
Abstract
Background/aims: Cardiovascular diseases are major causes of mortality in chronic renal failure patients before and after renal transplantation. Among them, coronary disease presents a particular risk; however, risk predictors have been used to diagnose coronary heart disease. This study evaluated the frequency and importance of clinical predictors of coronary artery disease in chronic renal failure patients undergoing dialysis who were renal transplant candidates, and assessed a previously developed scoring system. Methods: Coronary angiographies conducted between March 2008 and April 2013 from 99 candidates for renal transplantation from two transplant centers in São Paulo state were analyzed for associations between significant coronary artery diseases (≥70% stenosis in one or more epicardial coronary arteries or ≥50% in the left main coronary artery) and clinical parameters. Results: Univariate logistic regression analysis identified diabetes, angina, and/or previous infarction, clinical peripheral arterial disease and dyslipidemia as predictors of coronary artery disease. Multiple logistic regression analysis identified only diabetes and angina and/or previous infarction as independent predictors. Conclusion: The results corroborate previous studies demonstrating the importance of these factors when selecting patients for coronary angiography in clinical pretransplant evaluation.
Introduction
Chronic kidney disease (CKD) is a growing worldwide health problem, with the increased incidence and prevalence of kidney failure having direct effects on clinical outcomes for people affected and high costs to health systems. Cardiovascular disease is often associated with CKD, and CKD is a potent risk factor for cardiovascular morbidity and mortality. Mortality from cardiovascular disease is 10–30 times greater in dialysis patients than in the general population.Citation1 Studies have shown that cardiovascular risk remains elevated even after renal transplantation.Citation2 Reducing mortality in dialysis patients requires efforts to reduce cardiovascular mortality, and evaluation of coronary artery disease should form part of the routine evaluation of cardiovascular renal pretransplant risk.
There are different ways to stratify the risk of coronary artery disease in renal transplant candidates based on clinical cardiovascular risk. These include age, cumulative risk with the presence of other risk factors, pre-existing cardiovascular disease, and noninvasive tests.Citation3
The sensitivity of noninvasive methods for detection of coronary disease is satisfactory in studies of non-numeric population. Studies have demonstrated that the sensitivity and/or specificity for detecting significant coronary artery disease by myocardial scintigraphy or echocardiography with stress in chronic renal failure patients is variable and generally low, being <60%.Citation3,Citation4
Coronary angiography is the best method for detecting significant coronary artery disease and determining cardiac risk in patients aged over 50 years, with CKD or with risk factors such as pre-existing diabetes and cardiovascular disease.Citation3 In multivariate analysis, the only predictor of a cardiac event was coronary stenosis (≥70%, p = 0.003).Citation3 However, coronary angiography should be avoided in populations at low risk.
Clinical studies have proposed algorithms to help select candidates for renal transplantation for coronary angiography.Citation5–13 However, validation of these algorithms in various patient populations is scarce. The objective of this study was to evaluate the frequency and duration of clinical predictors of coronary artery disease in chronic renal failure patients on dialysis who were candidates for renal transplantation at two centers in São Paulo state, and to validate a previously developed algorithm.Citation5
Materials and methods
This was an observational, partly retrospective study using data obtained between March 2008 and April 2013 of patients from two kidney transplant centers in São Paulo state. The study was approved by the research ethics committee of both institutions. All patients analyzed prospectively provided informed consent. An exemption was provided by the ethics committees for retrospective analysis.
Chronic renal dialysis patients who were candidates for renal transplantation and over 18 years were included. The following risk factors were assessed: hypertension, diabetes, dyslipidemia, and smoking as defined by clinical history; obesity or being overweight as defined by body mass index; and a history of cardiovascular disease and peripheral artery disease, stroke, infarction, angina, and chronic heart failure as defined by the presence of compatible symptoms according to the Boston criteriaCitation14,Citation15 or left ventricular dysfunction in imaging studies with fractions <50% ejection. Age, gender, race, time on dialysis, and weekly dose of erythropoietin were analyzed, as were the following laboratory data: alkaline phosphatase, albumin, parathyroid hormone (PTH), phosphorus, and hematocrit.
All patients underwent coronary arteriography. Significant lesions ≥50% in the left main coronary artery or ≥70% in the left anterior descending (or its diagonal branches), the circumflex (or its marginal branches), and the right coronary artery by visual estimation were considered.
Statistical analysis
A sample size of 100 patients was sufficient to detect a 15% difference in frequency of an attribute with an alpha error of 0.05 and a beta error of 0.2. Analyses were performed using SPSS 12.0.1 software (Chicago, IL).
Univariate logistic regression was used to determine the association between coronary disease and age, gender, race, smoking, overweight or obesity, diabetes, physical inactivity, hypertension, dyslipidemia, heart failure, peripheral arterial disease, previous stroke, previous myocardial infarction or angina, and weekly dose of erythropoietin. The following laboratory data were also analyzed: alkaline phosphatase, albumin, PTH, phosphorus, and hematocrit. Variables associated with the outcome variable at p < 0.05 were selected for multivariate logistic regression.
A receiver operating characteristic curve was plotted to verify the discriminatory power of the formula previously proposed in the literature in relation to the current study.Citation8 The best cut-off point was determined by the highest sum of specificity and sensitivity (index Yuden). The formula was: Probability of coronary disease = {[(age × 0.4) + (DM × 9) + (CVD × 14] × 2} − 23. Age in years, where DM, diabetes mellitus, CVD, cardiovascular diseases. When DM and CVD present = 1.
Parametric data are expressed as mean ± standard deviation, nonparametric data as median and interquartile range, and categorical variables as percentages.
Results
Of the 129 patients on dialysis and in the renal transplant candidate program eligible to participate in the study, 23 were excluded (3 died prior to completion of coronary angiography: 1 polytrauma, 1 acute pulmonary edema, 1 aspiration pneumonia; and 20 did not provide consent). Of the remaining 106 patients undergoing dialysis and who underwent coronary angiography between March 2008 and April 2013, 7 were excluded because of recording clinical data and test analysis failures. Ninety-nine patients were enrolled, 33 of whom were analyzed prospectively and 66 analyzed retrospectively because they had previously had a coronary angiography. Thirteen patients were from transplant unit A and 53 from transplant unit B. The prospective group (33%) had a mean age of 49 ± 11.2 years and a low frequency of prior cardiovascular disease.
The study group was composed by 63 males and 36 females aged 54 ± 9.7 years. There were 99 patients; 80% white, 8% black and 11% mestizo and one of undetermined race. Cause of renal failure, that was clinically diagnosed, was diabetic nephropathy in 52 patients (53%), hypertensive nephrosclerosis in 28 patients (28%), glomerulopathy in 7 patients (7%), and other pathologies in the remainder. Median time on dialysis was 23 months, range 0–204 months. Fourteen patients were smokers (14%), 42 were overweight or obese (44%), diabetic (60, 61%), hypertensive (92, 93%), and dyslipidemia was present in 52% of 87 patients who presented with this condition. Heart failure occurred in 11 patients (11%), 14 patients had a history of peripheral arterial disease (14%), 11 patients had prior stroke (11%) and 27 patients (27%) had angina or previous infarction. Risk factors are depicted in .
Table 1. Demographic and clinical characteristics of dialysis patients candidates for renal transplantation submitted to coronariography.
Variables associated with significant coronary disease in univariate logistic regression analysis were selected to multiple analyses and the other was included.
With multivariate analysis, diabetes and angina or previous infarction were identified as independent predictors of significant coronary artery disease (). shows the frequency of coronary heart disease in accordance with the presence of diabetes and previous myocardial infarction or angina. Thirty-one percent of the total sample showed significant coronary artery disease in at least one epicardial artery. In the prospective group, 24% (8 of 33) had significant coronary disease.
Figure 1. Frequency of coronary heart disease according to the presence of diabetes and angina or prior myocardial infarction.
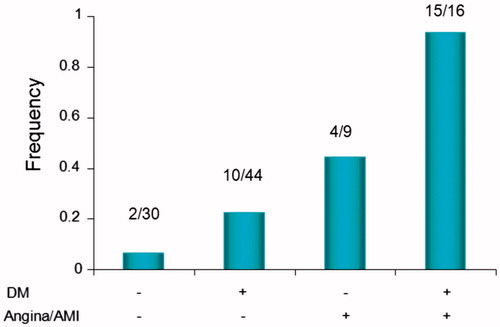
Table 2. Multiple logistic regression analysis.
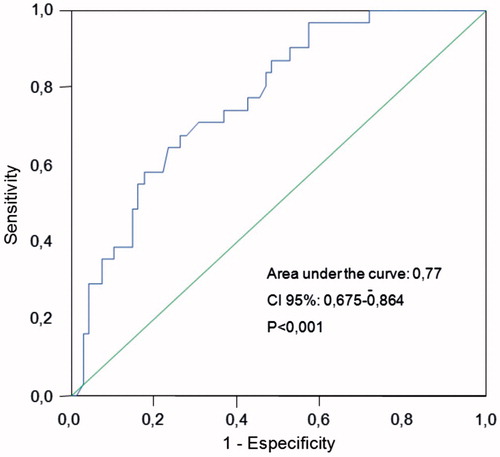
To evaluate the calibration of the previously proposed scoring system, the frequency of significant coronary artery disease predicted and observed among patients grouped according to results of the formula proposed by Gowdak et al. in progressive bands in ascending order (0–20%, 21–40%, 41–60% and 61–80%) was analyzed.Citation5 The proposed scoring system showed good calibration (). shows the receiver operating characteristic (ROC) curve for the discriminatory power of the formula applied to the present series. Excellent discriminatory power was observed. Using ≥51% as the cut-off value, a sensitivity of 68% and a specificity of 74% were obtained. The positive predictive value was 52% and the negative predictive value was 82%.
Figure 2. Frequency of coronary heart disease obtained in this study according to the previously predicted by the formula proposed by Gowdak et al.Citation5.
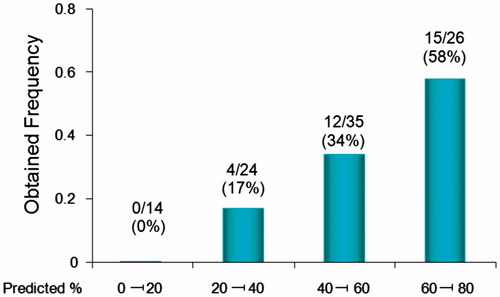
Figure 3. ROC curve related to the discriminatory power of a previously developed formulaCitation5 applied to the present series.
Discussion
Coronary heart disease is a major cause of mortality in patients with renal disease, and diagnosis is challenging.Citation16–25 The current study evaluated the frequency and clinical predictors of coronary artery disease in chronic renal failure patients on dialysis and renal transplant candidates and sought to validate a previously developed clinical scoring system.Citation5 Coronary disease was common and independently associated with diabetes and previous myocardial infarction or angina. Data from this study validates, for the studied region, the clinical scoring system developed in São Paulo.
In the literature, there are well established risk factors associated with coronary disease that in this study was not associated with the risk of coronary heart disease. This may possibly be because CKD is itself a risk factor, which overcomes the influence of other factors.
The current work supports the premise that it is mandatory for diabetic dialysis patients to perform cardiac catheterization during the pretransplantation evaluation. This exam is compelling too in dialysis patients with clinical manifestations of coronary heart disease. As a corollary, it is unnecessary for these patients to undergo noninvasive tests for coronary ischemia, such as myocardial scintigraphy or echocardiography with pharmacologic stress. Patients with neither diabetes nor prior cardiovascular disease do not require a cardiac catheterization, if this group had normal noninvasive tests.
The frequency of coronary artery disease in this study was slightly lower than that predicted by the formula (). Possible explanations may be the lower frequency of smokers and lower mean age in this sample compared with the sample that generated the formula. In particular, the group that underwent catheterization prospectively had a lower frequency of previous cardiovascular disease and a low age (data not shown).
This study had some limitations. Part of the study patients were analyzed retrospectively, with the limitations inherent in this study design. The data obtained from medical records is not so reliable than the data of prospective studies, but the patients with failed data were excluded from analysis in the current study. The indication for coronary angiography in patients studied retrospectively was based on guidelines which recommend this examination for all patients at high clinical risk, for example, older than 50, diabetic, patients with previous cardiovascular disease and symptomatic; whereas for a portion of patients prospectively evaluated (33% of the total), coronary angiography was routinely performed regardless of clinical risk. This produced a subgroup of patients at lower risk and therefore lower frequency of coronary disease. However, such bias changes only the frequency of coronary heart disease in this group and does not modify the predictive ability of the clinical variables studied. Besides this limitation, the number of patients is small, but sufficient to demonstrate statistical significances.
Conclusion
The previously developed formula was validated in this study and helps to determine the probability of coronary disease when assessing patients on a renal dialysis pretransplant program. The traditional risk factors, except for diabetes, were not associated with the likelihood of coronary disease in this study. Angina and/or previous myocardial infarction or diabetes were strong predictors of significant coronary disease, and may help identify patients who should be referred for coronary angiography when undergoing renal pretransplant evaluation.
Study association
This study consists of postgraduate research conducted by Emerson Albuquerque Seixas at the Faculty of Medicine of Botucatu.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
- Sarnak MJ, Levey AS, Schoolwerth AC, et al. Kidney disease as a risk factor for development of cardiovascular disease: A statement from the American Heart Association councils on kidney in cardiovascular disease, high blood pressure research, clinical cardiology, and epidemiology and prevention. Circulation. 2003; 108:2154–2169
- Stewart G, Jardine AG, Briggs JD. Ischemic heart disease following renal transplantation. Nephrol Dial Transplant. 2000;15:269–277
- Lima JJ, Sabbaga E, Vieira ML, et al. Coronary angiography is the best predictor of events in renal transplant candidates compared with noninvasive testing. Hypertension. 2003;42:263–268
- Holley JL, Fenton RA, Arthur RS. Thallium stress testing does not predict cardiovascular risk in diabetic patients with end-stage renal disease undergoing cadaveric renal transplantation. Am J Med. 1991;90:563–570
- Gowdak LH, Paula FJ, Cesar LA, et al. A new risk score model to predict the presence of significant coronary artery disease in renal transplant candidates. Transplant Res. 2013;2:18
- Gowdak LH, de Paula FJ, César LA, et al. Screening for significant coronary artery disease in high-risk renal transplant candidates. Coron Artery Dis. 2007;18:553–558
- Braun WE, Philips D, Vidt DG, et al. Coronary arteriography and coronary artery disease in 99 diabetic and nondiabetic patients on chronic hemodialysis or renal transplant programs. Transplant Proc. 1981;13:128–135
- Lewis MS, Wilson RA, Walker KW, et al. Validation of an algorithm for predicting cardiac events in renal transplant candidates. Am J Cardiol. 2002;89:847–850
- Foley RN, Parfrey PS, Sarnak MJ. Clinical epidemiology of cardiovascular disease in chronic renal disease. Am J Kidney Dis. 1998;32:S112–S119
- Levey AS, Beto JA, Coronado BE, et al. Controlling the epidemic of cardiovascular disease in chronic renal disease: What do we know? What do we need to learn? Where do we go from here? National Kidney Foundation Task Force on Cardiovascular Disease. Am J Kidney Dis. 1998;32:853–906
- National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: Evaluation, classification and stratification. Am J Kidney Dis. 2002;39(2 Suppl. 1):S1–S266
- Bucharles SGE, Varela AM, Barberato SH. Avaliação e manejo da doença cardiovascular em pacientes com doença renal crônica. J Bras Nefrol. 2010;32(1):120–127
- Rostand SG, Kirk KA, Rutsky EA. Dialysis associated ischemic heart disease: Insights from coronary angiography. Kidney Int. 1984;25:623–629
- Bocchi EA, Braga FG, Ferreira SM. III Diretriz Brasileira de Insuficiência Cardíaca Crônica. Arq Bras Cardiol. 2009;93(1 Suppl. 1):3–70
- Libby P, Bonow RO, Mann DL, et al. Braunwald’s Heart Disease a Textbook of Cardiovascular Medicine. 8th ed. Philadelphia, PA: Saunders Elsevier; 2008:206, 253–255, 259–61, 376–378
- Martin LC, Franco RJ. A doença renal como fator de risco cardiovascular. Arq Bras Cardiol. 2005;85:432–436
- Kasiske BL. Risk factors for accelerated atherosclerosis in renal transplant recipients. Am J Med. 1988;84:985–992
- Tzanatos HA, Tseke PP, Pipili C, et al. Cardiovascular risk factors in non-diabetic hemodialysis patients: A comparative study. Renal Failure. 2009;31:91–97
- Cheung AK, Sarnak MJ, Yan G, et al. Atherosclerotic cardiovascular disease risks in chronic hemodialysis patients. Kidney Int. 2000;58:353–362
- Tonelli M, Bohm C, Pandeya S, et al. Cardiac risk factors and use of cardioprotective medications in patients with chronic renal insufficiency. Am J Kidney Dis. 2001;37:484–489
- Le A, Wilson R, Douek K, et al. Prospective risk stratification in renal transplant candidates for cardiac death. Am J Kidney Dis. 1994;24:65–71
- Eknoyan G. On the epidemic of cardiovascular disease in patients with chronic renal disease and progressive renal failure: A first step to improve the outcomes. Am J Kidney Dis. 1998;32(Suppl. 3):51–54
- Manske CL, Thomas W, Wang Y, et al. Screening diabetic transplant candidates for coronary artery disease; identification of a low risk subgroup. Kidney Int. 1993;44:617–621
- Cachofeiro V, Goicochea M, de Vinuesa SG, et al. Oxidative stress and inflammation, a link between chronic kidney disease and cardiovascular disease. Kidney Int. 2008;111:S4–9
- Allon M. Evidence-based cardiology in hemodialysis patients. J Am Soc Nephrol. 2013;24:1934–1943