Abstract
Socio-demographics and workplace stress may affect men and women differently. The aim of this cross-sectional study was to assess sex-specific interactions among age, occupational status, and workplace Demand-Control-Support (D-C-S) factors in relation to psychiatric symptoms and allostatic load levels representing multi-systemic “wear and tear”. It was hypothesized that beyond main effects, D-C-S factors would be moderated by occupational status and age in sex-specific directions predictive of subjective psychiatric symptoms and objective physiological dysregulations. Participants included healthy male (n = 81) and female (n = 118) Montreal workers aged 20 to 64 years (Men: M = 39.4 years, SD = 11.3; Women: M = 42.8 years, SD = 11.38). The Job Content Questionnaire was administered to assess workplace D-C-S factors that included psychological demands, decisional latitude, and social support. Occupational status was coded using the Nam--Powers--Boyd system derived from the Canadian census. Psychiatric symptoms were assessed using the Beck Anxiety Scale and the Beck Depression Inventory II. Sex-specific allostatic load indices were calculated based on fifteen biomarkers. Regression analyses revealed that higher social support was associated with less depressive symptoms in middle aged (p = 0.033) and older men (p = 0.027). Higher occupational status was associated with higher allostatic load levels for men (p = 0.035), while the reverse occurred for women (p = 0.048). Women with lower occupational status but with higher decision latitude had lower allostatic load levels, as did middle-aged (p = 0.031) and older women (p = 0.003) with higher psychological demands. In summary, age and occupational status moderated workplace stress in sex-specific ways that have occupational health implications.
Introduction
Approximately 15% to 20% of Europeans and North Americans report chronic workplace stress (ILO, Citation2000) that costs society 1 to 3.5% of the national gross domestic product (Hoel et al., Citation2001). In Canada, one-third of workers report chronic workplace stress (Dewa et al., Citation2007), costing about $51 billion annually in terms of absenteeism, lost productivity, indemnities, and healthcare bills (Lim et al., Citation2008; Marchand & Durand, Citation2011). Chronic workplace stress is therefore a major focus of occupational health theories, research, and practice.
Among the various workplace stress perspectives, one of the most popular is the Demand-Control-Support (D-C-S) model (Karasek & Theorell, Citation1990; Kristensen, Citation1996) stating that high-strain workplaces are characterized by: (a) increased psychological demands representing the quantitative and qualitative responsibilities of one’s work; (b) decreased decision latitude representing limited authority, control, and ability to develop skills in the workplace; and (c), decreased social support garnered from colleagues and superiors. Collectively, high-strain workplaces are linked to psychiatric conditions, cardiovascular disease, and metabolic problems (Theorell, Citation2000). However, reports using the British Whitehall II cohort (Marmot et al., Citation1991) reveal that increased workplace decision latitude and social support are protective against psychiatry-related absenteeism (Stansfeld et al., Citation1997, Citation1999), highlighting the need to further investigate both harmful and beneficial D-C-S profiles. Concordantly, the current study assessed whether D-C-S factors would be associated with psychiatric symptoms and physiological dysregulation while accounting for the sex-specific moderating effects of workers’ age and socio-economic status (SES).
In Canada and other industrial nations, differential exposures to workplace stressors are partially explained by an unequal sex distribution among occupations that generally render women of diverse ages and social strata (Maclean et al., Citation2004) more vulnerable to adverse D-C-S profiles and associated psychiatric symptoms (Marchand et al., Citation2005a,Citationb,Citationc; Vermeulen & Mustard, Citation2000). For example, women have a higher lifetime risk of developing depressive and anxiety disorders than do men (Seedat et al., Citation2009). In the context of workplace stress, psychiatric symptoms are influenced by a complex interplay among D-C-S- factors that differ between the sexes from diverse backgrounds (Fuhrer & Stansfeld, Citation2002; Lennon, Citation1987; Marmot et al., Citation1991).
As demonstrated by a meta-analysis of the workplace stress literature, these sex differences in health outcomes may be due to divergent roles and ranks held within occupational hierarchies (Stansfeld & Candy, Citation2006). Occupational status (OS) represents the prestige, education, and income associated with one’s occupational position (Adler & Newman, Citation2002; Fujishiro et al., Citation2010). Epidemiological studies consistently link higher OS to lower risk of morbidity and mortality (Adler et al., Citation2007; Marmot, Citation2004; McEwen & Gianaroe, Citation2010; McEwen & Tucker, Citation2011). Among the Whitehall II cohort, lower OS was associated with more absenteeism due to psychiatric illness (Stansfeld et al., Citation1994) as well as more psychological distress among those additionally afflicted by physical illnesses (Stansfeld et al., Citation2003). Among respondents of the Canadian National Population Health Survey, social gradients in exposures to high psychological demands and low decision latitude exist whereby younger workers with less education and women are most affected (Brisson et al., Citation2001). Unfortunately, smaller occupational health studies rarely examine OS in conjunction with D-C-S factors to further understand sex-specific trajectories in stress-related diseases.
The cumulative impact of chronic workplace stress throughout lifespan development contributes to both psychiatric symptoms and physiological dysregulations. This “wear and tear” on the brain and body is called allostatic load (AL), which is quantifiable by assessing alterations in multiple biological systems (McEwen & Stellar, Citation1993). Using a count-based AL index that ascribes sub-clinical thresholds to various neuroendocrine, immune, cardiovascular and metabolic biomarkers (Seeman et al., Citation1997), numerous studies have demonstrated consistent associations with mental and physical health outcomes (e.g. psychiatric symptoms, cardiovascular disease, mortality) in cross-sectional and prospective analyses. Reviews also highlight that AL is related to older age, lower SES, and adverse working conditions, but inconclusively vis-à-vis sex differences (Beckie, Citation2012; Juster et al., Citation2010, Citation2011a).
International research has linked workplace stress to increased AL. To summarize, elevated AL levels were first reported among older male German industrial workers reporting high psychological demands (Schnorpfeil et al., Citation2003). Among a cohort of Chinese industrial workers, elevated AL levels was associated with older age, male sex and low decision latitude in a first study (Li et al., Citation2007), in addition to lower education, low psychological demands and high hostility in a subsequent study (Sun et al., Citation2007). A prospective study recently demonstrated that Swedes exposed to social adversity at age 16 years and who later reported high psychological demands at age 43 years had increased AL levels (Westerlund et al., Citation2012). Collectively, these findings indicate that D-C-S factors influence AL levels.
Moreover, workplace AL studies highlight the important main effects that sex, age, and SES exert on AL; however, much less is known about moderation effects using these factors conjunctively. Elsewhere in epidemiological studies, SES has been linked to AL levels across the lifespan (Szanton et al., Citation2005). Despite these complementary studies on social disparities, interactions among workplace stress and SES factors are rather rare and mixed in the occupational health literature (Muhonen & Torkelson, Citation2003), especially as they pertain to psychiatric symptoms (Wege et al., Citation2008) and AL levels (Beckie, Citation2012; Juster et al., Citation2011a).
Understanding sex differences in psychiatric symptomatologies and physiological dysregulations necessitates analyses that assess the synergistic effects of SES and workplace stress at various life stages in order to provide information on how to eventually minimize risk and maximize protection. In accordance, the present study explored the sex-specific interaction effects of age, OS (Muhonen & Torkelson, Citation2003; Piltch et al., Citation1994), and D-C-S factors, namely, psychological demands, decision latitude, and social support, in relation to symptoms of depression, anxiety, and AL levels in a medium-sized cross-section of healthy Montreal workers from various occupations.
Two sets of general hypotheses were explored. Firstly, to replicate direct effects of D-C-S factors, we hypothesized that increased psychological demands, decreased decision latitude, and decreased social support would be associated with increased symptoms of depression and anxiety as well as increased AL levels beyond any potential effects of age and OS. Secondly, in the proposed assessment of interaction effects, we hypothesized that D-C-S factors would be moderated by OS and age in sex-specific directions predictive of subjective psychiatric symptoms and objective physiological dysregulations.
Methods
Participants
Participants were healthy male (n = 81) and female (n = 118) workers aged 20–64 years (Men: M = 39.4 years, SD = 11.3; Women: M = 42.8 years, SD = 11.38). As reported elsewhere (Gordon et al., Citation2012; Levesque et al., Citation2009, Citation2010), they were recruited through advertisements in newspapers and community centers within the greater Montreal area. The purpose of the larger study conducted between 2005 and 2007 was to evaluate the relation between cardiovascular risk and psychophysiological factors. The current study is a quasi-experimental, cross-sectional analysis aimed at understanding the interactions among age, OS and D-C-S factors in relation to psychiatric symptoms and AL levels.
This sample was selected according to strict eligibility criteria that included: (a) no utilization of mental health services within the past year; (b) no current/known health problems or use of medications capable of affecting cardiovascular, immune, or neuroendocrine functions; (c) no learning or cognitive disabilities sufficient to impair ability to complete questionnaires or understand instructions; and (d) no current hormone replacement therapy. Interested participants were screened by telephone for inclusionary criteria to safeguard against confounding effects. In particular, we wished to avoid labeling effects that contribute to stereotyping as well as inherent disease processes that could influence psychological and biological indices. Despite these precautions, 9% of female and 17% of male participants met criteria for the metabolic syndrome in final analyses, revealing that this is not a purely pre-clinical sample as some participants had undiagnosed conditions. It is important to highlight the fact that AL is a construct that is different from the metabolic syndrome (McCaffery et al., Citation2012).
To ensure a broad age distribution across the continuum of working adulthood, participants were selected to provide approximately three equally represented age groups: 18–34 years, 35–44 years and 45–65 years. For purposes of other research questions not addressed in the current analysis, women were over-sampled to include a sufficient number of post-menopausal women: menopausal status (n = 34) was based on the absence of menstrual cycle for 12 months or more prior to testing that was not due to any medical condition (e.g. hysterectomy, anorexia). lists all sample characteristics and variable descriptive statistics.
Table 1. Descriptive statistics.
General protocol
Eligible participants were scheduled for a laboratory appointment at the Montreal Heart Institute. To control for circadian rhythms in physiological activity, all laboratory visits began at 08:00 h on weekdays. Participants were requested to abstain from eating, drinking (other than water), smoking and strenuous exercise for 12 h prior to testing. They were also asked to refrain from alcohol or other drug use during the 24 h period preceding the appointment. Participants who did not adhere to these instructions or who presented any physical symptoms (e.g. cough, headache) on the day of the testing were sent home and a new appointment was scheduled (n = 3).
After written informed consent was obtained, electrodes for electrocardiogram monitoring were attached in a bipolar configuration to the lower side of the left and right rib cage. A ground electrode was placed on the left hip. The laboratory visit involved two venipunctures, one before and one after exposure to psychosocial stress tasks, with a total of 30 ml of blood drawn. Blood extraction was facilitated by inserting a butterfly needle into the median cubital vein in the non-dominant arm to minimize discomfort. Blood was divided among (i) three tubes on ice containing ethylenediaminetetraacetic acid (EDTA) as anticoagulant, to later provide six plasma aliquots; (ii) a tube without anti-coagulant, to later provide three serum aliquots; and (iii) one heparinized tube; after 30–60 min the tubes were centrifuged for 30 min at 3000 × g at 4 °C. Glucose, insulin, lipid profiles and high sensitivity C-reactive protein were assayed immediately while the remaining plasma and serum aliquots were frozen and stored at −80 °C until assaying.
During the laboratory session, participants were tested by a same-sex research assistant trained to maintain a neutral rapport throughout the session.
Participants also engaged in psychosocial stress paradigms reported elsewhere (Gordon et al., Citation2012; Levesque et al., Citation2010). The protocol included nine time-points after which saliva was collected (): (1) baseline session (10 min period); (2) blood draw 1; (3–6) immediately after exposure to stressors 1 to 4 (each involving a 5 min relaxation phase and a 2 min preparation phase prior to stressor and a 5 min recovery phase following it); (7) post-stress recovery; (8) blood draw 2; and (9) final recovery phase. For the stress protocol, each participant was exposed to four stress tasks lasting 5 min each (20 min total), while being videotaped during testing. Firstly, a neutral reading task involved reading aloud a text on Antarctica’s geography in front of a same-sex confederate. Second and thirdly, two role-plays involved alternating scenarios whereby participants adopted the role of personnel supervisor providing feedback about mediocre work performance to a worker (research confederate); feedback was expressed using either agreeable assertions or quarrelsome assertions in counterbalanced conditions. Fourthly, a non-scripted debate on abortion ensued whereby participants argued from a partisan position, alternating speaking (3 min total) and listening (2 min total) for 1 min periods with a confederate debating the opposite position. In total, the laboratory protocol lasted approximately 90 min depending on the time required for blood sampling. Salivary samples were assayed for cortisol that was computed into a single value used in the calculation of AL indices ().
Table 2. Individual biomarkers incorporated into allostatic load indices for men and women separately. Sex-specific means, standard error of the mean (S.E.), and cut-offs used in the summation of allostatic load index dichotomizations (“0” = normal & “1” = sub-clinical/clinical).
In addition, questionnaires were administered to obtain information on socio-demographics, medical and psychological measures. Waist circumference, height and weight were measured and blood was drawn, as above, in a fasting state following a 10 min rest period. In addition, ambulatory blood pressure and electrocardiography were obtained during the 24 h period following the laboratory session. Finally, for a period of 21 days, participants provided information on their behavioral and affective responses to interpersonal interactions (up to 10 times a day) on a handheld computer (data not reported here).
In total, participants were required to come to the laboratory three times: stress testing, to return ambulatory blood pressure and electrocardiography equipment, and finally to return the palm top computer. Upon study completion, each participant received $200 Canadian as compensation for his/her considerable time commitment and travel expenses. The Research and Ethics Board of the Montreal Heart Institute approved this study, which adhered to the Declaration of Helsinki.
Occupational status
OS was coded using the Nam--Powers--Boyd method (Nam, Citation2000; Nam & Boyd, Citation2004) applied to the 2001 National Occupational Classification for Statistics system (Boyd, Citation2008). This pure-type socio-economic scaling system was developed to delineate the inequalities that exist among peoples’ occupations stratified according to collective demographic and SES dimensions (Boyd, Citation2008). In this manner, OS scores were based on the median education and income in a given occupational category as in the Canadian census (Nam & Boyd, Citation2004). While this formulation does not include consensus information typifying prestige-based methods (Fujishiro et al., Citation2010), it does inherently embody a hierarchy based on occupational rank.
We used Appendix A from Boyd (Citation2008) to code OS from occupation information provided by participants. A former career placement counsellor reviewed the coding to confirm the occupational classification chosen. Boyd (Citation2008) ranks prestige of 520 occupations (1 = Specialist Physicians to 520 = Trappers & Hunters) and estimates education and income for each occupation. We focused analyses on the Boyd-NP scores ranging from 0 (lowest OS) to 100 (highest OS). Mean OS in the current sample was similar between the sexes ().
Questionnaires
Workplace stress
A French Canadian translation of the Job Content Questionnaire (Brisson et al., Citation1998; Karasek et al., Citation1998; Larocque et al., Citation1998) was used to measure workplace stress dimensions of the D-C-S model; namely, psychological demands, decision latitude, and social support. This scale has 29-items answered using a 4-point Likert scale to demarcate workplace stress characteristics. The French Canadian version has acceptable internal consistency for both full-scale and sub-scales with Cronbach’s α ranging from 0.68 to 0.85 among both white and blue collar workers (Brisson et al., Citation1998). In the current study, internal consistency reliability was similar with Cronbach’s α = 0.77 for the full-scale. We used the following sub-scales in the analyses of the D-M-S model: (1) psychological demands (9-items; Cronbach’s α = 0.77), (2) decision latitude consisting of skill utilization and work constraints (9-items; Cronbach’s α = 0.77), and finally (3) social support consisting of reports of colleagues’ and supervisor(s)’ support (11-items; Cronbach’s α = 0.71). Algorithms used to calculate D-C-S sub-scales applied additions or multiplications that ultimately expand the sub-scale ranges: validation among Quebec workers (Karasek et al., Citation1998) revealed that psychological demands range from 9 to 36 (M = 24), decision latitude ranges from 24 to 96 (M = 73), and social support ranges from 11 to 44 (M = 24).
Depressive symptoms
The 21-item Beck Depression Inventory II (BDI-II) (Beck, Citation1996) was administered to assess self-reported depressive symptoms. It has high test–retest reliability (r = 0.93) and internal consistency (Cronbach’s α = 0.91). Participants completed a validated French Canadian translation (Bourque & Beaudette, Citation1982) with acceptable test–retest reliability (r = 0.62) after 1 month and high internal consistency (Cronbach’s α = 0.92). Total sum scores were used in the present analysis; Cronbach’s α = 0.88 denoted strong internal consistency in the current sample. The standardized cut-offs are: 0 to 13 (minimal depression); 14 to 19 (mild depression); 20 to 28 (moderate depression); and 29 to 63 (severe depression); (Beck et al., Citation1988b).
Anxiety symptoms
The 21-item Beck Anxiety Inventory (Beck et al., Citation1996) was used to measure self-rated symptoms of anxiety. This instrument has acceptable test–retest reliability (r = 0.75) after 1 week, and high internal consistency (Cronbach’s α = 0.93; Beck et al., Citation1988a). Participants completed a validated French Canadian translation (Freeston et al., Citation1994) with similar test–retest reliability (r = 0.63) after 1 month, and internal consistency (Cronbach’s α = 0.85). Total sum scores were used in the present study; Cronbach’s α = 0.81 denoted acceptable internal consistency. The standardized cut-offs are: 0 to 7 (minimal anxiety); 8 to 15 (mild anxiety); 16 to 25 (moderate anxiety); and 26 to 63 (severe anxiety) (Beck & Steer, Citation1993).
Biomarkers
Fifteen biomarkers were incorporated into the calculation of sex-specific AL indices. Cortisol dynamics (area under the curve) represented neuroendocrine activities. Immune/inflammatory functioning was measured with tumor necrosis factor-α (ng/l), interleukin-6 (ng/l), and high sensitivity C-reactive protein (mg/L). Cardiovascular functioning was measured with systolic blood pressure (mmHg), diastolic blood pressure (mmHg), and heart rate variability (standard deviation of normal to normal R-R intervals, SDNN) obtained over a 24-hour period. Glucose regulation was assessed with insulin (pmol/l), glucose (mmol/l), and homeostatic model assessment of insulin resistance (HOMA). Lipid profiles included high-density lipoprotein cholesterol (mmol/l), low-density lipoprotein cholesterol (mmol/l), and triglycerides (mmol/l). Anthropometrics included body mass index (kg/m2) and waist-to-hip ratio.
Neuroendocrine
Salivary cortisol was obtained using Salivettes (Sarstedt, Montreal, Canada) containing a piece of absorbent gauze. Subjects chewed on the swab for 45 s until it was saturated with saliva. Samples were transferred to a −20 °C freezer and analyzed off-site using an enzyme immunoassay kit (Assay Designs, Inc., Ann Arbor, MI) in duplicates. Cortisol in saliva is a valid and reliable measure of the unbound hormone in the blood (Kirschbaum & Hellhammer, Citation1989). Nine samples of salivary cortisol were obtained during the laboratory session beginning immediately after each of the following periods: baseline (around 08:30 h), two blood samples (drawn after baseline and after the last stressor was administered), each of four stressors and at the end of two recovery periods (following the last psychological stressor and following the last blood draw).
Cortisol concentrations normally peak within the first hour upon awakening (cortisol awakening response) and decrease thereafter, reaching lowest levels before bedtime. In the current study, the mean waking time of participants was 06:15 h ± 41 min and study testing began around 08:00 h, approximately 90 min after awakening. Given the timing of cortisol measures, we chose to examine cortisol as the area under the curve with respect to ground using the trapezoid formula (Pruessner et al., Citation2003) to represent overall cortisol activity during the laboratory session starting at zero (basal cortisol concentration).
Immune/inflammatory
Following a fasting blood draw, serum samples were assayed at the Montreal Heart Institute for tumor necrosis factor-α and interleukin-6, respectively, measured using the R&D Systems Quantikine High Sensitivity TNF-α ELISA assay (Cat. No. HSTA00D, R&D Systems, Minneapolis, MN) and High Sensitivity IL-6 ELISA assay (Cat. No. HS600B, R&D Systems, Minneapolis, MN) according to manufacturer instructions. Determinations were made in duplicates using 200 and 100 µl serum, respectively. These assays utilize one monoclonal and one polyclonal antibody in a sandwich enzyme immunoassay technique. The lower standard of the calibration curve (0.5 ng/l for tumor necrosis factor-α and 0.156 ng/l for interleukin-6) was employed as the lowest reportable result. All results were higher than the lowest standard of the calibration curve (0.5 ng/l for tumor necrosis factor-alpha and 0.156 ng/l for interleukin-6), so sensitivity was not a concern. Inter-assay precision for these assays is between 10.6% and 6.5% at different levels.
High-sensitivity C-reactive protein (hsCRP) in serum was measured using the Siemens (formerly Dade Behring) CardioPhase high-sensitivity quantitative CRP assay (Siemens Healthcare Diagnostics Products GmbH, Marburg, Germany) on the BN ProSpec Nephelometer (Siemens Healthcare Diagnostics Products GmbH). The assay utilizes monoclonal anti-CRP antibodies coated to polystyrene particles and a human calibrator traceable to the WHO Reference Material. Inter-assay precision for this assay is below 6.0%. The minimal detectable hsCRP concentration is 0.18 mg/l.
Cardiovascular
Blood pressure measures were obtained every 20 min in the day time and every hour from 22:00 h to 06:00 h using Spacelab Ambulatory Blood Pressure Units that use an oscillometric method. The blood pressure measures were based on values averaged over 24 h. Ambulatory measures of blood pressure have been found to be more reliable predictors of disease endpoints compared to clinic- or laboratory-based measures (Sherwood et al., Citation2002).
Electrocardiogram measures were obtained using the 92510 3-lead Holter recorder by Burdick. Data were analyzed offline using the Vision Premier Monitoring system, allowing Time Domain and Spectral Analysis of heart rate variability (HRV). HRV was calculated offline from beat-to-beat RR intervals derived from the electrocardiography recordings. Analyses were performed once artefacts and premature beats were manually excluded by an experienced technician. A minimum of 22 h of analyzable ECG data were required for validity. Among the time domain parameters, SDNN is the simplest and most frequently reported, reflecting all the cyclic components responsible for HRV over a specific recording period.
Metabolic
Upon a fasting blood draw, plasma samples were analyzed for lipids, glucose and insulin at the Montreal Heart Institute. Lipid and glucose determinations were made using the respective reagent Flex on the multi-analyzer Dimension RxL Max (Siemens Healthcare Diagnostics, Newark, DE, formerly Dade Behring Diagnostics, Marburg, Germany) while insulin was measured by electrochemiluminescence immunoassay (Roche Diagnostics, Mannheim, Germany) on the Cobas e601 analyzer (Roche Diagnostics) with heparinized plasma, immediately after blood draw.
Participants’ weight and height and hip and waist circumference were measured to respectively calculate body mass index (BMI) and waist-to-hip ratio.
Allostatic load index
Individual biomarker values were categorized according to sex-based cut-offs (Seplaki et al., Citation2006) based on the sample’s distribution for biomarker levels (). AL indices were then constructed using the traditional count-based formulation (McEwen & Seeman, Citation1999; Seeman et al., Citation2001) calculated by summing the number of values falling at/or beyond the cut-off. Cut-offs were therefore sex-specific and set at the upper 75th percentile for most biomarkers. The lowest 25th percentile was used for high-density lipoprotein cholesterol and HRV whereby decreased levels denote higher health risks. Additionally, because hypo- and hyper-activity of the HPA-axis are deleterious (Fries et al., Citation2005; Juster et al., Citation2011b), both low (12.5th percentile) and high (87.5th percentile) cut-offs were used for cortisol in accordance with a validated alternative method (Seplaki et al., Citation2005). AL indices could theoretically range from 0 to 15.
Statistical analysis
Preliminary analyses
reports all descriptive statistics for men and women separately. Preliminary analyses centered upon sex differences among our independent and dependent variables revealed that the women were significantly older (p = 0.036) and showed a trend towards receiving more social support at work (p = 0.055) compared to men. Greater age in women was not surprising as we oversampled women for menopause.
The potential confounding influence of marital status (coded as “1” for single/divorced/separated/widowed (n = 108) and as “2” for married/common-law (n = 81)) and number of cohabitating children/adolescents as well as weekly smoking, caffeine (coffee and tea), alcohol, exercise, and working hours on our outcomes was scrutinized. None of these variables were correlated with psychiatric symptoms or AL indices at p < 0.20. We therefore did not incorporate these variables as covariates in our main analyses in order to preserve power.
Preliminary analyses examined the correlations among indicators of SES for each sex. For men, OS was significantly correlated with personal income (r = 0.439, p < 0.001), household income (r = 0.412, p < 0.001), but not education level. Likewise for women, OS was significantly correlated with personal income (r = 0.232, p < 0.01), household income (r = 0.278, p < 0.01) and education level (r = 0.224, p < 0.05). These inter-correlations validate that our OS measure overlaps with other SES indices, albeit correlations are weaker among women.
Consistent with a review (de Lange et al., Citation2003) showing only modest effects when assessing additive and interactive formulations of workplace stress factors (e.g. low-control × high demands × low support), preliminary analyses incorporating these formulations did not approach significance (all p > 0.25). We consequently did not explore these alternative formulations of the D-C-S model further.
Pearson’s correlations split by sex were used to assess associations among our outcome measures. While AL levels were not correlated to psychiatric symptoms for either sex (all p > 0.19), depressive symptoms were strongly and identically correlated to anxiety symptoms among men (r = 0.640, p < 0.001) and women (r = 0.640, p < 0.001). This justified assessing psychiatric and AL levels as separate outcomes.
Main analytic strategy
Because of sex differences in workplace conditions and outcome variables, we stratified analyses according to sex in accordance with previous studies (Marchand, Citation2007; Messing et al., Citation1998). Separate hierarchical regressions were therefore run for men and women. The independent variables were age, OS, workplace stress characteristics (all entered as continuous variables), and finally interaction terms to assess moderation effects. Despite similarities, it has been recommended to assess symptoms of depression and anxiety separately given subtle differences in associations to D-C-S factors (Plaisier et al., Citation2007). The dependent variables were therefore total sum scores for the Beck Depression Inventory II and Beck Anxiety Inventory as well as AL indices.
Independent variables were entered into the regression equations in separate blocks: (1) age (forced in), (2) OS (forced in), (3) Karasek sub-scales for psychological demands, decision latitude, and social support (forced in), and (4) two-way interaction terms involving age, OS, and workplace variables (stepwise). Age was entered first, because it has consistently been found to correlate with AL levels (Crimmins et al., Citation2003; Juster et al., Citation2010) and with symptoms of depression (Blazer & Hybels, Citation2005) and anxiety (Brenes, Citation2006). OS was entered second as it estimates a person’s professional position at a population-level and therefore functions as a precursor to the potential workplace stress characteristics that may be experienced at an individual-level. D-C-S factors were entered third as they represent self-reported workplace conditions. Lastly, two-way interaction terms were entered stepwise to explore potential moderation effects of age, OS and workplace stress. We report F-tests for each regression model in-text; predictor weights and R2 change magnitudes are reported in .
Table 3. Hierarchical regression statistics for the prediction of depressive symptoms split by sex.
Table 4. Hierarchical regression statistics for the prediction of anxiety symptoms split by sex.
Table 5. Hierarchical regression statistics for the prediction of allostatic load indices split by sex.
Significance was set at p < 0.05 for main effects and at p < 0.10 for interactions in order to minimize Type II error (Winer, Citation1962). Interactions were then evaluated using simple slope analyses as proposed by Aiken & West (Citation1991). In all the analyses, multi-collinearity among predictors was deemed insignificant with variance inflator factors (VIFs) ranging from 1.018 to 1.336.
Results
Depressive symptoms
Men
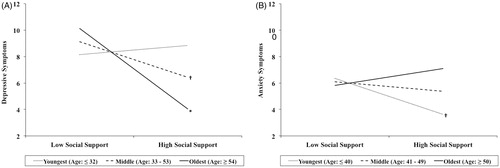
For depressive symptoms among men, age and OS entered respectively were non-significant. Workplace stress factors rendered the regression equation significant (FModel(5,75) =3.299, p = 0.010), whereby increased psychological demands and decreased decision latitude were associated with increased depressive symptoms (). Social support at work was found to be significant in interaction with age (FModel(6,74) = 3.751, p = 0.003). Simple slope analyses revealed that older men with higher social support experienced significantly lower depressive symptoms (β = −0.447, p = 0.004). A similar trend was also found among middle-aged men (β = −0.198, p = 0.063), but not young men ().
Figure 1. Estimated depression scores for men (n = 81) and anxiety scores for women (n = 118) based on two interaction effects decomposed using simple slope regression analyses. First, (A) depression scores were significantly lower among older men (p = 0.027) and as a trend among middle-aged men (p = 0.063) reporting higher social support. Second, (B) anxiety scores showed a trend towards lower levels among younger women with higher social support (p = 0.077). *p < 0.05; †p < 0.10.
Women
In women, age and OS were not significantly associated with depressive symptoms. Entering workplace stress factors was statistically significant (FModel(5,112) = 4.377, p = 0.001). Specifically, increased psychological demands and decreased social support predicted increased depressive symptoms. No significant interactions were found ().
Anxiety symptoms
Men
For anxiety symptoms among men, age and OS were not significant. With workplace stress factors entered (FModel(5,75) = 2.525, p = 0.036), increased psychological demands were associated with increased anxiety symptoms. No interaction effects were detected ().
Women
For anxiety symptoms among women, age and OS were not significant. When workplace stress factors were entered (FModel(5,112) = 3.0, p = 0.014), increased psychological demands and decreased decision latitude were associated with increased anxiety symptoms (). An interaction effect between age and social support was found (FModel(6,111) = 3.141, p = 0.007). Inspection of the simple slopes revealed that younger women with more social support at work revealed a non-significant trend to experience fewer anxiety symptoms (β = −0.20, p = 0.077; ).
Allostatic load
Due to incomplete collection of biomarkers, 14 of the 199 participants were dropped from analyses. shows results from hierarchical regressions for AL levels.
Men
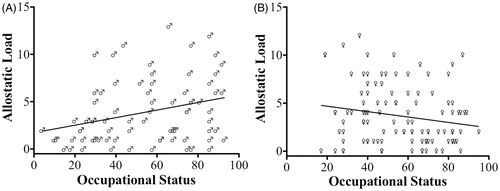
For men, AL indices were significantly associated with increased age (FModel(1,74) = 22.029, p < 0.001). OS was significantly associated with AL levels (FModel(2,73) = 13.877, p < 0.001); however, increased OS predicted increased AL indices (). Workplace stress factors did not contribute significantly to the prediction of AL and no interaction effects were detected.
Figure 2. Scatterplot illustrating the association between occupational status and allostatic load levels for (A) men (n = 76) and (B) women (n = 108). Noteworthy are the sex reversed patterns whereby increased occupational status is associated with increased allostatic load for men (p = 0.035) and decreased allostatic load for women (p = 0.048).
Women
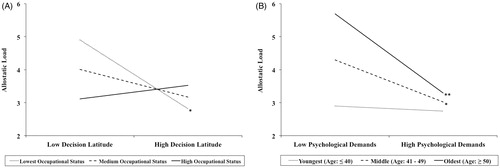
For women, AL indices were associated with increased age (FModel(1,106) = 10.002, p = 0.002). In contrast with men, lower OS predicted increased AL levels (FModel(2,105) = 7.144, p = 0.002; ). When workplace stress factors were entered (FModel(5,102) = 4.143, p < 0.001), decreased psychological demands predicted increased AL. Two significant interaction effects were found (FModel(6,101) = 4.061, p < 0.001; FModel(7,100) = 3.992, p < 0.001, respectively) between OS and decision latitude and between age and psychological demands. The simple slope analyses () revealed that among women with low OS, greater decision latitude was associated with lower AL levels (β = −0.086, p = 0.05), although this did not occur for women with medium or high OS. Secondly, simple slope analyses () showed that higher psychological demands among middle-aged women (β = −0.17, p = 0.031) and older women (β = −0.32, p = 0.003) related to lower AL levels. No such association was found for younger women.
Figure 3. Estimated allostatic load indices for women (n = 108) based for two interaction effects decomposed using simple slope regression analyses. First, (A) allostatic load indices were lower among women with lower occupational status but with higher decision latitude (p = 0.05). Occupational status appears to have an impact particularly in those with low decision latitude, while no such effect was observed among those with high decision latitude. Second, (B) allostatic load indices were significantly lower among middle-aged women (p = 0.031) and older women (p = 0.003) with higher psychological demands. **p < 0.01; *p < 0.05.
Discussion
This study investigated sex-specific interaction effects among age, OS and workplace stress in relation to symptoms of depression and anxiety as well as AL levels in healthy Montreal workers. Overall, psychiatric symptoms were associated with increased psychological demands for both sexes. In contrast, decreased decision latitude corresponded to depressive symptoms in men and anxiety symptoms in women. Moderation analyses revealed that higher social support at work was associated with fewer depressive symptoms in older men. Increased OS was associated with unfavorable AL levels for men, while the reverse was the case for women. Interestingly, women with lower OS but with higher decision latitude had lower AL levels, as did middle-aged and older women challenged with higher psychological demands. As hypothesized, our findings demonstrate that D-C-S factors interact with socio-demographic factors in sex-specific ways otherwise missed if we had only assessed main effects.
That D-C-S factors were distinctly associated with symptoms of depression and anxiety accords with existing research (Bonde, Citation2008; Karasek & Theorell, Citation1990; Theorell, Citation2000). Beyond the main effects of D-C-S factors, age moderated the beneficial effects of social support. For older men, higher social support at work was associated with lower depressive symptoms (). However, for younger women higher social support tended to protect against anxiety (). While sex differences among D-C-S factors are known to influence psychiatric symptoms (Wieclaw et al., Citation2008), this study provides important insights into the moderating effects social support exercises on age-related sex differences. Collectively, our results suggest that the moderating effect of social support garnered from work colleagues and supervisors may buffer against depression in older men and potentially against anxiety in younger women.
Distinct pathways towards psychopathology for men and women likely depend on the risk and protective factors embedded within the workplace at different ages. For instance, in the Whitehall II cohort, exertion-related conditions like psychological demands were not consistently associated with depression or anxiety symptoms, while workplace resources like decision latitude and social support were consistently shown to protect against depression and anxiety (Griffin et al., Citation2007). Because of inequalities between men and women in the distribution of certain occupations, and because certain jobs embody unique sets of D-C-S factors, it is not surprising that one model does not fit all in predicting subjective psychiatric symptoms.
Men and women may cope with workplace stress using distinct gender-based behavioral patterns adapted to different life stages (Juster & Lupien, Citation2012a). Gender refers to the implicit and explicit dissimilarities in an array of socio-culturally constructed roles, identities, and personality traits that generally predominate in one sex or the other (Juster & Lupien, Citation2012b). Gadinger et al. (Citation2010) highlighted that men are driven by achievement motivations, while women are driven by affiliation motivations (Gadinger et al., Citation2010). Perhaps younger working men striving for agency and control are less likely to build bonds in the workplace early on given their drive for greater individualism. As their position becomes more assured with increased age and OS, men may in turn reprioritize social support and thus garner more benefits against psychopathologies like depression.
By contrast, women strongly value affiliation with others throughout their lifespans, particularly under conditions of distress where they are more likely to activate “tend-and-befriend” behaviors instead of activating male-typical “fight-or-flight” behaviors (Taylor et al., Citation2000). While women may initially benefit from social networks to help face the anxieties of entering the workforce, social support at work may be less salient over time. For instance, social support garnered at work may be less important as working womens’ positions, self-confidence and skill-sets become ever more secure and stronger in parallel to growing family responsibilities that further limits non-work fraternization with colleagues. This interpretation highlights the need for further investigation in order to better understand D-C-S factors in the context of lifespan development.
Taken together, social support among our workers would have had little noticeable effect on psychological wellbeing if it had not been examined as part of a moderation analysis that took age into account. Likewise, previous investigations of Quebec workers concluded that social support by itself does not link high strain conditions to psychological distress (Bourbonnais et al., Citation1996) nor absenteeism (Bourbonnais & Mondor, Citation2001). In addition, neither age nor OS attained significance as main effects predictive of psychiatric symptoms in the current study. Our findings therefore highlight the importance of considering the interaction effects of age in studies assessing stress-related psychopathology.
Unlike psychiatric symptoms, increased age was associated with AL for both sexes in accord with existing research that confirms that chronic stress exerts a cumulative toll on the brain and body over time (Crimmins et al., Citation2003; Juster et al., Citation2010). A novel and unexpected finding from the present study is that higher OS was related to higher AL levels among men (). These findings indicate that higher occupational strata might incur a physiological cost for men. By contrast, it appears that women in higher positions may be more resilient than men in similar positions, possibly because they had to work harder and surpass many obstacles to get there. Such women either had or developed the personal resources to allow them to better cope with the responsibilities of higher status.
Alternatively, combinations of interacting biopsychosocial factors that contribute to AL in the short-term may not be the same factors that maintain them in the long-term. According to adjustment models (Frese & Zapf, Citation1988), workers develop coping mechanisms to adapt to workplace stressors and/or find ways to navigate to higher echelons within their respective occupations as they gain experience and skills. Thus, some studies might detect subtle negative health outcomes earlier on that dissipate over time (Ibrahim et al., Citation2009). Consistent with this notion, longitudinal data from Canada’s National Population Health Survey showed that psychological distress does indeed decline over time (Marchand et al., Citation2005a).
Importantly, changes in workplace conditions can have positive effects: an analysis of occupational career changes among Swedish middle-aged women revealed that highly educated women moving up the occupational hierarchy had lower AL levels compared to less educated workers who remained in unskilled work (Johansson et al., Citation2007). While more longitudinal research is needed to ascertain how life-course trajectories in SES and workplace stress mediate or moderate effects on AL, our findings using OS as a predictor of AL levels provide insights into differential social determinants of health that do not necessarily correspond between the sexes.
In the present study, workplace characteristics moderated AL levels differently depending upon women’s OS. As illustrated in , women with lower OS, but who exacted higher decision latitude at work, had lower AL levels. Recent findings indicate that individuals that are able to “shift-and-persist” out from low childhood SES might be more resilient to AL (Chen et al., Citation2012). This approach is of particular importance to those faced with social adversities as it combines “shifting” one's cognitive appraisals and emotional regulation positively to adapt to stressors as well as “persisting” by maintaining hopes for the future (Chen & Miller, Citation2012; Chen et al., Citation2012). While our results cannot directly address resiliency due to our cross-sectional design and lack of retrospective information, we speculate that increased control over one’s work is one way in which positive working conditions can moderate the otherwise negative effects of lower SES. In the context of the shift-and-persist hypothesis, we propose that protective workplace characteristics represent one avenue whereby individuals can promote their health even when unable to shift into a higher SES.
By contrast, our findings indicate that psychological demands influence AL levels with increasing age independently of SES. Initially, it may seem surprising that women with decreased psychological demands experienced increased AL levels. Yet, it is important to note that the psychological demands dimension of the D-C-S model involves non-linear effects (Karasek & Theorell, Citation1990) and threshold effects (de Jonge et al., Citation2000; Marchand et al., Citation2005a,Citationb; van der Doef et al., Citation2000). It is possible that psychological demands at tolerable levels constitute a protective factor rather than a risk factor for health outcomes. Indeed, Karasek & Theorell's (1990) original formulation stated that healthy “active workers” were those who experienced high decision latitude and high psychological demands.
Middle-aged and older women with lower psychological demands manifested the highest AL levels (), indicating that they may not be sufficiently challenged by their work. Likewise among a French cohort, less psychological demands and decision latitude corresponded with lower OS and education, particularly among older women (Niezborala et al., Citation2003). Moderation analysis in the current study revealed an adaptive tendency for women with higher psychological demands and increasing age to experience lower AL levels, underlining the variegated effects of psychological demands. Furthermore, we observed an aging gradient: as women move from middle-age to older age in the presumed absence of stimulating workplace conditions, the higher their AL levels. Prospective studies that are able to capture changes throughout the lifespan are needed to replicate and disentangle this finding further.
Limitations and strengths
Limitations
Our sample was carefully selected and our older individuals were quite healthy and disease/medication free for their age. While advantageous given our numerous biological indices, this may mean that they were also more resistant to the effects of OS and workplace stress. Hence, our findings likely underestimate the extent to which these factors influence psychological and physical health across the lifespan. Another selection bias may have been an inadvertent influence of our substantial compensation, which was set to reflect the study demands, but represented more money than many workers would have made in a workday. In addition, our medium sample size limits the strength of conclusions given the multiple statistical tests conducted. Nevertheless, our findings point to important differentials in psychiatric symptoms and physiological dysregulations as a function of age, OS, and workplace stress in a healthy sample across the working lifetime.
Given our cross-sectional analysis, the issue of temporality with respect to retrospective social conditions could not be explored. Because of the synergistic effects of age, OS, and workplace stress, it would have been of interest to explore life histories in socio-economic mobility and social and family relationships to delineate potential interactions with AL outcomes (Ryff & Singer, Citation2000; Singer & Ryff, Citation1999).
Regarding the method chosen for OS classification, Boyd’s (Citation2008) formulation gives equal weight to education and income, hence the sexes are theoretically better represented than other prestige-based composite scales that attribute different weights to adjust for gender inequalities (Hauesr & Warren, Citation1997). Strictly prestige-based OS systems are often male-derived or based on notions of social hierarchy that differ between age groups and the sexes (Lundberg, Citation2005). Our sex-specific findings vis-à-vis OS effects on AL levels indicate that men and women benefit differently from their OS. Nonetheless, other potential indices of social disparities should be explored further in relation to D-C-S factors, and other workplace stress measures like the effort/reward imbalance model could be included (Siegrist, Citation1996).
Our sex-specific AL formulation included 15 biomarkers giving equal weight to lipid, glucose, inflammatory, cardiovascular and anthropometric indices, and stress-reactive cortisol levels. Salivary cortisol samples were collected about 6–7 minutes following the initiation of each stressor (while the peak response was likely to be at 20 min), and during the morning, which likely underestimates stress responsivity (Kudielka et al., Citation2004), although we calculated area under the curve values for cortisol across the stress exposure.
There is debate in the literature concerning the appropriateness of count-based AL operationalizations that do not ascribe weight to biomarkers to evaluate AL (Beckie, Citation2012; Juster et al., Citation2010), without a consensus at present (Seplaki et al., Citation2005). For the present study, the simplicity of a count-based approach was complemented by the important inclusion of sex-specific thresholds to minimize error in systemic variation (Beckie, Citation2012).
Strengths
The study was methodologically rigorous using a healthy sample, so our conclusions are unlikely driven by extraneous factors related to measurement error or confounding characteristics. Furthermore, there are conceptual advantages to triangulating self-reported measures of psychiatric symptoms like depression and anxiety in conjunction with biomarkers indicative of physiological stress and/or precursors of pathology in the context of workplace stress studies (Ganster & Schaubroeck, Citation1991). Transdisciplinary research that incorporates psychometrics of environmental and psychosocial characteristics coupled with AL indices increasingly substantiate our knowledge-base of individual differences among risk and protective profiles (Juster et al., Citation2011a).
The inclusion of time-dependent measurement of salivary cortisol levels and repeated measures of 24 h blood pressure, and heart rate variability exemplifies how the AL model can be expanded to include dynamic measures rather than static, systemic snap-shots (Gruenewald et al., Citation2012). In concordance, tailoring our AL index to sex-specific biomarker distributions allowed insights into systemic variation among healthy male and female workers. Perhaps most importantly, our ability to detect AL differences in an otherwise healthy sample provides further support of its utility as a sub-clinical tool that is associated with important and modifiable workplace characteristics that could eventually benefit workers of diverse socio-demographic backgrounds.
Conclusions
The present study demonstrated sex-specific interaction effects of age, OS and workplace stress on symptoms of depression and anxiety and mixed findings in association with AL levels. Workplace stress evidently influences people in complex ways that will need to be further explored using larger-scale prospective studies. Beyond main effects of D-C-S factors, the moderating effects of age and OS on subjective and objective health indices highlights areas to intervene to promote employee health. For example, our moderation effects inform the following occupational health practices: (i) recognizing the age- and sex-specific protective effects of social support from colleagues and supervisors; (ii) providing increased decision latitude among women of lower OS; (iii) diversifying psychological demands of older women. Future research delineating elusive sex differences in various risk and protective factors are needed in order to further inform occupational policies that can be better tailored for both sexes of different ages and social strata.
Declaration of interest
The authors of this study have no conflicts of interest to report. This study was supported by grants awarded to Dr. D’Antono by the Canadian Institutes of Health Research (CIHR; MOP #79456) and the Fondation de l’Institut de Cardiologie de Montréal (FICM). Salary support was also awarded to Dr. D’Antono by the Fonds de la recherche en santé du Québec (FRSQ). Robert-Paul Juster is supported by doctoral scholarships from the Aging Institute of CIHR (SIA 95402) and from the Research Team on Work and Mental Health.
Acknowledgements
Thanks go to Nadia Durand for helping confirm occupational coding, Luc Brunet for helpful comments during manuscript preparation, and finally to two anonymous reviewers for their guidance during revisions.
Related Research Data
References
- Adler NE, Newman K. (2002). Socioeconomic disparities in health: pathways and policies. Health Aff (Millwood) 21:60–76
- Adler NE, Stewart J, Cohen S, Cullen M, Diez Roux A, Dow W, Evans GW, et al. (2007). Reaching for a healthier life: facts on socioeconomic status and health in the U. S. The John D. and Catherine, T. MacArthur Foundation Research Network on Socioeconomic Status and Health. Available at http://jimcov.myweb.uga.edu/3100/Adler%20et%20al%20ND%20(Reaching%20for%20a%20Healthier%20Life).pdf (accessed 16 September 2013)
- Aiken LS, West SG. (1991). Multiple regression: testing and interpreting interactions. London, UK: Sage Publications
- Beck A, Steer RA. (1993). Beck anxiety inventory manual. San Antonio, TX: Harcourt Brace and Company
- Beck AT. (1996). Manual for the Beck depression inventory. San Antonio, TX: The Psychological Corporation
- Beck AT, Epstein N, Brown G, Steer RA. (1988a). An inventory for measuring clinical anxiety: psychometric properties. J Consult Clin Psychol 56:893–7
- Beck AT, Steer RA, Brown GK. (1996). The BDI-II manual, 2nd ed. San Antonio, TX: The Psychological Corporation
- Beck AT, Steer RA, Garbin MG. (1988b). Psychometric properties of the Beck depression inventory – 25 years of evaluation. Clin Psychol Rev 8:77–100
- Beckie TM. (2012). A systematic review of allostatic load, health, and health disparities. Biol Res Nurs 14:311–46
- Blazer DG, 2nd Hybels CF. (2005). Origins of depression in later life. Psychol Med 35:1241–52
- Bonde JP. (2008). Psychosocial factors at work and risk of depression: a systematic review of the epidemiological evidence. Occup Environ Med 65:438–45
- Bourbonnais R, Brisson C, Moisan J, Vezina M. (1996). Job strain and psychological distress in white-collar workers. Scand J Work Environ Health 22:139–45
- Bourbonnais R, Mondor M. (2001). Job strain and sickness absence among nurses in the province of Quebec. Am J Ind Med 39:194–202
- Bourque P, Beaudette D. (1982). Étude psychometriques du questionnaire de dépression de Beck auprès d’un échantillon d’étudiants universitaires francophones. Rev Canad Sci Comp 14:211--18
- Boyd M. (2008). A socioeconomic scale for Canada: measuring occupational status from the census. Can Rev Socio 45:51–91
- Brenes GA. (2006). Age differences in the presentation of anxiety. Aging Ment Health 10:298–302
- Brisson C, Dion G, Moisan J, Vezina M. (1998). Reliability and validity of the French version of the 18-item Karasek Job Content Questionnaire. Work Stress 12:322–36
- Brisson C, Larocque B, Bourbonnais R. (2001). Impact of occupational stress on health status in Canada. Can J Public Health 92:460–7
- Chen E, Miller GE. (2012). “Shift-and-Persist” strategies: why being low in socioeconomic status isn’t always bad for health. Perspect Psychol Sci 7:135–58
- Chen E, Miller GE, Lachman ME, Gruenewald TL, Seeman TE. (2012). Protective factors for adults from low-childhood socioeconomic circumstances: the benefits of shift-and-persist for allostatic load. Psychosom Med 74:178–86
- Crimmins EM, Johnston M, Hayward M, Seeman T. (2003). Age differences in allostatic load: an index of physiological dysregulation. Exp Gerontol 38:731–4
- de Jonge J, Reuvers MM, Houtman IL, Bongers PM, Kompier MA. (2000). Linear and nonlinear relations between psychosocial job characteristics, subjective outcomes, and sickness absence: baseline results from SMASH. J Occup Health Psychol 5:256–68
- de Lange AH, Taris TW, Kompier MA, Houtman IL, Bongers PM. (2003). “The very best of the millennium”: longitudinal research and the demand-control-(support) model. J Occup Health Psychol 8:282–305
- Dewa CS, Lin E, Kooehoorn M, Goldner E. (2007). Association of chronic work stress, psychiatric disorders, and chronic physical conditions with disability among workers. Psychiatr Serv 58:652–8
- Freeston MH, Ladouceur R, Thibodeau N, Gagnon F, Rhéaume J. (1994). L’inventaire d’anxiété de Beck: propriétés psychométriques d’une traduction française. L’Encéphale 20:47–55
- Frese M, Zapf D. (1988). Methodological issues in the study of work stress: objective vs. subjective measurement of work stress and the question of longitudinal studies. In: Cooper CL, Payne R, editors. Causes, coping, and consequences of stress at work. Chichester, England: Wiley. p 375--411
- Fries E, Hesse J, Hellhammer J, Hellhammer DH. (2005). A new view on hypocortisolism. Psychoneuroendocrinology 30:1010–16
- Fuhrer R, Stansfeld SA. (2002). How gender affects patterns of social relations and their impact on health: a comparison of one or multiple sources of support from “close persons”. Soc Sci Med 54:811–25
- Fujishiro K, Xu J, Gong F. (2010). What does “occupation” represent as an indicator of socioeconomic status?: exploring occupational prestige and health. Soc Sci Med 71:2100–7
- Gadinger MC, Fischer J, Schneider S, Terris DD, Krückeberg K, Yamamoto S, Frank G, Kromm W. (2010). Gender moderates the health effects of job strain in managers. Int Arch Occup Environ Health 83:531–41
- Ganster DC, Schaubroeck J. (1991). Work stress and employee health. J Management 17:235–71
- Gordon JL, Ditto B, D’Antono B. (2012). Cognitive depressive symptoms associated with delayed heart rate recovery following interpersonal stress in healthy men and women. Psychophysiology 49:1082–9
- Griffin JM, Greiner BA, Stansfeld SA, Marmot M. (2007). The effect of self-reported and observed job conditions on depression and anxiety symptoms: a comparison of theoretical models. J Occup Health Psychol 12:334–49
- Gruenewald TL, Karlamangla AS, Hu P, Stein-Merkin S, Crandall C, Koretz B, Seeman TE. (2012). History of socioeconomic disadvantage and allostatic load in later life. Soc Sci Med 74:75–83
- Hauesr RM, Warren JR. (1997). Socioeconomic indexes for occupations: a review, update, and critique. Cambridge, UK: Blackwell
- Hoel H, Sparks K, Cooper CL. (2001). The cost of violence/stress at work and the benefits of a violence/stress-free working environment. Geneva: International Labor Organization
- Ibrahim S, Smith P, Muntaner C. (2009). A multi-group cross-lagged analyses of work stressors and health using Canadian National sample. Soc Sci Med 68:49–59
- ILO. (2000). Yearbook. Geneva: International Labour Office
- Johansson G, Huang Q, Lindfors P. (2007). A life-span perspective on women’s careers, health, and well-being. Soc Sci Med 65:685–97
- Juster RP, Bizik G, Picard M, Arsenault-Lapierre G, Sindi S, Trepanier L, Marin MF, et al. (2011a). A transdisciplinary perspective of chronic stress in relation to psychopathology throughout life span development. Dev Psychopathol 23:725–76
- Juster RP, Lupien S. (2012a). A sex- and gender-based analysis of allostatic load and physical complaints. Gend Med 9:511–23
- Juster RP, Lupien SJ. (2012b). Chronic stress and allostatic load. In: Schenck-Gustafsson K, DeCola PR, Pfaff DW, Pisetsky DS, editors. Handbook of clinical gender medicine. Basel: Karger AG. p 70–81
- Juster RP, McEwen BS, Lupien SJ. (2010). Allostatic load biomarkers of chronic stress and impact on health and cognition. Neurosci Biobehav Rev 35:2–16
- Juster RP, Sindi S, Marin MF, Perna A, Hashemi A, Pruessner JC, Lupien SJ. (2011b). A clinical allostatic load index is associated with burnout symptoms and hypocortisolemic profiles in healthy workers. Psychoneuroendocrinology 36:797–805
- Karasek R, Brisson C, Kawakami N, Houtman I, Bongers P, Amick B. (1998). The Job Content Questionnaire (JCQ): an instrument for internationally comparative assessments of psychosocial job characteristics. J Occup Health Psychol 3:322–55
- Karasek R, Theorell T. (1990). Healthy work: stress, productivity, and the reconstruction of working life. New York: Basic Books
- Kirschbaum C, Hellhammer DH. (1989). Salivary cortisol in psychobiological research: an overview. Neuropsychobiology 22:150–69
- Kristensen TS. (1996). Job stress and cardiovascular disease: a theoretic critical review. J Occup Health Psychol 1:246–60
- Kudielka BM, Buske-Kirschbaum A, Hellhammer DH, Kirschbaum C. (2004). HPA axis responses to laboratory psychosocial stress in healthy elderly adults, younger adults, and children: impact of age and gender. Psychoneuroendocrinology 29:83–98
- Larocque B, Brisson C, Blanchette C. (1998). Cohérence interne, validité factorielle et validité discriminante de la traduction française des échelles de demande psychologique et de latitude décisionnelle du « Job Content Questionnaire » de Karasek. Rev Epidemiol Sante Publique 46:371–81
- Lennon MC. (1987). Sex differences in distress: the impact of gender and work roles. J Health Soc Behav 28:290–305
- Levesque K, Bureau S, Moskowitz DS, Tardif JC, Lavoie J, Dupuis G, D’Antono B. (2009). Defensiveness and metabolic syndrome: impact of sex and age. Biol Psychol 80:354–60
- Levesque K, Moskowitz DS, Tardif JC, Dupuis G, D’Antono B. (2010). Physiological stress responses in defensive individuals: age and sex matter. Psychophysiology 47:332–41
- Li W, Zhang JQ, Sun J, Ke JH, Dong ZY, Wang S. (2007). Job stress related to glyco-lipid allostatic load, adiponectin and visfatin. Stress Health 23:257–66
- Lim KL, Jacobs P, Ohinmaa A, Schopflocher D, Dewa CS. (2008). A new population-based measure of the economic burden of mental illness in Canada. Chronic Dis Can 28:92–8
- Lundberg U. (2005). Stress hormones in health and illness: the roles of work and gender. Psychoneuroendocrinology 30:1017–21
- Maclean H, Glynn K, Ansara D. (2004). Multiple roles and women’s mental health in Canada. BMC Womens Health 4(Suppl 1):S3
- Marchand A. (2007). Mental health in Canada: Are there any risky occupationsand industries? Int J Law Psychiat 30:272–83
- Marchand A, Demers A, Durand P. (2005a). Do occupation and work conditions really matter? A longitudinal analysis of psychological distress experiences among Canadian workers. Sociol Health Illn 27:602–27
- Marchand A, Demers A, Durand P. (2005b). Does work really cause distress? The contribution of occupational structure and work organization to the experience of psychological distress. Soc Sci Med 60:1–14
- Marchand A, Durand P. (2011). Psychological distress, depression, and burnout: similar contribution of the Job Demand-Control and Job Demand-Control-Support models. J Occup Environ Med 53:185–9
- Marchand A, Durand P, Demers A. (2005c). Work and mental health: the experience of the Quebec workforce between 1987 and 1998. Work 25:135–42
- Marmot M. (2004). The status syndrome: how social standing affects our health and longevity. New York: Henry Holt and Company
- Marmot MG, Smith GD, Stansfeld S, Patel C, North F, Head J, White I, et al. (1991). Health inequalities among British civil servants: the Whitehall II study. Lancet 337:1387–93
- McCaffery JM, Marsland AL, Strohacker K, Muldoon MF, Manuck SB. (2012). Factor structure underlying components of allostatic load. PLoS One 7:e47246
- McEwen BS, Gianaroe PJ. (2010). Central role of the brain in stress and adaptation: links to socioeconomic status, health, and disease. In: Adler NE, Steward J, editors. The biology of disadvantage: socioeconomic status and health (Annals of the New York Academy of Sciences). Hoboken, NJ: Wiley-Blackwell. p 190–222
- McEwen BS, Seeman T. (1999). Protective and damaging effects of mediators of stress. Elaborating and testing the concepts of allostasis and allostatic load. Ann NY Acad Sci 896:30–47
- McEwen BS, Stellar E. (1993). Stress and the individual. Mechanisms leading to disease. Arch Intern Med 153:2093–101
- McEwen BS, Tucker P. (2011). Critical biological pathways for chronic psychosocial stress and research opportunities to advance the consideration of stress in chemical risk assessment. Am J Public Health 101(Suppl 1):S131–9
- Messing K, Tissot F, Saurel-Cubizolles MJ, Kaminski M, Bourgine M. (1998). Sex as a variable can be a surrogate for some working conditions: factors associated with sickness absence. J Occup Environ Med 40:250–60
- Muhonen T, Torkelson E. (2003). The demand-control-support model and health among women and men in similar occupations. J Behav Med 26:601–13
- Nam CB. (2000). Comparison of three occupational scales. Tallahasse, FL: Centre for the Study of Population
- Nam CB, Boyd M. (2004). Occupational status in 2000: over a century of census-based measurement. Popul Res Policy Rev 23:327–58
- Niezborala M, Marquie J-C, Baracat B, Esquirol Y, Soulat J-M. (2003). Job stress and occupational status in a French cohort. Rev Epidemiol Sante Publique 51:607–16
- Piltch CA, Walsh DC, Mangione TW, Jennings SE. (1994). Gender, work, and mental distress in an industrial labor force: an expansion of Karasek’s job strain model. In: Keita GP, Hurrell JJ Jr, editors. Job stress in a change workforce: investigating gender, diversity, and family issues. Washington, DC: American Psychological Association. p 39–54
- Plaisier I, de Bruijn JGM, de Graaf R, ten Have M, Beekman ATF, Penninx BWJH. (2007). The contribution of working conditions and social support to the onset of depressive and anxiety disorders among male and female employees. Soc Sci Med 64:401–10
- Pruessner JC, Kirschbaum C, Meinlschmid G, Hellhammer DH. (2003). Two formulas for computation of the area under the curve represent measures of total hormone concentration versus time-dependent change. Psychoneuroendocrinology 28:916–31
- Ryff CD, Singer BH. (2000). Biopsychosocial challenges of the new millennium. Psychother Psychosom 69:170–7
- Schnorpfeil P, Noll A, Schulze R, Ehlert U, Frey K, Fischer JE. (2003). Allostatic load and work conditions. Soc Sci Med 57:647–56
- Seedat S, Scott KM, Angermeyer MC, Berglund P, Bromet EJ, Brugha TS, Demyttenaere K, et al. (2009). Cross-national associations between gender and mental disorders in the World Health Organization World Mental Health Surveys. Arch Gen Psychiatry 66:785–95
- Seeman E, Singer BH, Rowe J, Horwitz RI, McEwen B. (1997). Price of adaptation – allostatic load and its health consequences. Arch Intern Med 157:2259–68
- Seeman TE, McEwen BS, Rowe JW, Singer BH. (2001). Allostatic load as a marker of cumulative biological risk: MacArthur studies of successful aging. Proc Natl Acad Sci USA 98:4770–5
- Seplaki CL, Goldman N, Glei D, Weinstein M. (2005). A comparative analysis of measurement approaches for physiological dysregulation in an older population. Exp Gerontol 40:438–49
- Seplaki CL, Goldman N, Weinstein M, Lin YH. (2006). Measurement of cumulative physiological dysregulation in an older population. Demography 43:165–83
- Sherwood A, Gullette EC, Hinderliter AL, Georgiades A, Babyak M, Waugh RA, Blumenthal JA. (2002). Relationship of clinic, ambulatory, and laboratory stress blood pressure to left ventricular mass in overweight men and women with high blood pressure. Psychosom Med 64:247–57
- Siegrist J. (1996). Adverse health effects of high-effort/low-reward conditions. J Occup Health Psychol 1:27–41
- Singer B, Ryff CD. (1999). Hierarchies of life histories and associated health risks. Ann NY Acad Sci 896:96–115
- Stansfeld S, Candy B. (2006). Psychosocial work environment and mental health – a meta-analytic review. Scand J Work Environ Health 32:443–62
- Stansfeld S, Feeney A, Head J, Canner R, North F, Marmot M. (1994). Sickness absence for psychiatric illness: the Whitehall II study. Soc Sci Med 40:189–97
- Stansfeld SA, Fuhrer R, Head J, Ferrie J, Shipley M. (1997). Work and psychiatric disorder in the Whitehall II Study. J Psychosom Res 1997:73–81
- Stansfeld SA, Fuhrer R, Shipley MJ, Marmot MG. (1999). Work characteristics predict psychiatric disorder: prospective results from the Whitehall II Study. Occup Environ Med 56:302–7
- Stansfeld SA, Head J, Fuhrer R, Wardle J, Cattell V. (2003). Social inequalities in depressive symptoms and physical functioning in the Whitehall II study: exploring a common cause explanation. J Epidemiol Community Health 57:361–7
- Sun J, Wang S, Zhang JQ, Li W. (2007). Assessing the cumulative effects of stress: the association between job stress and allostatic load in a large sample of Chinese employees. Work Stress 21:333–47
- Szanton SL, Gill JM, Allen JK. (2005). Allostatic load: a mechanism of socioeconomic health disparities? Biol Res Nurs 7:7–15
- Taylor SE, Klein LC, Lewis BP, Gruenewald T, Gurung RA, Updegraff JA. (2000). Biobehavioral responses to stress in females: tend-and-befriend, not fight-or-flight. Psychol Rev 107:411--29
- Theorell T. (2000). Working conditions and health. In: Berkman L, IKawachi I, editors. Social epidemiology. Oxford: Oxford University Press. p 95--117
- van der Doef M, Maes S, Diekstra R. (2000). An examination of the job demand-control-support model with various occupational strain indicators. Anxiety Stress Coping 13:165–85
- Vermeulen M, Mustard C. (2000). Gender differences in job strain, social support at work, and psychological distress. J Occup Health Psychol 5:428–40
- Wege N, Dragano N, Erbel R, Jockel K-H, Moebus S, Stang A, Siegrist J. (2008). When does work stress hurt? Testing the interaction with socioeconomic position in the Heinz Nixdorf Recall Study. J Epi Comm Health 62:338–41
- Westerlund H, Gustafsson PE, Theorell T, Janlert U, Hammarstrom A. (2012). Social adversity in adolescence increases the physiological vulnerability to job strain in adulthood: a prospective population-based study. PLoS One 7:e35967
- Wieclaw J, Agerbo E, Mortensen PB, Burr H, Tuchsen F, Bonde JP. (2008). Psychosocial working conditions and the risk of depression and anxiety disorders in the Danish workforce. BMC Public Health 8:280
- Winer BJ. (1962). Statistical principles in experimental design, 2nd ed. New York: McGraw-Hill Book Company. p 379