
Abstract
Purpose: To report the first documented case of HLA-A29+ birdshot chorioretinopathy in a Hispanic patient.
Case description: A 62-year-old female from Mexico presented with a 15-year history of progressive nyctalopia, floaters, and decreasing vision. She carried multiple previous diagnoses, including posterior vitreous detachment and macular edema. Both fundi showed characteristic creamy ill-defined lesions of birdshot chorioretinopathy, mostly atrophic, with evidence of old periphlebitis and arteriolar attenuation. Bilateral macular atrophy resulted in compromised visual acuity. Workup revealed positive HLA-A29 and was negative for TB and syphilis.
Conclusion: Despite having been reported almost exclusively in non-Hispanic Caucasians, HLA-A29-positive birdshot chorioretinopathy may occur in Hispanic patients. This patient's ethnicity may have resulted in a significant delay in diagnosis.
Birdshot chorioretinopathy (BSCR) is a poorly understood disease affecting 6–7.9% of patients with posterior uveitis,Citation1,Citation2 with a slight female predilection.Citation3,Citation4 To date, there is no clear explanation as to the pathophysiology leading to the characteristic ill-defined deep circular or ovoid cream-colored fundus lesions, classically described around the optic disc, radiating toward the midperiphery.Citation5 The disease is also associated with retinal vasculitis and cystoid macular edema. The strongest association with BSCR is the presence of HLA-A29 allele.Citation6
Report of a Case
We describe a 62-year-old woman from Mexico with a 15-year history of floaters, decreasing vision, and progressive nyctalopia. She had been seen by multiple ophthalmologists in both Mexico and the United States, and had received multiple diagnoses, including posterior vitreous detachment and unspecified uveitis. Five years ago, while hospitalized for a cerebrovascular accident, the patient was diagnosed with hypertension and non-insulin-dependent diabetes mellitus. She suffered severe visual loss at the same time and was found to have bilateral macular edema. No further investigation was performed and only topical treatment was instituted.
On presentation to our service, the patient's complaints were severe visual compromise, nyctalopia, and photopsias. Ocular history included retinal macroaneurysm in her left eye. She was on oral agents for treatment of diabetes, hypertension, and hypercholesterolemia. She was not on any medications for her ophthalmic condition.
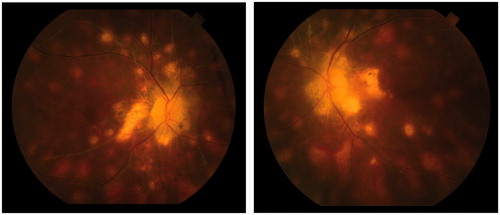
Best corrected visual acuity was 20/40 in both eyes, with reduced confrontation visual fields. Slit-lamp examination was normal, with the exception of 2+ anterior vitreous cell OU. Fundus examination revealed diffuse optic disc pallor and a rim of peripapillary atrophy in both eyes. Retinal vessels showed diffuse old sheathing of the veins in both eyes, with marked arteriolar attenuation. Multiple cream-colored ovoid deep lesions were seen around the discs in both eyes, extending nasally, superiorly and inferiorly (see ). Some punched out lesions were seen in the posterior pole and periphery in both eyes.
Figure 1. Both fundi showing classic end stage birdshot picture; profound optic atrophy surrounded by large patches of atrophic retina, multiple deep oval lesions extending to the midperiphery and involving the macula. There is profound arteriolar attenuation and mild inactive-appearing venous sheathing. There are also multiple punched out lesions.
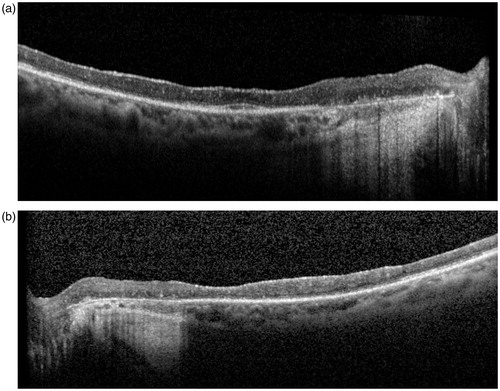
The maculae showed dull reflexes associated with marked atrophy of the outer retina as confirmed by OCT (see ).
Figure 2. (a) Macular OCT OD. Loss of architecture of the inner retinal layers and diffuse atrophy of the outer layers. Residual photoreceptor layer can be seen in the foveal region. Nasal to the fovea, the RPE is atrophic (corresponding to atrophy seen in the colored fundus photograph). The choroid is visualized and appears atrophic. (b) Macular OCT OS. Shows a similar picture as OD with an irregular subfoveal photoreceptor layer. Nasal to the fovea, the RPE is atrophic.
PPD and FTA-ABS were negative. HLA-A29 testing was positive. The patient was lost to follow-up, and therefore visual field, ERG, fluorescein, and ICG angiography results are not available. Workup did not include investigations for sarcoidosis as the fundus findings, including arteriolar attenuation, and characteristic deep, ill-defined ovoid lesions were typical of BSCR. However, sarcoidosis is always in the differential of retinitis and choroiditis, and is a more common diagnosis in this population.
Discussion
Birdshot chorioretinopathy has been described almost exclusively in non-Hispanic Caucasian patients. In a review by Shah et al.,Citation3 only 2 patients out of 337 reported in literature were not Caucasian of European descent. To our knowledge, this is only the second Hispanic patient with BSCR reported in literatureCitation4 and the first supported by positive HLA-A29. The diagnosis of birdshot chorioretinopathy is based on the characteristic clinical picture. A positive HLA-A29 is a supportive finding,Citation5 occurring in at least 95% of BSCR patients.Citation7 HLA typing is the most sensitive and specific test for BSCR, with a very high estimated relative risk of developing the disease in HLA-A29 carriers.Citation6,Citation8
The exact role of the HLA molecule in birdshot chorioretinopathy is not completely understood. The disease's response to immunosuppressive therapy strongly suggests an autoimmune process with a genetic predisposition, having been reported in twinsCitation9 and families.Citation10 The primary site of the inflammatory process is believed to be the choroid.Citation3 The role of class I HLA (including HLA-A) is to present antigens to T cells, an immune process related to the expression of the HLA-A29 molecules within antigen-presenting cells believed to contribute to the pathology of BSCR.Citation11 Using PCR, the major histocompatibility complex alleles HLA-A*2901 and HLA-A*2902 are found to be the most commonly occurring HLA-A29 subtypes in birdshot chorioretinopathy patients.Citation12 Structurally, both molecules differ by a single amino acid that is not related to their antigen presenting function, leading to equal roles in initiating an immune response.Citation12 The frequencies of the alleles in U.S. Hispanic population are 0.35 and 4.17%, respectively.Citation13 Their frequencies in U.S. non-Hispanic Caucasian population are 0.7 and 3.3%. Thus, differences in frequency of these alleles in the two populations cannot explain the overrepresentation of non-Hispanic Caucasians in the population of patients with BSCR. The reason for the disparity in disease prevalence in different groups is unclear, and may be elucidated with further research into genetic or other factor associated with development of disease.
We present this patient to highlight the fact that birdshot chorioretinopathy may occur in Hispanic patients, as we believe that this patient's ethnicity resulted in a significant delay in diagnosis, with resultant permanent loss of visual function. While HLA typing may not be necessary in the setting of a Caucasian patient with typical clinical findings, it is a good confirmatory test in less classic situations.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
- Rodriguez A, Calonge M, Pedroza-Seres M, et al. Referral patterns of uveitis in a tertiary eye care center. Arch Ophthalmol. 1996;114:593–599
- Smit RL, Baarsma GS, de Vries J. Classification of 750 consecutive uveitis patients in the Rotterdam Eye Hospital. Int Ophthalmol. 1993;17:71–76
- Shah KH, Levinson RD, Yu F, et al. Birdshot chorioretinopathy. Surv Ophthalmol. 2005;50:519–541
- Gasch AT, Smith JA, Whitcup SM. Birdshot retinochoroidopathy. Br J Ophthalmol. 1999;83:241–249
- Levinson RD, Brezin A, Rothova A, et al. Research criteria for the diagnosis of birdshot chorioretinopathy: results of an international consensus conference. Am J Ophthalmol. 2006;141:185–187
- Brézin AP, Monnet D, Cohen JH, Levinson RD. HLA-A29 and birdshot chorioretinopathy. Ocul Immunol Inflamm. 2011;19:397–400
- Priem HA, Kijlstra A, Noens L, et al. HLA typing in birdshot chorioretinopathy. Am J Ophthalmol. 1988;105:182–185
- Papadia M, Herbort CP. Reappraisal of birdshot retinochoroiditis (BRC): a global approach. Graefes Arch Clin Exp Ophthalmol. 2013;251:861–869
- Fich M, Rosenberg T. Birdshot retinochoroidopathy in monozygotic twins. Acta Ophthalmol (Copenh). 1992;70:693–697
- Trinh L, Bodaghi B, Fardeau C, et al. Clinical features, treatment methods, and evolution of birdshot chorioretinopathy in 5 different families. Am J Ophthalmol. 2009;147:1042–1047
- Szpak Y, Vieville JC, Tabary T, et al. Spontaneous retinopathy in HLA-A29 transgenic mice. Proc Natl Acad Sci USA. 2001;98:2572–2576
- Levinson RD, Rajalingam R, Park MS, et al. Human leukocyte antigen A29 subtypes associated with birdshot retinochoroidopathy. Am J Ophthalmol. 2004;138:631–634
- www.allelefrequencies.net [online]