
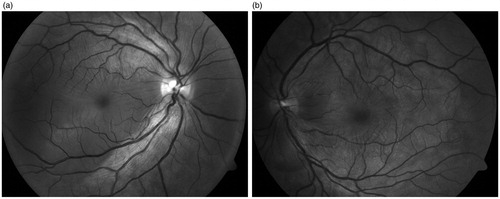
We report a case with a diagnostic dilemma due to an unusual clinical sign seen in a patient of Vogt-Koyanagi-Harada (VKH) disease. A young woman aged 36 years presented with sudden onset of painless visual loss of 5 days duration. She did not have any past history of corticosteroid use through systemic, topical, or other routes. On examination, her visual acuity was 20/80 in OD (right eye) and 20/40 in OS (left eye). Anterior segment examination showed the presence of occasional cells in both eyes. The fundus examination in both eyes showed mild hyperemia of the optic nerve heads and the red free fundus photo showed multiple subretinal fluid pockets along with retinal folds at the posterior pole in both eyes ().
FIGURE 1. Red-free fundus photo shows clear delineation of multiple subretinal fluid pockets and retinal folds in the posterior pole in both eyes.
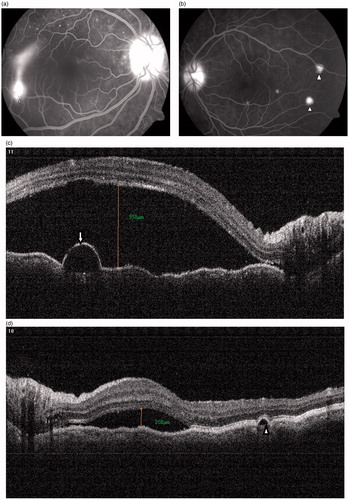
Fluorescein angiographic (FA) in OD showed a typical smokestack leak, with neurosensory retinal detachment. Two areas of retinal pigment epithelial detachment were seen in OS. Both eyes showed otherwise typical FA features, such as disc staining and multiple pinpoint leaks at the posterior pole, suggestive of Vogt-Koyanagi-Harada disease (VKH) ().Citation1 The OCT (optical coherence tomography) scan showed serous detachment of the macula in both eyes along with a small pigment epithelial detachment (PED) in the right eye corresponding to the area of smokestack leak seen on FA and also showed typical folds of RPE (retinal pigment epithelium)/Bruch’s membrane seen in VKH in both eyes ().Citation4
FIGURE 2. (a) Typical smokestack leak (arrow) with optic disc staining and multiple pinpoint leaks were seen at the posterior pole in the right eye. (b) Two small PED leaks (arrowheads) with disc staining and multiple pinpoint leaks are seen at the posterior pole in the left eye. (c) OCT scan in the right eye shows serous detachment of macula (measuring 958 μm), folds of RPE, and a small pigment epithelial detachment (arrow) corresponding to the smokestack leak seen on FA. (d) OCT scan in the left eye shows serous detachment of macula (measuring 208 μm), a small PED (arrowhead), and folds of RPE.
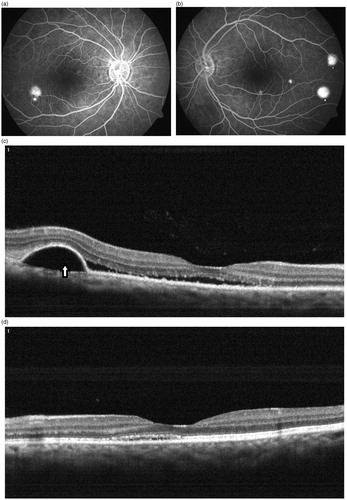
She was started on oral steroid therapy (tablet prednisolone 60 mg (1 g/kg) and an immunosuppressant (tablet azathioprine 50 mg twice a day). The oral steroid was tapered by 10 mg per week and immunosuppressant was continues as a steroid-sparing agent. After a month of therapy, she showed substantial clinical resolution of angiographic leakage and neurosensory detachment and subretinal fluid on OCT (). Visual acuity improved to 20/20, N6 in both eyes at 1 month follow-up. She was continued on immunosuppressants for 12 weeks. At the most recent follow-up visit, 1 year after the initial episode, she was maintaining VA of 20/20, N6 in both eyes. She did not have any recurrence of VKH and is not on any medication now.
FIGURE 3. (a, b) Substantial angiographic resolution of smokestack leak (arrow) in right eye with persistence of PED leaks (arrowheads) in both eyes. (c, d) OCT scan of the right eye shows partial resolution of serous detachment of macula with persistence of PED (arrow) seen temporally and substantial resolution of serous detachment of macula seen in the left eye.
The case describes the finding of an unusual smokestack pattern on FA and PED leaks suggestive of central serous chorio-retinopathy (CSCR)Citation2 occurring without past history of corticosteroid usage in a case of VKH at the initial presentation. To the best of our knowledge, this unusual association has not been reported earlier. However, association of CSCR with corticosteroid usage in uveitic entities such as VKH, Behçet uveitis, and birdshot chorio-retinopathy have been reported earlier.Citation4 A smokestack leak is a relatively rare angiographic finding seen in about 10% of cases of CSCR. A smokestack type of leak may not be seen frequently in VKH as the density of subretinal fluid is more due to a high protein content in contrast to CSCR. Bilateral, multiple pinpoint lesions on FA can be seen in multifocal CSCR. However, inflammatory cells in the anterior chamber (AC), hyperemia of optic nerve head, with disc staining on FA are unusual findings seen in CSCR. Predominant male gender predilection is seen in CSCR as compared to VKH. Indocyanine green angiography (ICGA) would have helped in differentiating between VKH disease and CSCR in our patient. The ICG shows multiple areas of choroidal vascular hyperpermeability in the mid-to-late phases of ICGA, which are indicative of CSCR,Citation5 whereas diffuse choroidal vascular hyperpermeability, hypofluorescent dark dots, and optic disc staining are typical features of VKH disease.Citation6
The treatment for CSCR and that of VKH is completely different, with steroids, being the mainstay of therapy in VKH but being contraindicated in CSCR.Citation1 We treated our case with systemic steroids and immunosuppressants. In our patient, the addition of an immunosuppressant (as a steroid-sparing agent) also helped to rapidly taper systemic steroids. This management was based on the overall clinical picture favoring the diagnosis of VKH. The case highlights the importance of basing a clinical diagnosis and management on the overall clinical picture rather than on a single clinical sign.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
- Bordaberry MF. Vogt-Koyanagi-Harada disease: diagnosis and treatments update. Curr Opin Ophthalmol 2010;21:430–435
- Ross A, Ross AH, Mohamed Q. Review and update of central serous chorioretinopathy. Curr Opin Ophthalmol. 2011;22:166–173
- Yamaguchi Y, Otani T, Kishi S. Tomographic features of serous retinal detachment with multilobular dye pooling in acute Vogt-Koyanagi-Harada disease. Am J Ophthalmol. 2007;144:260–265
- Khairallah M, Kahloun R, Tugal-Tutkun I. Central serous chorioretinopathy, corticosteroids, and uveitis. Ocul Immunol Inflamm. 2012;20:76–85
- Menchini U, Virgili G, Lanzetta P, et al. Indocyanine green angiography in central serous chorioretinopathy: ICG angiography in CSC. Int Ophthalmol. 1997;21:57–69
- Herbort CP, Mantovani A, Bouchenaki N. Indocyanine green angiography in Vogt-Koyanagi-Harada disease: angiographic signs and utility in patient follow-up. Int Ophthalmol. 2007;27:173–182