Sirs,
Surgery, including Mohs' technique, is regarded the reference modality for the treatment of most basal cell carcinomas (BCCs) (Citation1). Yet surgical treatment in challenging cases (large, multiple, confluent or recurrent BCCs) can be an arduous undertaking with relatively high relapse rates, particularly when conventional surgery is employed. ‘Immunocryosurgery’ has been recently introduced as a non-surgical, tissue-sparing combination of cryosurgery during ongoing topical imiquimod for the treatment of ‘non-superficial’ BCCs (Citation2).
Herein, on the occasion of two cases, we would like to highlight the efficacy of immunocryosurgery as a treatment alternative for patients with challenging BCCs: (i) multiple/concurrent facial tumors that require extensive surgery and (ii) BCC relapses that would have mandated major reconstructive head-and-neck surgery.
Patient 1: A 71-year-old farmer presented with multiple (n = 18) facial BCCs (, ). Pathology confirmed diagnosis in two excised (eyelid BCCs) and six biopsied tumors. His medical history included prostate cancer, coronary heart disease and hyperlipidemia on goserelin acetate, clopidogrel and simvastatin, respectively. Excessive sun exposure was his only risk factor for multiple BCC. Nevoid BCC syndrome was excluded based on history, physical examination and assessment of relevant radiological signs. Daily 5% imiquimod cream (Aldara; Meda) was applied every evening on the nasal and left parietal lesions. After 2 weeks, no inflammation was evident and 0.1% tazarotene gel (Zorac; Pierre Fabre) was added every morning. Two weeks later (), a mild, open spray liquid N2 cryosurgery was applied to the inflamed BCCs (two freeze–thaw cycles (FTCs); 15-second freezing time each) and tazarotene and imiquimod were continued for an additional 4 weeks after cryosurgery. In this way, 16 tumors were treated in groups of three to five tumors and within 4 months the patient was disease-free. During the 24-month follow-up, one tumor recurred (, arrow). Conclusively, in this patient, 15/16 tumors were effectively treated with one cycle of immunocryosurgery.
Figure 1. Immunocryosurgery for the treatment of two representative patients with therapeutically challenging BCC disease: treatment course and outcomes. Panels A–D: treatment of a patient with a multitude of concurrent, almost confluent head-and-neck BCCs (Patient 1). (A) Detail of the patient's mid-face showing multiple BCCs covering most of his nose surface. Insert: illustration of the patient's head and neck region indicating the localizations of the concurrent 18 BCCs at presentation. (B) Mid-face of the patient showing multiple, almost confluent BCCs on the nose and concurrent BCCs on the cheeks. (C) The same region as in Panel B on the day of cryosurgery showing heavily inflamed tumors after treatment with daily 5% imiquimod cream for 4 weeks (during the 2 last weeks in combination with 0.1% tazarotene gel) just before the cryosurgery session. (D) The same region as in Panel B 24 months after treatment. The outcome of treatment was excellent, with minimal scarring and sustained remissions in 15/16 tumors treated by immunocryosurgery (one tumor relapsed during the 2-year follow-up: Panel D, arrow). Two BCCs – the tumor at the left lower eyelid (Panel B) and a tumor on the right lower eyelid – were surgically removed prior to the immunocryosurgery. Panels E and F: patient 2. (E) Neglected BCC relapse of the right ear 5 years after excision of the primary tumor at presentation. (F) Clinical outcome 18 months after treatment with a single cycle of immunocryosurgery.
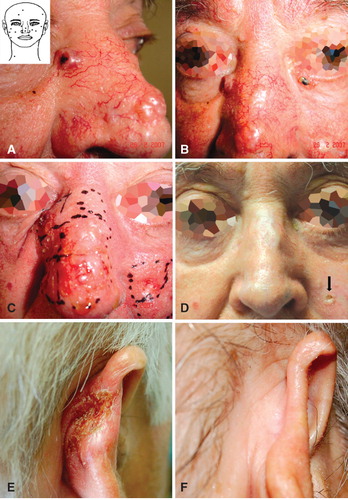
Patient 2: A 63-year-old male was referred for a neglected, 28 × 17-mm, biopsy-proven recurrent BCC on his right ear 5 years after surgical removal of the primary (). His medical history included type II diabetes on glimepiride, arterial hypertension and coronary heart disease on olmesartan and metoprolol. After 3 weeks on daily imiquimod, liquid N2 cryosurgery was performed (open spray, two FTCs, 15-second freezing time each) followed by 3 additional weeks of imiquimod. The tumor cleared and has remained relapse-free for 18 months ().
The efficacy of imiquimod monotherapy on incompletely excised, recurrent or large tumors in patients unsuitable for surgery has been reasonably questioned (Citation3) as have the rationale and effectiveness of ‘aggressive’ freezing times of several minutes (Citation4), which are required to control such challenging BCCs. Yet topical imiquimod and cryosurgery combine additively in the framework of immunocryosurgery, as underlined by the substantially shorter freezing times employed in this approach (Citation2,Citation5). Notably, in selected cases where imiquimod alone elicits an inadequate inflammatory response (patient 1), this can be overcome by the addition of tazarotene.
In conclusion, immunocryosurgery is a promising, pathophysiologically designed, minimally invasive, office-based therapeutic modality that can be applied as an alternative approach in the treatment of otherwise relatively ‘difficult-to-treat’ BCCs.
Acknowledgement
This study was partially supported by Special Research Account Program, University of Ioannina No 22195.
Declaration of interest: GG, KN and IDB declare that they have received travel grants from Meda Hellas. CV reports no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
- Thissen M, Neumann M, Schouten L. A systematic review of treatment modalities for primary basal cell carcinomas. Arch Dermatol. 1999;135(10):1177–1183.
- Gaitanis G, Nomikos K, Vava E, Alexopoulos EC, Bassukas ID. Immunocryosurgery for basal cell carcinoma: Results of a pilot, prospective, open-label study of cryosurgery during continued imiquimod application. J Eur Acad Dermatol Venereol. 2009;23(12):1427–1431.
- Murphy ME, Brodland DG, Zitelli JA. Definitive surgical treatment of 24 skin cancers not cured by prior imiquimod therapy: A case series. Dermatol Surg. 2008;34(9):1258–1263.
- Kokoszka A, Scheinfeld N. Evidence-based review of the use of cryosurgery in treatment of basal cell carcinoma. Dermatol Surg. 2003;29(6):566–571.
- Bassukas ID, Gaitanis G. Combination of cryosurgery and topical imiquimod: Does timing matter for successful immunocryosurgery? Cryobiology. 2009;59(1):116–117.