Sir:
Juvenile xanthogranuloma (JXG) is a benign dermatologic condition affecting primarily infants and young children. It is a histiocytic proliferative disorder of non-Langerhans cells that usually appears as nodular cutaneous lesions and rarely affects the eye.Citation1 Some cases of limbal JXG have been describedCitation2 but to the best of our knowledge, this is the first report of JXG presented as an isolated conjunctival mass in a preschool child.
Case report
A 2-year-old Caucasian male infant was evaluated for a conjunctival lesion of 3-month duration. There was no history of trauma or foreign body entry. The patient's medical history was unremarkable.
Slit-lamp examination showed a raised, yellowish, rounded, 4-mm bulbar conjunctival mass without extension onto the cornea. The remainder of the ocular examination (cycloplegic refraction, iris inspection, and fundus appearance) was normal. There were no skin lesions and the systemic pediatric workup was noncontributory. After 3 weeks of medical treatment (fluorometholone drops) there was no regression. An excisional biopsy was then performed. A subconjunctival mass firmly attached to the sclera was dissected. ().
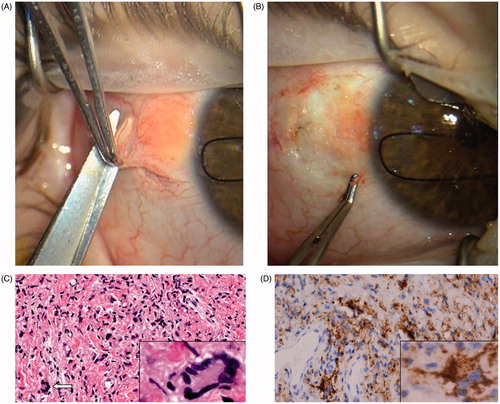
Figure 1. (A) Surgical excision of a subconjunctival yellow-orange lesion at the bulbar conjunctiva. (B) The subconjunctival mass has been dissected. The infiltration of the sclera was seen during the operation. (C) Microscopically, the specimen showed confluent histiocytes that were not particularly filled with lipid, scattered Touton giant cells (arrow and inset), and lymphocytes (hematoxylin–eosin, original magnification, ×100; inset, original magnification, ×400). (D) Diffuse CD68 positivity (macrophage marker) of the lesion (original magnification, ×100; inset magnification, ×400).
Histopathological examination showed a nodule of histiocytes with few lipidization, multinucleated Touton giant cells, and inflammatory cells (). No cytologic atypia, mitotic figures, or necrosis areas were observed. Immunohistochemical examination showed that cells were positive for α-1 antitrypsin and CD68 markers () and negative for S-100 protein. The morphology and the immunochemistry were consistent with the diagnosis of JXG, and specifically with the nonlipidized JXG form (NJXG).Citation3 Postoperatively, topical fluorometholone drops were again instituted. At the 20-month follow-up, there was no recurrence of the lesion.
Comment
JXG presented as a solitary infiltrative conjunctival mass is a very rare form recently described in an adult.Citation4 We are now presenting the first case of isolated JXG of the conjunctiva in a child. The differential diagnosis must be done with the spectrum of Langerhans cell histiocytosis that includes eosinophilic granuloma, and with some lymphoproliferative disorders. The histiocytes of JXG typically stain with the macrophage markers CD68 and α-1 antitrypsin, but are negative for the Langerhans cell markers S-100 and CD1a,Citation5 even in this atypical histopathologic variant of JXG, more common in infants.
In conclusion, JXG should be considered in the differential diagnosis of a solely bulbar conjunctival mass in the pediatric population. Histological and immunohistochemical examinations increase the diagnostic accuracy and are decisive in the final diagnosis.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
- Mocan MC, Bozkurt B, Orhan D, et al. Juvenile xanthogranuloma of the corneal limbus: report of two cases and review of the literature. Cornea. 2008;27:739–742
- Chaudhry IA, Al-Jishi Z, Shamsi FA, et al. Juvenile xanthogranuloma of the corneoscleral limbus: case report and review of the literature. Surv Ophthalmol. 2004;49:608–614
- Newman CC, Raimer SS, Sánchez RL. Nonlipidized Juvenile xantogranuloma: a histologic and immunohistochemical study. Pediatr Dermatol. 1997;14:98–102
- Lee ML, Wee WR, Lee, Jh, et al. Juvenile xanthogranuloma presenting as infiltrative conjunctival mass in an adult. Cornea. 2012;31:447–449
- Eagle RC. Immunohistochemistry in diagnostic ophthalmic pathology: a review. Clin Exp Ophthalmol. 2008;36:675–688