
Abstract
Aim: to investigate the therapeutic effects of oral carbonic adsorbent on rats with early-stage renal failure. Methods: The early-stage renal failure model was established with three-fourth subtotal nephrectomy Wistar rats. Four weeks after the subtotal nephrectomy, the rats were randomly divided into four groups: (1) adsorbent diet (AD) rats; (2) low protein diet (LPD) group; (3) low protein and AD rats; and (4) normal diet rats as control (ctrl) group. Sham operation group is set as well. The therapeutic effects of adsorbent were examined after 15 weeks treatment. Results: The level of 24 hours urinary protein excretion, serum creatinine (Scr), index of glomerulosclerosis (GSI) and tubulointerstitial fibrosis score (TIFS) of rats with adsorbent or LPD treatment are significantly lower than ctrl group rats. The combination of adsorbent and LPD lowered level of 24 hours urinary protein excretion, Scr, index of GSI and TIFS compared with LPD or adsorbent treatment alone. Conclusion: Both AST-120 and LPD treatment lowered the Scr and blood urea nitrogen level as well as ameliorated the proteinuria and glomerular and tubulointerstitial damage of rats with early stage renal failure. The combined treatment of oral carbonic adsorbent and LPD showed greater therapeutic effects.
Introduction
Chronic kidney disease (CKD) is considered as a major public health concern worldwide. Approximately 13% of adults in America suffer from CKD,Citation1 and research in Beijing shows that the morbidity of CKD in adults is up to 13% in China.Citation2 CKD, developing into end-stage renal disease (ESRD) eventually, seriously affects the living condition of patients. The survival rate of ESRD remains low, and the cost of treatment is relatively high. Evidence demonstrated that early detection and treatment of CKD can slow the progression of disease and other adverse outcomes.Citation3,Citation4 Despite the use of conventional therapy, such as angiotensin receptor blocker or angiotensin-converting enzyme inhibitor treatment, finding other effective methods of early intervention and precaution to delay CKD developing into ESRD is of great importance.
In the progression of CKD, uremic toxins, mostly protein catabolism waste products, accumulate in blood and/or tissues, causing pathological and physiological changes in other organs and accelerating renal damage,Citation5,Citation6 and protein-bound uremic toxins such as p-cresyl sulfate and indoxyl sulfate are difficult to be removed with currently available dialysis techniquesCitation7. An effective way to reduce serum uremic toxins is of great importance in ameliorating CKD progression.
Adsorbing uremic toxin by carbonic adsorbent in intestine is a therapy with intensive studies. AST-120, a kind of oral carbonic adsorbent, has been available in Japan since 1991, and subsequently Korea (2005), and the Philippines (2010) as an agent to prolong the time to initiation of hemodialysis and for improvement of uremic symptoms in patients with CKD.Citation8 Animal experiment and clinical research demonstrated that AST-120 lowered the level of serum creatinine (Scr) and blood urea nitrogen (BUN) as well as ameliorate renal failure in CKD rats and patients.Citation9–11 Notably, research supported the beneficial effects of AST-120 with regard to preserving renal function specifically in patients with early-stage diabetic nephropathy.Citation12 Low protein diet (LPD) is an essential and common therapeutic measure in CKD.Citation13 Restriction of dietary protein intake lowers the excretion of BUN and protects kidney.Citation14 Noticeably, some research confirmed synergistic effect of carbonic adsorbent and LPD on CKD.Citation15,Citation16
Early treatment is of vital importance for CKD patients to prolong the time to initiation of hemodialysis and to slow the progression of renal failure. However, the effect of carbonic adsorbent on early-stage CKD is not very clear. In addition, the effect of combined therapy of AST-120 and LPD in early-stage CKD is still unknown. To investigate the effects of AST-120 on early-stage renal failure kidneys and evaluate its synergistic effects with LPD treatment, we established three-fourth subtotal nephrectomy (3/4 NX) rats as early-stage CKD animal model and studied the therapeutic effects of AST-120 alone and with LPD on their kidneys.
Materials and methods
Reagents
Reagents were obtained from the following companies: oral carbonic adsorbent AST-120 (Antuoxin Pharmaceutical Technology Co., Ltd, Shanghai, China); LPD food and food for AST-120 diet (Slaccas Experimental Animal Co., Ltd., Shanghai, China); and urine protein kit (C035, Bioengineering Institution, Nanjing, China).
Subtotal nephrectomy and shame operation
Subtotal nephrectomy rat is a common and mature renal failure animal model. The mechanism includes proteinuria, glomerulosclerosis (GSI), tubulointerstitial fibrosis, hypofunction and hemodynamic changes such as hypertransfusion and hyperfiltration in remained kidney. The amount of remained nephron directly affects the progress and the prognosis of the disease. Since we aimed at observing the renal function and construction of early-stage renal failure rats, 3/4 NX, which establishes early-stage CKD,Citation11,Citation15 was established instead of five-sixth subtotal nephrectomy.
Thirty male Wistar rats, which weighed 220–240 g, were provided by Experimental Animal Center, Medical School of Fudan University, Shanghai, China. Twenty-four rats were established with 3/4 NX. Rats were anesthetized with 5% sodium pentobarbital (50 mg/kg, i.p.) via intraperitoneal injection. Left kidney was exposed by median abdominal incision, and the upper one-fourth and the lower one-fourth of left kidney was removed. A week later, the right kidney was removed completely through right dorsal incision. The removed kidney tissue was weighed, and the proportion of removed kidney (proportion of NX) was calculated. Six sham-operated rats underwent anesthesia and manipulation of the renal pedicles.
Experimental diets
From the first experimental day to four weeks after the remove of right kidney, rats were feed with normal diet (containing 18% of protein, provided by experimental animal center of medical school of Fudan University). Four weeks after the removal of right kidney, rats were randomly divided into four groups: adsorbent diet rats (AD, n = 6); LPD group (n = 6); low protein and AD rats (AD + LPD, n = 6); and normal diet rats (control [ctrl], n = 6). AD rats were fed powder chow containing 5% carbonic adsorbent and 18% protein; LPD rats were fed powder chow with 6% protein; AD + LPD rats were fed powder chow with 5% carbonic adsorbent and 6% protein; and ctrl group rats were fed a normal diet as previously described.
Measurement of urinary and serum samples and blood pressure
Four weeks after the removal of right kidney, blood samples were gathered by retro orbital vein puncture for examining the baseline of Scr, BUN, hemoglobulin (Hb) and serum albumin (Alb). Metabolic cages were used for 24 hours urinary protein excretion (24 h Upro) testing. Systolic blood pressure was measured non-invasively by tail-cuff sphygmomanometer.
Weight testing was performed every week, and the weekly amount of food intake was recorded. Examining of Upro, SBP, Scr, BUN and Alb were performed as previously described every five weeks.
The blood routine, including Scr, Alb and Hb, is tested by automated hematology analyzer, Sysmex KX-21 (Japan). Scr, BUN and Alb were assessed using Hitachi automatic biochemical analyzer (Japan); 24 h Upro was measured by Coomassie brilliant blue method.
Kidney pathology tests
Fifteen weeks after the treatment, the rats were anesthetized with 5% sodium pentobarbital (50 mg/kg, i.p.), and the left kidney was removed after gathering 10 mL blood from the heart.
Renal tissues were 10% formalin-fixed, embedded in paraffin and sections (2 µm) prepared and stained with Masson and Periodic Acid-Schiff (PAS). To detect GSI and tubulointerstitial fibrosis, 50 glomerular areas and 50 tubulointerstitial areas were analyzed under light microscopy. Each glomerulus (or tubulointerstitial area) was graded on a 0–4 scale, which represent sclerotic (or fabric area for tubulointerstitium) area involving 0, 1–25, 26–50, 51–75, or > 75% of the glomerulus (or tubulointerstitium). Scores for all glomeruli were averaged and defined as index of GSI, and scores for all tubulointerstitial areas were averaged and defined as tubulointerstitial fibrosis score (TIFS).
Statistical analysis
Results are expressed as means ± SD. One-way analysis of variance (ANOVA) was used to compare statistics in different groups. Statistical analysis is processed by SPSS, 13.0 (SPSS Inc., Chicago, IL). The two factors and two levels of factorial ANOVA were used to evaluate the interaction between LPD and oral carbonic adsorbent. Values were regarded as significant at two-sided, p < 0.05.
Results
Characteristics of subtotal nephrectomy rats
Subtotal nephrectomy rats showed kidney dysfunction and damage. At week 0, the subtotal nephrectomy rats showed higher Scr, BUN and 24 h Upro and lower Hb compared with sham-operated rats (p < 0.05). Scr, BUN, Alb, BW, SBP, Hb, 24 h Upro and proportion of NX showed no significant differences between the four subtotal nephrectomy groups before dietary treatment (p > 0.05; ). The pathological sections obtained at 15th week showed kidney damage of subtotal nephrectomy rats. Glomerular hypertrophy and focal segmental sclerosis as well as a few global scleroses were observed. Enlarge of Bowman’s capsule, the adhesion of glomerulus and capsule, the capsule wall thickness and glomerular capillary loop stenosis or blocking, proliferation of mesangial cells, increasing of interstitial substance and mesangial area, moderate fibrosis and inflammatory cell infiltration of interstitial substance and a large amount of protein cast was observed as well (). Meanwhile, in the pathological sections of shame operation rats, the glomerulus and vascular wall remained normal, without proliferation of mesangial cells and glomerular capillary loop stenosis. The interstitial substance of shame operation rats showed no significantly inflammatory cell infiltration as well ().
Figure 1. Renal histology in PAS-stained sections (400 ×). Notes: (a) Sham operation group; (b) control group; (c) low protein diet group; (d) AST-120 group; and (e) AST-120 + LPD group. The kidney tissue of AD + LPD, LPD and AD rats are with less proliferation of mesangial cells, increase area and inflammatory cell infiltration of interstitial substance and protein cast compared with ctrl rats. No focal segmental sclerosis and adhesion of glomerulus and capsule was observed ().
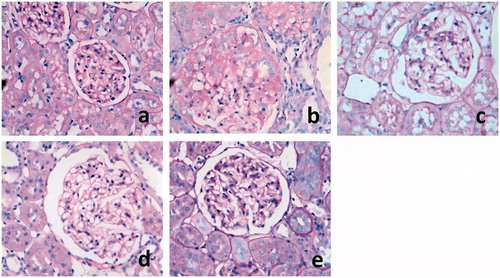
Table 1. Baseline characteristics on week 0.
Effects of adsorbent and LPD treatment
Rats with adsorbent and/or LPD treatment showed preserved kidney function and construction compared with ctrl rats. At the 15th week, AD, LPD and AD + LPD rats showed lower Scr (p < 0.01) and BUN (p < 0.01) compared with ctrl rats ( and ), while ctrl rats showed no significant differences in SBP, BW, Alb and the amount of total food intake (AFI) compared with every other subtotal nephrectomy groups ().
Figure 2. Scr characteristics of rats with early-stage renal failure Notes: Ctrl, control group; LPD, low protein diet group; AD, AST-120 adsorbent group; and AD + LPD, AST-120 + low protein diet group. *Compared with ctrl rats, p < 0.01. †Compared with AD rats, p < 0.01. ‡Compared with LPD rats, p < 0.01.
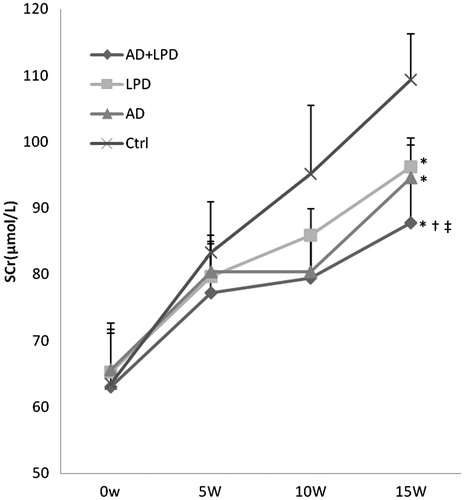
Figure 3. BUN characteristics of rats with early-stage renal failure. Notes: Ctrl, control group; LPD, low protein diet group; AD, AST-120 adsorbent group; and AD + LPD, AST-120 + low protein diet group. *Compared with ctrl rats, p < 0.01. †Compared with AD rats, p < 0.01.
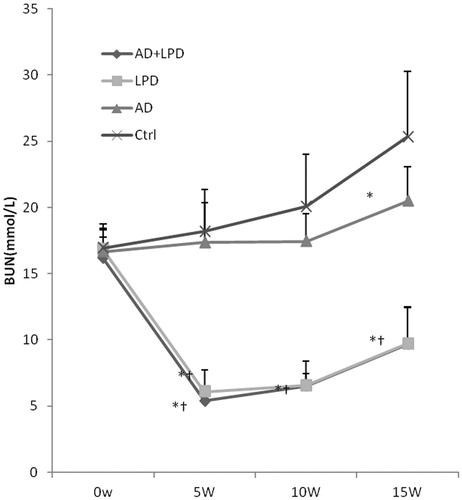
Table 2. WB, SBP, AFI, Alb and Hb statistics at the 15th week.
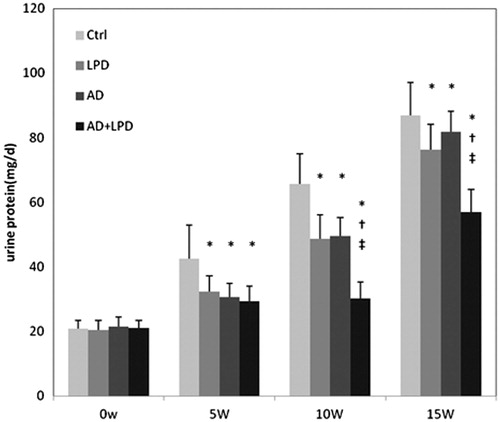
The 24 h Upro of rats progressively increased in every subtotal nephrectomy groups since the beginning of the experiment. The growth of 24 h Upro is slower in AD, LPD, AD + LPD rats compared with ctrl rats. At the 15th week, AD, LPD and AD + LPD rats showed lower 24 h Upro compared with ctrl rats (81.87 ± 6.25 mgd–1, 76.25 ± 7.77 mgd–1, 56.87 ± 7.15 mgd–1 and 96.80 ± 7.53 mgd–1, p < 0.01; ). The pathological sections showed that kidney tissue of AD + LPD, LPD and AD rats are with less proliferation of mesangial cells, increase area and inflammatory cell infiltration of interstitial substance and protein cast compared with ctrl rats. AD + LPD, LPD and AD rats showed smaller GSI and TIFS compared with ctrl rats as well (p < 0.05; ).
Figure 4. Urine protein characteristics of early-stage CKD rats. Notes: Ctrl, control group; LPD, low protein diet group; AD, AST-120 adsorbent group; and AD + LPD, AST-120 + low protein diet group. *Compared with ctrl rats, p < 0.01. †Compared with AD rats, p < 0.01. ‡Compared with LPD rats, p < 0.01.
Effects of combined therapy of adsorbent and LPD
Combined therapy of adsorbent and LPD showed greater renal protective effects compared with separated treatment. At the 5th week and the 10th week, AD + LPD rats showed lower BUN compared with AD rats (p < 0.01). At the 15th week, AD + LPD rats showed lower Scr compared with AD and LPD rats ().
AD + LPD rats showed lower 24 h Upro compared with AD and LPD rats after 15 weeks treatment (p < 0.01; ). AD + LPD rats showed significantly smaller GSI and TIFS compared with LPD and AD rats (p < 0.05; ).
Table 3. Pathological characteristics of remnant kidneys.
Discussion
In our study, subtotal nephrectomy rats showed kidney dysfunction and damage and no rat death reported from the experiment, indicating that 3/4 NX can be a model investigating early-stage CKD and observing the effects of medical treatment to the prognosis of CKD.
AST-120 is an oral intestinal spherical carbon adsorbent consisting of porous carbon particles that are 0.2–0.4 mm in diameter and insoluble in water and common organic solvents.Citation17 Conventional carbon adsorbent is in powder form, unable to effectively absorb uremic toxins and always accumulates in gut, causing abdominal distention and constipation. AST-120 consists of spherical porous carbon particles, which significantly improved the adsorption effect by increasing the superficial area, effectively absorbing toxins in intestine. It adsorbs indole, a precursor of indoxyl sulfate derived from the metabolism of tryptophan by bacteria within the gastrointestinal tract,Citation17 and indoxyl sulfate is a uremic toxin which stimulates progression of both tubulointerstitial fibrosis and glomerular sclerosis in CKD.Citation18 In this experiment, the AD rats with oral carbonic adsorbent treatment for 15 weeks showed lower Upro, Scr, GSI and TIFS than ctrl rats, indicating the renal protection effects on early-stage CKD rats of AST-120.
The use of a low-protein diet in treating CKD dates back many decades. In CKD, a low-protein diet has a minimal effect on the decline in GFR, but it is capable of delaying renal death (i.e., the start of renal replacement therapy).Citation13 In this study, LPD rats showed preserved kidney function and construction compared with ctrl rats, indicating that LPD treatment plays an important role in the treatment of CKD.
LPD and AST-120 treatment work in similar mechanism: LPD ameliorates uremic symptoms through reducing accumulation of protein catabolism waste products, and carbonic adsorbent protects kidney through absorbing uremic toxins in intestine. In our study, AD + LPD rats showed less renal damages compared with LPD rats and AD rats, suggesting the synergistic effect of adsorbent and LPD. AD + LPD and LPD rats showed lower BUN compared with AD rats. However, AD + LPD rats showed no significantly lower BUN compared with LPD rats. This probably resulted from the low BUN in AD + LPD and LPD rats caused by extreme low nitrogen intake of LPD, indicating positive effects on lowering BUN of LPD.
One potential concern of oral carbonic adsorbent therapy would be the risk of loss of essential elements and malnutrition. Research showed that AST-120 has lower adsorption ability for amylase, pepsin, lipase and chymotrypsin than conventional carbon adsorbent.Citation19 In our study, rats in subtotal nephrectomy groups showed no significant differences in BW, Alb and the AFI compared with every other subtotal nephrectomy groups with ctrl rats after 15 weeks’ treatment, which indicate that oral carbonic adsorbent therapy showed no such side effect mentioned above.
Our study suggested renal protective effect of AST-120 as well as the synergistic effect of oral carbonic adsorbent and LPD on early-stage CKD rats. This research provided theoretical evidence for further investigation and clinical researches on early intervention of CKD as well as the evidence to further define the role of AST-120 in CKD treatment.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
This study is supported by Department of Nephrology, Zhongshan Hospital, Fudan University.
Ethical approval
The “Principles of Laboratory animal care” NIH publication Vol 25, No. 28 revised 1996 were followed.
References
- Coresh J, Selvin E, Stevens LA, et al. Prevalence of chronic kidney disease in the United States. JAMA. 2007;298:2038–2047
- Zhang L, Zhang P, Wang F, et al. Prevalence and factors associated with CKD: A population study from Beijing. Am J Kidney Dis. 2008;51:373–384
- Levey AS, Atkins R, Coresh J, et al. Chronic kidney disease as a global public health problem: Approaches and initiatives—A position statement from Kidney Disease Improving Global Outcomes. Kidney Int. 2007;72:247–259
- Hallan SI, Coresh J, Astor BC, et al. International comparison of the relationship of chronic kidney disease prevalence and ESRD risk. J Am Soc Nephrol. 2006;17:2275–2284
- Vanholder R, Baurmeister U, Brunet P, Cohen G, Glorieux G, Jankowski J. A bench to bedside view of uremic toxins. J Am Soc Nephrol. 2008;19:863–870
- Vanholder R, De Smet R, Glorieux G, et al. Review on uremic toxins: Classification, concentration, and interindividual variability. Kidney Int. 2003;63:1934–1943
- Neirynck N, Vanholder R, Schepers E, Eloot S, Pletinck A, Glorieux G. An update on uremic toxins. Int Urol Nephrol. 2013;45:139–150
- Schulman G, Vanholder R, Niwa T. AST-120 for the management of progression of chronic kidney disease. Int J Nephrol Renovasc Dis. 2014;7:49–56
- Schulman G, Agarwal R, Acharya M, Berl T, Blumenthal S, Kopyt N. A multicenter, randomized, double-blind, placebo-controlled, dose-ranging study of AST-120 (Kremezin) in patients with moderate to severe CKD. Am J Kidney Dis. 2006;47:565–577
- Marier JF, Lee J, Kambhampati SR, et al. Effect of repeated oral administrations of the oral adsorbent AST-120 on serum creatinine and other markers of renal function. A randomized controlled study in patients with chronic kidney disease. Am J Nephrol. 2006;26:136–141
- Kobayashi N, Maeda A, Horikoshi S, Shirato I, Tomino Y, Ise M. Effects of oral adsorbent AST-120 (Kremezin) on renal function and glomerular injury in early-stage renal failure of subtotal nephrectomized rats. Nephron. 2002;91:480–485
- Konishi K, Nakano S, Tsuda S, Nakagawa A, Kigoshi T, Koya D. AST-120 (Kremezin) initiated in early stage chronic kidney disease stunts the progression of renal dysfunction in type 2 diabetic subjects. Diabetes Res Clin Pract. 2008;81:310–315
- Bellizzi V. Low-protein diet or nutritional therapy in chronic kidney disease? Blood Purif. 2013;36:41–46
- Hostetter TH, Meyer TW, Rennke HG, Brenner BM. Chronic effects of dietary protein in the rat with intact and reduced renal mass. Kidney Int. 1986;30:509–517
- Imai E, Takenaka M, Isaka Y, et al. Carbonic adsorbent AST-120 retards progression of renal failure by additive effect with ACEI and protein restriction diet. Clin Exp Nephrol. 2003;7:113–119
- Sanaka T, Fujimoto K, Niwayama J, et al. Effect of combined treatment of oral sorbent with protein-restricted diet on change of reciprocal creatinine slope in patients with CRF. Am J Kidney Dis. 2003;41:S35–S37
- Niwa T, Emoto Y, Maeda K, Uehara Y, Yamada N, Shibata M. Oral sorbent suppresses accumulation of albumin-bound indoxyl sulphate in serum of hemodialysis patients. Nephrol Dial Transplant. 1991;6:105–109
- Niwa T, Ise M. Indoxyl sulfate, a circulating uremic toxin, stimulates the progression of glomerular sclerosis. J Lab Clin Med. 1994;124:96–104
- Kanai F, Takahama T, Yamazaki Z, Idezuki Y, Koide K. Effects of oral adsorbent on experimental uremic rats. Nihon Jinzo Gakkai Shi. 1986;28:1249–1259