
Percutaneous nephrolithotomy (PNL) is regarded as the primary treatment option for large and complex kidney stones. However, in malrotated or pelvic ectopic kidneys, the injury risk of overlying bowel and abnormal vessels make this surgery a challenging procedure to urologists.Citation1,Citation2 Eshghi et al.Citation3 firstly described the laparoscopic-assisted PNL technique for ectopic kidneys. After this, several authors described their techniques, and in a recent study Rifaioglu et al.Citation1 presented a case of laparoscopic-assisted PNL via direct renal pelvis puncture in a pelvic kidney stone. We read this article with a great interest and herein we want to report our experiences in recently treated two cases with renal calculi; one had a pelvic kidney while the other had a malrotated kidney.
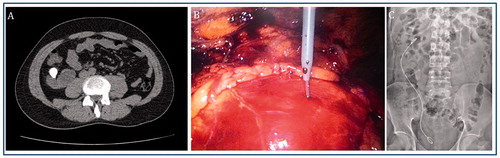
A 38-year-old man presented with right flank pain and hematuria. Non-contrast computerized tomography (CT) showed an approximately 30 mm calculus in the renal pelvis of malrotated right kidney (). We thought that transperitoneal laparoscopic-assisted PNL would provide an efficient and safe access for PNL. Firstly, a ureteral catheter was inserted cystoscopically on dorsal lithotomy position. The patient was then placed in the 60° flank position and 3-port laparoscopic approach was used. Gerota fascia was opened and renal pelvis carefully dissected. Renal access and tract dilation was performed directly into the renal pelvis under laparoscopic and fluoroscopic control (). Stone removal was accomplished using ultrasound lithotripsy through a 22 F rigid nephroscope. After complete stone clearance, renal pelvis was not repaired, but a double-J stent was inserted and 14 F drain was placed in the peritoneal cavity (). Drain catheter was removed on the second postoperative day and the patient was discharged from hospital 48 h after the procedure.
Figure 1. Approximately 30 mm calculus in the renal pelvis of malrotated right kidney (A); renal access was performed directly into the renal pelvis under laparoscopic and fluoroscopic control (B); complete stone clearence achieved and a double-J stent was inserted (C) 301 × 94mm (96 × 96 DPI).
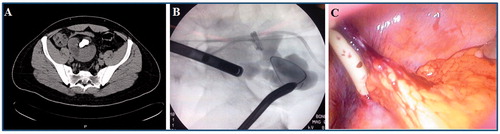
The second patient, aged 25-year-old man, presented with hematuria and abdominal pain. CT imaging showed atrophic left kidney and partial staghorn renal calculi in right pelvic ectopic kidney (). Patient was scheduled for laparoscopic-assisted PNL. Firstly, he was placed in the dorsal lithotomy position and open-ended ureteral catheter was inserted. The patient was then placed in the Trendelenburg position and through an umbilical incision a 10 mm port inserted into the peritoneal cavity. Two additional 5-mm cannulas were placed. The ectopic right kidney was identified and lower surface of kidney was exposed. Under laparoscopic vision and fluoroscopic control, percutaneous access to the lower calix was obtained (). Rest of the procedure was performed as in standard PNL. At the end of the procedure, a double-J stent and nephrostomy tube were inserted and 14 F drain was placed in the peritoneal cavity (). There was minimal drainage and drain catheter was removed on first postoperative day. Nephrostomy tube was removed on postoperative day 3 after antegrade nephrostography revealed. Patient was discharged on the third postoperative day.
Figure 2. Partial staghorn renal calculi in right pelvic ectopic kidney (A); under laparoscopic vision and fluoroscopic control, percutaneous access to the lower calix was obtained (B); a nephrostomy tube was inserted (C). 266 × 70mm (96 × 96 DPI).
In conclusion, laparoscopy-assisted PNL is safe, effective and has excellent results in the management of stones in pelvic ectopic kidneys and renal access can be performed directly into the renal pelvis or calyx.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
- Rifaioglu MM, Yalcinkaya FR, Bayarogullari H, et al. Direct pelvic access percutaneous nephrolithotomy in management of ectopic kidney stone: A case report and literature review. Ren Fail. 2013;35:1440–1444
- Binbay M, Istanbulluoglu O, Sofikerim M, et al. Effect of simple malrotation on percutaneous nephrolithotomy: A matched pair multicenter analysis. J Urol. 2011;185:1737–1741
- Eshghi AM, Roth JS, Smith AD. Percutaneous transperitoneal approach to a pelvic kidney for endourological removal of staghorn calculus. J Urol. 1985;134:525–527