
ABSTRACT
Purpose: To determine the prevalence of trachoma in all suspected endemic districts in Malawi.
Methods: A population-based survey conducted in 16 evaluation units from 12 suspected endemic districts in Malawi (population 6,390,517), using the standardized Global Trachoma Mapping Project (GTMP) protocol. A 2-stage cluster-random sampling design selected 30 households from each of 30 clusters per evaluation unit; all residents aged 1 year and older in selected households were examined for evidence of follicular trachoma (TF), intense trachomatous inflammation (TI), and trachomatous trichiasis (TT).
Results: Four of the 16 evaluation units were found to be endemic for trachoma, with a prevalence range of 10.0–13.5% for TF and 0.2–0.6% for TT. Nine evaluation units had a TF prevalence between 5.0% and 9.9% while three evaluation units had a TF prevalence <5.0%.
Conclusion: The prevalence rates of active trachoma in Malawi were not uniform among suspected endemic evaluation units, with rates higher than the World Health Organization (WHO) threshold for implementation of community-based control measures (TF ≥ 10.0%) in only 4 of the 16 evaluation units. Trachoma remains a disease of public health importance in some parts of Malawi and adjoining (unmapped) districts should be prioritized for mapping. According to the survey, an additional 3,169,362 people require intervention to reduce active disease and 1557 trichiasis surgeries are needed to reduce the prevalence of TT below WHO recommended thresholds.
INTRODUCTION
As a result of an unprecedented recent increase in international interest, blinding trachoma may be facing its end.Citation1 Trachoma, an infectious eye disease, is caused by serotypes A, B, Ba and C of the bacterium Chlamydia trachomatis.Citation2,Citation3 The immune response which is central to the development of scarring pathology provides only partial protection against re-infection, which can be frequent. Repeated infections can eventually lead to thickening and scarring of the upper tarsus which can result in the eyelashes turning inwards and rubbing on the cornea,Citation4 causing abrasions and ulceration. Trachoma remains the leading infectious cause of blindness in Sub-Saharan Africa, especially in populations that have poor environmental sanitation, inadequate water supply and poor socioeconomic status.Citation5,Citation6 More than 80% of the burden of active trachoma is now concentrated in only 14 countries, all of them located in Africa.Citation1,Citation5,Citation7 In endemic areas, trichiasis (inward turning of lashes that abrade the cornea) is about 1.8 times more prevalent in women than men.Citation8,Citation9
Worldwide, considerable progress has been made in trachoma elimination; over the last decade, the estimated number of individuals with trichiasis has been revised downwards from 8.2 million,Citation5,Citation10 to 4.6 million.Citation1 However, many trachoma suspected areas lack district-level prevalence dataCitation11,Citation12 necessary for deciding whether or not full implementation of community-based interventions is required. As of July 2013, Malawi was no exception, with only 5 of the 17 suspected trachoma-endemic districts having been mapped.Citation13,Citation14 With support from the Global Trachoma Mapping Project (GTMP) we sought to map the remaining 12 suspected endemic districts in the country.
MATERIALS AND METHODS
Approval was obtained from the National Health Sciences Research Committee (NHSRC), and separate approval was obtained from the district health administrative offices (DHO) in Malawi. Approval for the GTMP internationally was obtained from the ethics committee of the London School of Hygiene & Tropical Medicine (reference 6319). After explanation of the purpose of the study, written informed consent was obtained from all subjects who participated in the study. Where the participant was a minor, informed consent was obtained from the head of household or guardian.
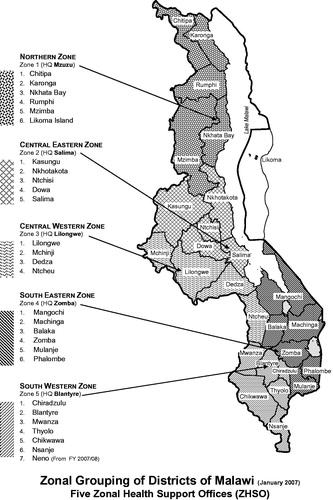
Malawi has five health zones, which have a total of 28 districts (). There were 12 selected study districts in total, encompassing a total population of 6,390,517, situated in all health zones except the Northern Zone, which was not suspected to have endemic trachoma. Mangochi, the district with the largest population, was subdivided into three sub-districts, while the two other large population districts (Zomba and Lilongwe) were each subdivided into two sub-districts resulting in the construction of 16 evaluation units in total, according to World Health Organization (WHO) recommended size for an evaluation unit (100,000–250,000 persons).
FIGURE 1. Map of Malawi Health Zones.
The study was a cross-sectional population-based survey designed to obtain district-level prevalence estimates for follicular trachoma (TF) in children aged 1–9 years, and trachomatous trichiasis (TT) in persons aged 15 years and over. The study was conducted between May and September 2013. The GTMP standardized training package and methodologies were used.Citation15 The Malawian team leader (KK) underwent training and certification as a Master Grader in Ethiopia in February 2013 conducted by the GTMP Chief Scientist (AWS), and this was followed by a training-of-trainers course on how to train others, organized in Blantyre in March 2013 and conducted by SL.
Sample Size
As described elsewhere,Citation15 the GTMP sample size for each evaluation unit of approximately 100,000–250,000 persons (designed to have 80% power of estimating 10% TF prevalence with an absolute precision of 3% and design effect of 4) was 1019 children aged 1–9 years, inflated by a factor of 1.2 to allow for non-response. To achieve this sample size in the Malawian context, 30 clusters of 30 households each were proposed to be sampled from each evaluation unit.
Selection of Clusters and Households for Survey
Clusters were defined as villages, which in rural Malawi have a mean population of 1000–2000 residents. In each evaluation unit, a sampling frame of all villages was obtained from the district health office, and 30 were selected using probability proportional to size. In each cluster, all households were listed and 30 were selected using computer-generated random numbers. All residents of selected households aged 1 year and older were invited to participate.
Training
Training included several stages; training of survey graders and training of survey recorders was performed separately, followed by testing and certification of grader and recorder trainers, and finally combined training of survey graders and recorders on the survey protocol.
Training of grader trainers took 3 days. The format of the GTMP manual provided the basis for the training so that trainers learned how to use the manual. For certification in grading, a standardized slide test was administered in the morning of the first day and after all trainees demonstrated proficiency on this, they went to the field for an inter-grader agreement practice test, with KK's grades serving as the gold standard. A total of 50 eyes of 50 children were examined and a minimum kappa score of 0.8 for the diagnosis of TF was required for certification as a grader trainer. The final day was spent on training and discussion with the recorder trainers, initially starting with revisions of the hard copies of the questionnaire, followed by practice on an Android smartphone.
Training of survey graders and recorders took 4 days and each group was trained separately for 2 days (graders focusing on eye examinations to grade trachoma, while recorders focused on capturing data on the Android smartphone), and this was followed by 2 more days where teams were trained together. Graders were taught how to safely and reliably examine children and adults for evidence of TF, intense trachomatous inflammation (TI) and TT, and recognize and refer other priority diseases. Both training sessions had theoretical classroom lessons, followed by classroom practice and then field practice. At the end of field practice both groups took exams and only those who passed were allowed to continue. Recorders were required to pass an online examination while graders took a grading test and were required to score a minimum kappa of 0.7 for the diagnosis of TF in an inter-grader agreement test with 50 eyes of 50 children. Graders and recorders who passed the test were trained together for 2 more days on the study methodology and roles for each person, through classroom and field practice.
Two grader/recorder training sessions were conducted in Malawi, the first for the six Southern Region districts (9 evaluation units), where 13 Ophthalmic Clinical Officers (OCOs) and 13 recorders (final year medical students) were trained (July 2013), and the second for the six Central Region districts (7 evaluation units) where 12 OCOs and 12 recorders (fresh non-medical university graduates) were trained (August 2013). All 25 OCOs were from the Ministry of Health. After training, teams were formed comprising one grader and one recorder, with the grader examining while the recorder captured data on the Android smartphone. In total, 10 teams were used for the Southern and Central Region districts. On average each team was expected to map one cluster per day (according to the GTMP training manual), hence with 10 teams, each evaluation unit of 30 clusters could be mapped within 3 days.
Field Methods
Each selected cluster was visited a few days in advance of the survey date/day by a community health worker (Health Surveillance Assistant) from the Ministry of Health; this cadre is normally responsible for disease surveillance and health promotion. Their role here was to brief the village chief and the community members and organize the selected village household list to be used for random household selection by the survey team. On arrival in the villages, the survey team made a random selection of households. Then, after obtaining consent from the household head, global positioning system (GPS) and water, sanitation and hygiene (WASH) data were collected, and household members were enumerated and examined for signs of trachoma, using a 2.5 × magnifying loupe (Binomag plastic, Kansas City, MO, USA). Individuals found to have active trachoma were treated with 1% tetracycline eye ointment and adults with TT were referred to the district hospital.
Quality Control
The 10 teams were supervised by two supervisors, with each supervisor spending 1 day each per every 5 days with each team. The supervisors were experienced OCOs who had been assessed and qualified as grader trainers and were part of the training team. In addition, at the completion of field work for each evaluation unit, investigators, supervisors and recorders met to discuss logistical challenges faced and suggest solutions and improvements.
Data Management, Analysis and Reporting
Field data collection was performed using Android devices running the LINKS application system (Task Force Links/Task Force for Global Health, Decatur, GA, USA). Upon completion of field work each day, the recorder uploaded survey data from the Android smartphone over an encrypted connection to the GTMP secure server running in the Amazon Elastic Compute Cloud (EC2, Amazon Web Services). Subsequent processing and approval was undertaken as described elsewhere.Citation15
RESULTS
A total of 480 clusters from 16 evaluation units were visited, and 14,296 households out of 14,400 planned were enumerated (99% coverage). In total 48,395 people were examined, out of the 50,084 enumerated, representing a coverage of 96.6% ().
TABLE 1. Demographic characteristics of participants examined in baseline trachoma surveys, Southern Malawi, 2013.
The data showed that the districts of Lilongwe (east and west), Kasungu and Nkhotakota (together representing four evaluation units) were above the WHO threshold of 10% TF in children aged 1–9 years, whereby implementation of the full SAFE strategy (surgery, antibiotics, facial cleanliness and environmental improvements), including mass drug administration of azithromycin, is recommended, while 10 evaluation units had a measurable TT prevalence above the WHO “elimination” goal of < 1/1000 in 10 out of 16 evaluation units, indicating the need for TT surgery in these locations (). Three evaluation units (Zomba 1, Balaka and Phalombe) warranted no specific trachoma intervention for active trachoma (prevalence of TF in children 1–9 years was < 5%). Nine evaluation units had TF prevalence rates between 5.0 and 9.9% in children aged 1–9 years, indicating the need for sub-district level estimates of TF prevalence.
TABLE 2. Prevalence of trachomatous inflammation–follicular (TF) and trachomatous trichiasis (TT) in surveyed districts, Southern and Central Malawi, 2013.
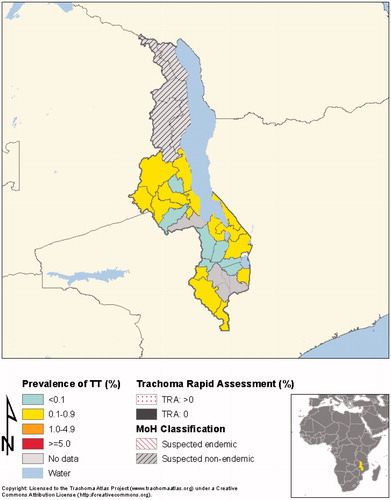
shows the prevalence of TF in Malawi, according to the most recent survey data, including those reported in the current manuscript, while shows the prevalence of TT in Malawi according to the most recent survey data, including those reported in the current manuscript.
FIGURE 2. Prevalence of follicular trachoma (TF) in Malawi, according to the most recent survey data, including those reported in the current manuscript. TRA, trachoma rapid assessment; MoH, Ministry of Health.
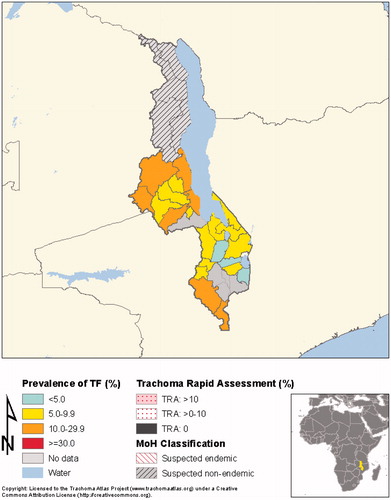
FIGURE 3. Prevalence of trachomatous trichiasis (TT) in Malawi, according to the most recent survey data, including those reported in the current manuscript. TRA, trachoma rapid assessment; MoH, Ministry of Health.
DISCUSSION
The GTMP set out to generate prevalence data on TF, TT and WASH variables in all trachoma-suspected districts in Malawi, to guide national policy and decision-making in regard to implementation of the SAFE strategy.
The results show that all nine suspected endemic evaluation units in Southern Malawi had active trachoma below the prevalence level at which the full SAFE strategy is recommended while four of seven suspected endemic evaluation units in Central Malawi had active trachoma above this level. The prevalence of TF and TT in the confirmed endemic districts was very similar to figures obtained from recent mapping in other endemic districts.Citation13
The low TF prevalence obtained in the Southern Region districts was somewhat unexpected since this area has been thought to be trachoma endemic for a long time. District and tertiary hospitals in these areas consistently report the presence of cases of un-operated TT, consistent with the TT prevalence we found. This fits a general pattern in which TF disappears but prevalent cases of TT remain, requiring TT interventions. It is also possible that there are specific pockets with high TF and TT within sub-districts in this region, and that by framing relatively large populations of more than 300,000 people as evaluation units, these hot spots were not identified in the evaluation unit-level analyses.
The presence of a majority of evaluation units with TF prevalence between 5.0 and 9.9% highlights an important problem requiring consideration. According to current guidelines, evaluation units with TF prevalence <5.0% do not need a full 3-year SAFE strategy implementation cycle, while evaluation units with TF prevalence ≥10.0% do require implementation of the full SAFE strategy for at least a 3-year period. For evaluation units with TF prevalence 5.0–9.9%, the WHO recommendation is to estimate prevalence at “sub-district” levelCitation16 to look for “hot spots” that require treatment. The cost of undertaking formal sub-district surveys and the level down to which they should be undertaken has not been studied. As more surveys are done, it is likely that there will be many evaluation units in this situation. It is a matter of some urgency that clear, practical, tested guidelines are provided.
Another issue highlighted in these surveys is the question of what to do about unmapped areas which are not suspected to have TF but which border evaluation units with TF high enough to warrant treatment. Districts from Northern Malawi were not selected as suspected endemic districts but in fact, three Northern Region districts are bordered by two of the four confirmed endemic districts in the Central Region; an additional two districts in Northern Malawi are bordered by areas in Tanzania and Zambia confirmed to have endemic trachoma. It seems reasonable to suspect that these bordering previously “unsuspected” districts might now become “suspected endemic” and require mapping. Guidelines are urgently needed not only for when to label a district as “suspect” and requiring mapping, but also for when not to map. With the data being collected by the GTMP there are possibilities for identifying water and sanitation indicators that might help us answer these questions.
In summary, the GTMP has provided information on evidence that trachoma is of public health importance in four evaluation units in Central Malawi; according to WHO guidelines, these are eligible for full implementation of the SAFE strategy. However, the survey has also raised practical questions about further mapping in areas bordering high-TF evaluation units and about how best to deal with evaluation units with TF prevalence of 5.0–9.9%. These questions require urgent attention from the international trachoma community if we are to eliminate this disease as a public health problem.
ACKNOWLEDGMENTS
We would like to acknowledge the contributions by the following individuals and organizations during the survey period: Ministry of Health for providing staff, District Health Management teams for all the recorders and graders, the Health Surveillance Assistants and the community volunteers that took part in the survey.
The Global Trachoma Mapping Project Investigators are:
Methodologies Working Group: Simon J. Brooker, Paul Emerson, Katherine Gass, Danny Haddad, Jonathan D. King, Chad MacArthur, Els Mathieu, Beatriz Muñoz, Erik Harvey, Jeremiah Ngondi (lead), Stephanie Ogden, and Anthony W. Solomon.
Prioritisation Working Group: Simon Bush, Paul Courtright, Paul M. Emerson, Allen Foster (lead), Danny Haddad, Richard Le Mesurier, Silvio P. Mariotti, and Anthony W. Solomon.
Tools Working Group: Erik Harvey, Jonathan D. King, Thomas M. Lietman, Alexandre L. Pavluck, Joseph Pearce, Anthony W. Solomon (lead), and Sheila K. West.
Training Working Group: Agatha Aboe, Paul Courtright (lead), Jonathan D. King, Susan Lewallen, Chad MacArthur, Silvio P. Mariotti, Els Mathieu, Jeremiah Ngondi, Anthony W. Solomon, Jennifer L. Smith, and Sheila K. West.
ITI Technical Team: Brian Chu, Rebecca M. Flueckiger, Alexandre L. Pavluck, and Rebecca Willis.
DECLARATION OF INTEREST
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Financial support was received from the United Kingdom's Department for International Development, through its Global Trachoma Mapping Project grant to Sightsavers.
REFERENCES
- Haddad D. Trachoma: the beginning of the end? Community Eye Health 2012;25:18
- Bailey R. rRNA-based tests for chlamydial infection in trachoma. Br J Ophthalmol 2007;91:271
- Mabey DC, Forsey T, Treharne JD. Serotypes of Chlamydia trachomatis in The Gambia. Lancet 1987;2:452
- Mabey DC, Solomon AW, Foster A. Trachoma. Lancet 2003;362:223–229
- Mariotti SP, Pascolini D, Rose-Nussbaumer J. Trachoma: global magnitude of a preventable cause of blindness. Br J Ophthalmol 2009;93:563–568
- Burton MJ. Trachoma: an overview. Br Med Bull 2007;84:99–116
- Hu VH, Harding-Esch EM, Burton MJ, et al. Epidemiology and control of trachoma: systematic review. Trop Med Int Health 2010;15:673–691
- Mpyet C, Lass BD, Yahaya HB, et al. Prevalence of and risk factors for trachoma in Kano state, Nigeria. PLoS One 2012;7:e40421
- Cromwell EA, Courtright P, King JD, et al. The excess burden of trachomatous trichiasis in women: a systematic review and meta-analysis. Trans R Soc Trop Med Hyg 2009;103:985–992
- Resnikoff S, Pascolini D, Etya'ale D, et al. Global data on visual impairment in the year 2002. Bull World Health Organ 2004;82:844–851
- Polack S, Brooker S, Kuper H, et al. Mapping the global distribution of trachoma. Bull World Health Organ 2005;83:913–919
- Smith JL, Haddad D, Polack S, et al. Mapping the global distribution of trachoma: why an updated atlas is needed. PLoS Negl Trop Dis 2011;5:e973
- Kalua K, Chirwa T, Kalilani L, et al. Prevalence and risk factors for trachoma in central and southern Malawi. PLoS One 2010;5:e9067
- Tielsch JM, West KP Jr, Katz J, et al. The epidemiology of trachoma in southern Malawi. Am J Trop Med Hyg 1988;38:393–399
- Solomon AW, Pavluck A, Courtright P, et al. The Global Trachoma Mapping Project: methodology of a 34-country population-based study. Ophthalmic Epidemiol 2015;22:214–225
- Solomon A, Zondervan M, Kuper H, et al. Trachoma control: a guide for programme managers. Geneva, Switzerland: World Health Organization, 2006
- Malawi Housing and Population 2008 census. Zomba, Malawi: National Statistical office. Available from: www.nsomalawi.mw [last accessed Nov 2013]