
ABSTRACT
Purpose: To describe a case of Rosai-Dorfman-associated sclerouveitis in an HIV-infected patient.
Design: Case report.
Methods: A 49-year-old man with HIV had bilateral eye pain, redness, photophobia, and multiple systemic complaints. He underwent serial ocular examinations, abdomen/pelvis CT scan, and lymph node biopsy.
Results: Ophthalmologic evaluation revealed bilateral, nongranulomatous anterior uveitis and anterior scleritis. Biopsy of a retroperitoneal lymph node identified on CT revealed mixed inflammatory infiltrate composed of histiocytes, lymphocytes, and plasma cells involving fibroadipose tissue, indicating Rosai-Dorfman disease.
Conclusions: This is the first report of sclerouveitis in Rosai-Dorfman disease. Rosai-Dorfman is typically self-limiting, occurring rarely in HIV.
A 49-year-old African-American HIV-infected male (CD4 361 cells/mm3, HIV RNA 25 copies/mL) on combination antiretroviral therapy came to the inpatient HIV service with a 33-pound weight loss, night sweats, abdominal pain, and headache with bilateral eye pain, redness, and photophobia. He had no previous ophthalmic history. On ophthalmologic evaluation, visual acuity measured 20/40 in the right eye and 20/35 in the left eye, with pinhole improvement to 20/20 and 20/25, respectively. Intraocular pressures were 12 in both eyes, and no afferent papillary defect was present. Slit-lamp examination demonstrated bilateral, anterior uveitis with 2+ cells in the anterior chambers of both eyes, diffuse endothelial pigment, and a few scattered foci of posterior synechiae. Additionally, he had 3+ diffuse anterior scleritis, which was tender to palpation and did not blanch with topical phenylephrine 10%. There were no vitreous cells, and fundus examination was completely normal, with no evidence of posterior scleritis. Anterior chamber paracentesis was performed, and viral PCR was negative for HSV, VZV, and CMV. He was started on hourly topical prednisolone. Oral steroids were not initially started, due to concern about an infectious etiology.
CT scans revealed a hazy soft tissue thickening surrounding the proximal superior mesenteric artery, a 3.6 × 4-cm retroperitoneal mass with ill-defined borders, and axillary adenopathy, all suspicious for lymphoma. RPR, FTA-ABS, HLA-B27, p-ANCA, c-ANCA, and QuantiFERON-TB Gold were negative. CRP was 13.4 mg/dL. Angiotensin converting enzyme was normal. Fine-needle aspiration of the retroperitoneal mass was nondiagnostic, and excisional axillary lymph node biopsy revealed benign fibroconnective tissue.
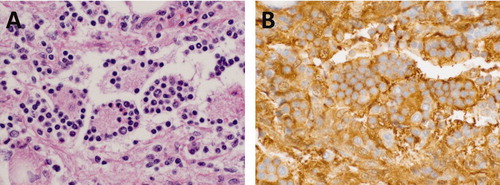
Ultimately, excisional biopsy of the retroperitoneal mass revealed a mixed inflammatory infiltrate composed of histiocytes, lymphocytes, and plasma cells involving fibroadipose tissue. Some histiocytes showed emperipolesis, consistent with sinus histiocytosis with massive lymphadenopathy (Rosai-Dorfman disease) ().
FIGURE 1. (A) Emperipolesis in Rosai-Dorfman disease: Large irregularly shaped histiocytes with abundant cytoplasm engulf intact cells, predominantly lymphocytes (H&E; 400×). (B) Cells that demonstrate emperipolesis are positive for S100 (S100; 400×).
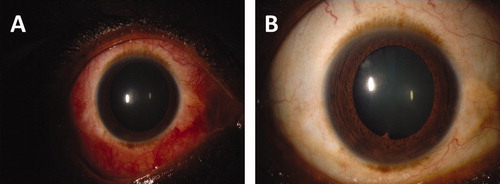
At the time of the excisional biopsy, 1 month after initial presentation, he had persistent, bilateral anterior scleritis and minimal anterior chamber inflammation. Following the biopsy, so as not to decrease the diagnostic yield, high-dose prednisone (100 mg daily; ∼0.6 mg/kg/day) was added, resulting in rapid improvement (). Three months later, he had tapered the oral prednisone to 5 mg daily with prednisolone drops twice daily and had no evidence of active scleritis or uveitis. Follow-up CT scan 6 months after original presentation revealed no persistent adenopathy.
FIGURE 2. (A) Ocular findings at presentation. (B) Ocular findings at 3-month follow-up.
ROSAI-DORFMAN DISEASE
Rosai-Dorfman disease was first described in the late 1960s and is characterized by a nonmalignant proliferation of histiocytes. The typical presentation is massive, bilateral, painless cervical adenopathy, and extranodal disease is common.Citation1
Ocular involvement in Rosai-Dorfman disease has been reported in up to 11.5% of patients a large series.Citation2 The most common ophthalmic manifestation is orbital soft tissue and eyelid infiltration, with similar cell populations and occasionally similar histopathologic architecture to that seen in the lymph nodes.Citation2–4 The globe is involved much less frequently in Rosai Dorfman disease. Uveitis has been reported in a few cases, including 2 cases of anterior uveitis in childrenCitation5,Citation6 and 3 cases with posterior segment involvement.Citation2,Citation7,Citation8 Several cases of epibulbar masses, with and without concomitant uveitis, have been reported.Citation7–9 These cases may mimic scleritis, but no cases of true scleritis associated with this disease appear in the literature. We believe our patient's presentation to be unique, in that he had no evidence of a discrete epibulbar mass, and instead presented with a more diffuse, bilateral anterior scleritis and associated nongranulomatous anterior chamber inflammation.
The treatment for ophthalmic manifestations of Rosai-Dorfman disease varies depending on the site of eye involvement. Surgical resection may be necessary if a discrete mass is present,Citation2 and patients with uveal involvement have been treated with varying combinations of topical and oral corticosteroids, as well as systemic immunosuppressive therapy.Citation7,Citation8
Four previous cases of Rosai-Dorfman disease in HIV-infected patients have been reported. In these cases, CD4 count at initial presentation ranged from 204 to 350 cells/mm3,Citation10,Citation11 a range similar to that of our patient. It is not known if chronic HIV infection contributes to an environment that stimulates macrophage activation. In summary, Rosai-Dorfman disease is benign and typically self-limiting, and has been rarely described in association with HIV. This is the first report of sclerouveitis in Rosai-Dorfman disease, and the patient responded to oral and topical corticosteroids.
DECLARATION OF INTEREST
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Related Research Data
REFERENCES
- Foucar E, Rosai J, Dorfman R. Sinus histiocytosis with massive lymphadenopathy (Rosai-Dorfman disease): review of the entity. Semin Diagn Pathol. 1990;7:19–73
- Foucar E, Rosai J, Dorfman R. The ophthalmologic manifestations of sinus histiocytosis with massive lymphadenopathy. Am J Ophthalmol. 1979;87:354–367
- Sanchez R, Sibley RK, Rosai J, Dorfman RF. The electron microscopic features of sinus histiocytosis with massive lymphadenopathy: a study of 11 cases. Ultrastruct Pathol. 1981;2:101–119
- Friendly DS, Font RL, Rao NA. Orbital involvement in sinus' histiocytosis: a report of four cases. Arch Ophthalmol. 1977;95:2006–2011
- Pivetti-Pezzi P, Torce C, Colabelli-Gisoldi RA, et al. Relapsing bilateral uveitis and papilledema in sinus histiocytosis with massive lymphadenopathy (Rosai-Dorfman disease). Eur J Ophthalmol. 1995;5:59–62
- Berger L, Galt J, Allansmith MR. Globe involvement in sinus histiocytosis. Am J Ophthalmol. 1983;95:124–125
- Payne JF, Srivastava SK, Wells JR, Grossniklaus HE. Rosai-Dorfman disease simulating nodular scleritis and panuveitis. Arch Ophthalmol. 2011;129:518–520
- Sarwal R, Tu E, Mendelblatt FI, et al. Atypical ocular presentations of Rosai-Dorfman disease. Ocul Immunol Inflamm. 2008;16:9–15
- de Oliveira RC, Rigueiro M, Vieira AC, et al. Rosai-Dorfman disease manifesting as an epibulbar ocular tumour. Clin Exp Ophthalmol. 2011;39:175–177
- Perry B, Gregg C, Myers S, et al. Rosai-Dorfman disease (extranodal sinus histiocytosis) in a patient with HIV. Ear NoseThroat J. 1998;77:855–858
- Delacretaz F, Meuge-Moraw C, Anwar D, et al. Sinus histiocytosis with massive lym Rosai Dorfman disease) in an HIV-positive patient. Virchows Arch A Pathol Anat Histopathol. 1991;419:251–254