypercortisolism, malabsorption, sterility, oligomenorrhea, type I diabetes, malignancy, and immobility for more than 1 week as well as pregnant and lactating women. The Research Ethics Committee of the Endocrine and Metabolism Research Center (EMRC) approved the protocol of this study.
Study protocol
Blood pressure (BP) was measured on the dominant arm by trained nurses using a mercury sphygmomanometer (Reishter, Germany; provided with an appropriate size cuff according to the arm circumference of the subject) in the sitting position after a 10-minute rest period. The subjects were asked not to smoke or consume caffeine during the 30-minute gap preceding the measurement. Systolic BP (SBP) was defined by the onset of the first Korotkoff sound, and diastolic BP (DBP) was indicated by the fifth Korotkoff sound (disappearance of Korotkoff sound).Citation3,Citation18,Citation19
Blood pressure values were classified according to the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure as normal (<120/80 mmHg), Pre HTN (120–139/80–89 mmHg), and Hypertension (≥140/90 mmHg) (Stage I: 140–159/90–99 mmHg, Stage II: ≥160/100 mmHg).Citation3
Aiming to determine the influence of anthropometric variables on blood pressure, individuals were categorized according to their body mass index (BMI) values (underweight <18.5, normal weight 18.5–25, overweight 25–29.9, and obese ≥30 kg/m2).Citation20 The quartiles of waist circumference (WC), hip circumference (HC), and waist-to-hip ratio (WHR) were considered to define each class.
Statistical analysis
Data analysis was performed using SPSS software version 13 (SPSS, Chicago, IL) and analyzed based on a pair-wise approach. Means ± SD or medians were used to express standard descriptive statistics. Categorical variables were expressed as percentages. Differences between groups were assessed using the chi-squared test for qualitative variables and Student's t-test for normally distributed quantitative variables with a level of significance of 5%.
Pearson’s coefficient was calculated for the correlation. Analysis of covariance (ANCOVA) was performed to describe the influence of WC, HC, and WHR, in addition to BMI on the SBP and DBP endpoint variables. The significance level was chosen as 0.05.
Results
Some 1242 individuals from Tehran (21.7%), 1200 from Tabriz (21%), and 1194 from Booshehr (20.9%) were enrolled in the study. From among the studied individuals 1385 (44.6%) were male. The mean age of the participants was 42.39 ± 14.01 years. The blood pressure values of 3049 of these subjects were available.
Overall, 26.21% of the studied cases were estimated to be hypertensive [546 (17.6%) had stage I and 274 (8.8%) had stage II hypertension] and an additional 1441 (47.1%) were reported to have pre-hypertension. Comparing the individuals of each of the three blood pressure groups, there was a significant difference in their anthropometric and blood pressure variables (all p values were <0.001) ().
Table 1. Demographic data based on HTN classificationa.
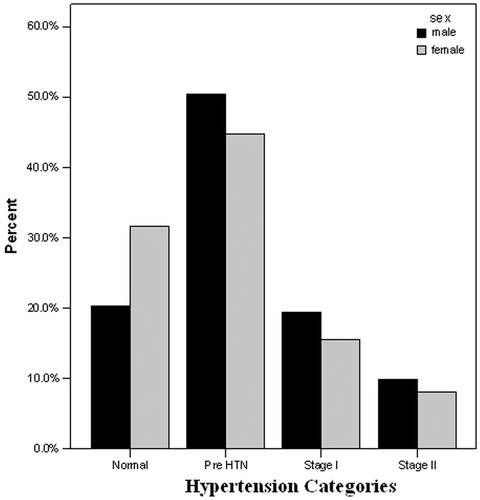
SBP was 4.74 mmHg greater in males (p value <0.001), whereas DBP was 2.65 mmHg greater in females (p value <0.001). Hypertension however was more common in men than women (29.3% vs. 23.5%, 95% CI: 0.612–0.869, p value <0.001) (). The condition was also more prevalent among older individuals and those who lived in Tehran.
Figure 1. The prevalence of hypertension based on gender.
The severity of hypertension based on the participant’s age is outlined in . Each year increase in age was associated with 1.070 higher risk of developing hypertension (p value <0.001), adding that males were at a 0.740 greater chance of developing the condition (p value <0.001). Hypertension stage III was particularly more prevalent among men of all age groups. Age-specific prevalence rates increased significantly in women aged ≥20 and men aged ≥30 years for both diastolic and systolic blood pressure. As for mean arterial pressure (MAP), a similar pattern was noted in both genders ().
Figure 2. The difference between the estimated mean arterial blood pressure (MAP) in females and males based on different age groups. (The highest differences between the two genders are seen in the 20–29 age group.)
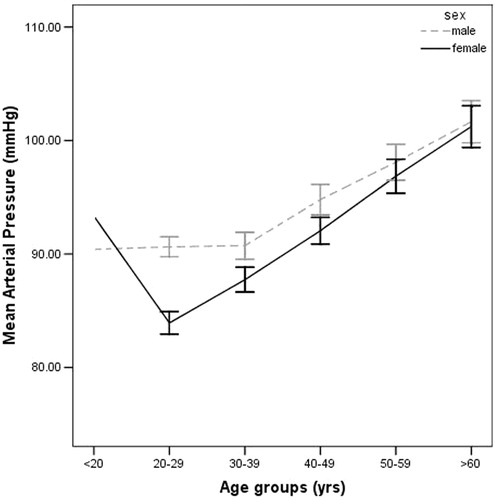
Table 2. Estimates of prevalence of hypertension and pre-hypertension among different age groups.
In logistic regression model, BMI changes were significantly associated with an increased risk of developing hypertension (p < 0.001). There was a trend toward increased chance of developing HTN across the WC, HC, and WHR quartiles (p < 0.001).
Discussion
Non-communicable diseases particularly hypertension imposes a heavy burden on many countries worldwide; the estimated total number of adults with hypertension living in different parts of the world in 2000 was 932 million.Citation21 While hypertension is more frequent in European and American countries, the prevalence of the condition is surging rapidly in most developing countries, turning hypertension into a major public health concern.Citation22 In this context, the Middle East, in which Iran is located, is considered as one of the world’s worst hit countries as in this region hypertension is anticipated to affect the economically productive age of 45 to 64 years rather than the elderly who are commonly affected in most developed countries.Citation23,Citation24
The East Mediterranean Regional Office (EMRO) of the WHO stated in a 2002 report that the prevalence of hypertension in the region covered by that office was 26%.Citation25 Among the Persian Gulf countries, where approximately one-quarter of the population were hypertensive, the prevalence of the condition is reported to be about 25.6% in Saudi Arabia, 26.3% in Kuwait, 27–33.1% in Oman, and 36.6% in United Arab Emirates.Citation26–31
This study revealed the prevalence of hypertension to be 26.21% (23.5% in females and 29.3% in males), which corroborates to previous studies conducted in the same field in Iran. The third national Surveillance of Risk Factors of Non-Communicable Diseases (SuRFNCD) conducted on 5278 Iranian adults in 2007 revealed the high prevalence of diabetes, hypertension, obesity, central obesity, and dyslipidemia in the country. The study reported the prevalence of hypertension to be about 26.6% (28.6% in females and 24.7% in males).Citation32 Another national study conducted in 2005 also showed 25.2% (24.8% in females and 25.5% in males) of the Iranians are hypertensive.Citation33
Considering the results of a systematic review published by Haghdoost et al. in 2008, the overall estimation of HTN, based on the data extracted from Iranian Health Profile Survey (IHPS) and separate published studies, in the 30–55 and >55-year-old population was 12.5% and 22.1%, respectively.Citation11 According to the results of separate studies, Tehran (47.0%) and Ghazvin (6.9%) had the highest and lowest prevalence of HTN. Based on IHPS results, however, these rates were seen in East-Azerbaijan (24.1%) and Sistan and Baluchestan (8.8%), correspondingly. This comes while this study similarly reported Tehran (29.15%) to have the highest prevalence rate of the condition among the studied provinces.Citation34–40
Taken as a whole, a considerable number of studies conducted in Iran and across the globe have reported the problem to be more common among females, older age groups, and those living in urban areas.Citation6,Citation8,Citation11,Citation32,Citation41–44 In view of these studies, higher body mass index (BMI), their lifestyles, the use of oral contraceptives, and menopause are among possible factors contributing to the greater risk of HTN in women.Citation11,Citation41,Citation45 In line with the APCSC study and certain studies conducted in the region, this study reported hypertension to be more prevalent among elderly men.Citation29,Citation46,Citation47 Higher frequency of physician contacts with women along with higher awareness and better control in this population due to factors including sex-related differences in vascular wall properties and the efficiency of antihypertensive medications may be among potential factors accounting for higher prevalence of hypertension among elderly men.Citation8,Citation22,Citation48
Similar to previous studies, the present research showed the prevalence of HTN in Iranian population to be age dependent, adding that the elderly are at a greater risk of developing stage II hypertension. It also revealed that by each year increase in age, the prevalence of HTN increases around 1.070.Citation11,Citation15
The fact that the prevalence of hypertension is rising in the context of progressive rise in age and BMI is of particular concern in public health policy as well as medical care perspective, turning effective prevention, detection, and treatment of the condition into one of the most important goals aiming to halt and reverse this rising tide of hypertension prevalence.
In the present population-based study, hypertension was assessed through self-report and thus a potential bias of undiagnosed underlying diseases, therefore, is probable. Additionally, the cross-sectional nature of this study has precluded the causal inferences regarding the prevalence of hypertension in the study. Large prospective studies are needed to better evaluate the impact of these anthropometric variables on blood pressure regulations.
Moreover, this study was an observational study in which blood pressure was measured in a single session through the auscultatory method; some subjects, therefore, may have been misclassified as having borderline high blood pressure.
Conclusion
The noticeably high prevalence of hypertension reported in this study points out the urgent need to educate individuals regarding the consequences of having high blood pressure and to adopt certain policies and preventive interventions at national scale. These measures may include following more optimal and healthy dietary plan, getting engaged in regular physical activity, and the adaptation of other behavioral approaches required to target this highly prevalent condition.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Acknowledgements
The authors of this study acknowledge the personnel of the Endocrinology and Metabolism Research Center, the laboratory staff, and all those who kindly cooperated in conducting this study.
References
- Whitworth J, World Health Organization ISoHWG. World Health Organization (WHO)/International Society of Hypertension (ISH) statement on management of hypertension. J Hypertens. 2003;21:1983–1992
- Cutler J, Sorlie P, Wolz M, Thom T, Fields L, Roccella E. Trends in hypertension prevalence, awareness, treatment, and control rates in United States adults between 1988–1994 and 1999–2004. Hypertension. 2008;52(5):818–827
- Chobanian A, Bakris G, Black H, et al. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. National Heart, Lung, and Blood Institute; National High Blood Pressure Education Program Coordinating Committee. Hypertension. 2003;42(6):1206–1252
- Gu D, Reynolds K, Wu X, et al. Prevalence, awareness, treatment, and control of hypertension in China. Hypertension. 2002;40(6):920–927
- Unwin N, Setel P, Rashid S, et al. Noncommunicable diseases in sub-Saharan Africa: where do they feature in the health research agenda? Bull World Health Organ. 2001;79(10):947–953
- Oh J, Hong Y, Sung Y, Barret-Conner E. Prevalence and factor analysis of metabolic syndrome in an urban Korean population. Diabetes Care. 2004;27:2027–2032
- Ordunez P, Silva L, Rodriguez M, Robles S. Prevalence estimates for hypertension in Latin America and the Caribbean: are they useful for surveillance? Rev Panam Salud Publica. 2001;10:226–231
- Wolf-Maier K, Cooper R, Banegas J, et al. Hypertension prevalence and blood pressure levels in 6 European countries, Canada, and the United States. JAMA. 2003;289:2363–2369
- Kearney P, Whelton M, Reynolds K, Whelton P, He J. Worldwide prevalence of hypertension: a systematic review. J Hypertens. 2004;22(1):11–19
- Hajjar I, Kotchen T. Trends in prevalence, awareness, treatment, and control of hypertension in the United States, 1988–2000. JAMA. 2003;290:199–206
- Haghdoost A, Sadeghirad B, Rezazadehkermani M. Epidemiology and heterogeneity of hypertension in iran: a systematic review. Arch Iranian Med. 2008;11(4):444–452
- Mohammadi E, Abedi H, Gofranipour F, Jalali F. Partnership caring: a theory of high blood pressure control in Iranian hypertensives. Int J Nurs Pract. 2002;8:324–329
- Whelton P. Epidemiology of hypertension. Lancet. 1994;344:101–106
- Malekzadeh R, Mohamadnejad M, Merat S, Pourshams A, Etmadi A. Obesity pandemic: an Iranian perspective. Arch Iranian Med. 2005;8:1–7
- Bahrami H, Sadatsafavi M, Pourshams A, et al. Obesity and hypertension in an Iranian cohort study; Iranian women experience higher rates of obesity and hypertension than American women. BMC Public Health. 2006;6:158--166
- Ghanbarian A, Rezaei-Ghaleh N, salehi P, Azizi F. Blood pressure distribution in an Iranian adolescent population: “Tehran Lipid and Glucose study”. Med J Malaysia. 2006;61(4):433–437
- Aghaei Meybodi H, Heshmat R, Maasoumi Z, et al. Iranian osteoporosis research network: background, mission and its role in osteoporosis management. Iranian J Publ Health. 2008;1:1–6
- Tuan N, Adair L, He K, Popkin B. Optimal cutoff values for overweight: using body mass index to predict incidence of hypertension in 18–65-year-old Chinese adults. J Nutr. 2008;138(7):1377–13782
- Lohman T, Roche A, Martorell R. Anthropometrical Standardization Reference Manual. Champaign: Human Kinetics Books; 1988
- Lau D, Douketis J, Morrison K, et al. 2006 Canadian clinical practice guidelines on the management and prevention of obesity in adults and children. CMAJ. 2007;176(8 suppl):1–117
- Kearney P, Whelton M, Reynolds K, Munter P, Whelton P, He J. Global burden of hypertension: analysis of worldwide data. Lancet. 2005;365:217–223
- Fuentes R, Ilmaniemi N, Laurikainen E, Tuomilehto J, Nissinen A. Hypertension in developing economies: a review of population-based studies carried out from 1980 to 1998. J Hypertens. 2000;18(5):521–529
- Boutayeb A, Boutayeb S. The burden of non communicable diseases in developing countries. Int J Equity Health. 2005;4(1):2--9
- Lopez A, Mathers C, Ezzati M, Jamison D, Murray C. Global and regional burden of disease and risk factors, 2001: systematic analysis of population health data. Lancet. 2006;367(9524):1747–1757
- EMRO. The Forty-Ninth Session of the WHO Regional Committee Regional Office for the Eastern Mediterranean in Cairo; 2002
- Al-Nozha M, Ali M, Osman A. Arterial hypertension in Saudi Arabia. EMHJ. 1998;4(382):170–174
- Al-Hosani H. Health for all in the United Arab Emirates. EMHJ. 2000;6(838):838--840
- Hasab A, Jaffer A, Hallaj Z. Blood pressure patterns among the Omani population. EMHJ. 1999;5:46–54
- Al Riyami A, Afifi M. Hypertension in Oman: distribution and correlates. J Egypt Public Health Assoc. 2002;77(3–4):383–407
- El-Reshaid K, Al-Owaish R, Diab A. Hypertension in Kuwait: the past, present and future. Saudi J Kidney Dis Transpl. 1999;10(3):357–364
- Al-Said J. The prevalence of hypertension in Persian Gulf countries and its correlation with demographic and socio-economic factors. J Hypertens. 2005;23(6):1275–1277
- Esteghamati A, Meysamie A, Khalilzadeh O, et al. Third national surveillance of risk factors of non-communicable diseases (SuRFNCD-2007) in Iran: methods and results on prevalence of diabetes, hypertension, obesity, central obesity, and dyslipidemia. BMC Public Health. 2009;9:167–177
- Esteghamati A, Abbasi M, Alikhani S, et al. Prevalence, awareness, treatment, and risk factors associated with hypertension in the Iranian population: the national survey of risk factors for noncommunicable diseases of Iran. Am J Hypertens. 2008;21(6):620–626
- Azizi F, Esmaillzadeh A, Mirmiran P. Obesity and cardiovascular risk factors: an epidemiological study in Tehran. Iran J Endocrinol Metabol. 2004;5(suppl 4):389–397
- Mirmiran P, Azadbakht L, Azizi F. The predictors of cardiovascular risk factors in adolescents: Tehran Lipid and Glucose Study. J Shaheed Beheshti Univ Med Sci Health Serv. 2003;3:175–184
- Navaei L, Mehrabi Y, Kimiagar M, Azizi F. Epidemiologic survey on hypertension and its relation with obesity, diabetes, and hyperlipidemia in Islamshahr, Iran. J Shaheed Beheshti Univ Med Sci Health Serv. 1998;2:40–52
- Navaii L, Mehrabi Y, Azizi F. An epidemiologic study of hyperlipidemia, obesity, and hypertension in Tehran villages. Iranian J Endocrinol Metabol. 2000;8:253–263
- Azizi F, Saadat N, salehi P, Emami H. Glucose intolerance and cardiovascular risk factors in Tehran urban population: “Tehran Lipid and Glucose Study”. Iran J Endocrinol Metabol. 2001;12:247–256
- Azizi F, Emami H, salehi P, Ghanbarian A, Mirmiran P, Mirbolooki M. Cardiovascular risk factors in the elderly: Tehran Lipid and Glucose Study (TLGS). Iran J Endocrinol Metabol. 2003;17:3–14
- Ghanbarian A, Majid M, Rahmani M, Sarraf-Zadeh A, Azizi F. Distribution of blood pressure and prevalence of hypertension in Tehran adult population: Tehran Lipid and Glucose Study. Iran J Endocrinol Metabol. 2003;17:425–435
- Efstratopoulos A, Voyaki S, Baltas A, et al. Prevalence, awareness, treatment, and control of hypertension in Hellas, Greece. Am J Hypertens. 2006;19(1):53–60
- Sadeghi M, Roohafza H, Kelishadi R. Blood pressure and associated cardiovascular risk factors in Iran: Isfahan Healthy Heart Programme. Med J Malaysia. 2004;59(4):460–467
- Altun B, Arici M, Nergizoglu G, et al. Prevalence, awareness, treatment and control of hypertension in Turkey (the PatenT study) in 2003. J Hypertens. 2005;23(10):1817–1823
- Gupta R. Trends in hypertension epidemiology in India. J Hum Hypertens. 2004;18:73–78
- Writing Group for the Women’s Health Initiative Investigators. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results from the women's health initiative randomized controlled trial. JAMA. 2002;288:321–333
- Martiniuk A, Lee C, Lawes C, et al. Hypertension: its prevalence and population-attributable fraction for mortality from cardiovascular disease in the Asia-Pacific region. J Hypertens. 2007;25(1):73–79
- Al-Nozha M, Abdullah M, Arafah M, et al. Hypertension in Saudi Arabia. Saudi Med J. 2007;28(1):77–84
- Inamo J, Langb T, Atallahc A, et al. Prevalence and therapeutic control of hypertension in French Caribbean regions. J Hypertens. 2005;23:1341–1346