
To the editor,
With reference to the publication by Neslihan Andic et al. regarding risk of thrombosis in a case of idiopathic thrombocytopenic purpura, we share herein a similar experience in our medical institute.
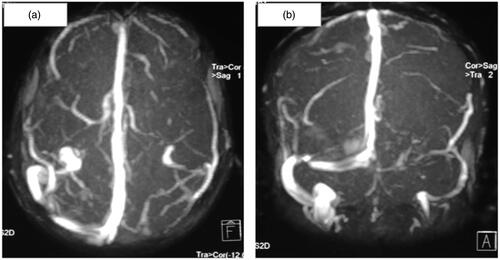
A 16-year-old boy with history of epistaxis and petechial spots over body for last 2 years was evaluated and found to have low platelet counts of 10 × 103/µl. Bone marrow examination suggested megakaryocytic thrombocytopenia. Other benign causes were ruled out and final diagnosis of idiopathic thrombocytopenic purpura was made. He was started on prednisolone 1 mg/kg once a day to which he responded over period of next 4–6 weeks and platelet counts rose up to maximum value of 75000/µL. However, as steroid doses were tapered down, his platelet counts started worsening. Hence he required alternative drugs – danazol and azathioprine, to which he again responded dramatically and his average platelet counts varied between 75 and 100 × 103/µl. Unfortunately, he did not turned up for next 6 months and finally presented to emergency services with the complaints of focal, involuntary movement of right upper limb. Initial clinical possibility of intracranial bleed was kept in view of past history of thrombocytopenic disorder. However, radiological investigations including magnetic resonance and venography showed venous thrombosis of left transverse and sigmoid sinus (). His platelet count was 90 × 103/µl. Therapeutic anticoagulation with injectable low-molecular weight heparin followed by oral warfarin was started. Later on, he was continued with azathioprine for his basic disease with threshold of platelet count being maintained ∼50–75 × 103/µl.
Figure 1. MRI venography of intracerebral vessels showing thrombosis of left transverse and sigmoid sinus in transverse (a) and coronal planes (b).
Above experience with index case is very similar to that of author's case in that both patients required varied range on immunosuppresant's for thrombocytopenia. Both cases developed venous thrombosis during course of treatment. However, the platelet count of our patient was 90000/µL that is much lower as compared to author's case which underlines the importance of factors other than increased platelet count as a cause of thrombosis. One such cause is continuous circulation of comparatively younger cells having more thrombotic potential which author has also highlighted.
The other major point that is worth mentioning here is regarding recent study by Kim et al. [Citation1] who studied vWF antigen levels in 21 patients of ITP and did thromboelastography to investigate the effect of vWF antigen levels in the haemostasis and coagulation profile of ITP patients. They found that those patients who have elevated vWF levels have comparatively higher thrombotic tendencies. Also, cases with elevated vWF levels were comparatively older and had disease of long duration.
Study by Neslihan Andich et al. [Citation2] and Kim et al. [Citation1] have very well pointed out that there should be different cut-off or threshold levels of platelet count depending on following factors: (1) duration of disease, (2) drugs being used with concern to their thrombotic potentials, (3) vWF antigen levels, (4) previous history of thrombosis, (5) associated co-morbidities like chronic liver disease or thrombophilia and (6) hypercoagulable states like pregnancy or use of pro-thrombotic drugs like contraceptive pills.
In conclusion, our case as well as author's case very well justifies the need of regular follow-up for better titration of doses of drugs. And, also each individual of ITP should be scrutinized for possible thrombotic predispositions and hence individualization of target level of platelet counts is of utmost importance.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the article.
References
- Kim WH, Park JB, Jung CW, Kim GS. Rebalanced hemostasis in patients with idiopathic thrombocytopenic purpura. Platelets 2014
- Andic N, Gunduz E, Akay OM, Sahin D, Teke HU. Cardiac and pulmonary thrombosis during multidrug treatment in an idiopathic thrombocytopenic purpura patient. Platelets 2014;25:69–70