
Abstract
We examined whether lifetime exposure to stressful and traumatic events alters hypothalamic-pituitary-adrenal (HPA) axis functioning, as indexed by hair cortisol, regardless of associated psychopathology, among pregnant women of different racial/ethnic backgrounds. 180 women provided hair samples for measurement of integrated cortisol levels throughout pregnancy and information regarding their lifetime exposure to stressful and traumatic life events. Results indicate that increased lifetime exposure to traumatic events was associated with significantly greater hair cortisol over the course of pregnancy. Similarly, greater lifetime exposure to stressful and traumatic events weighted by reported negative impact (over the previous 12 months) was associated with significantly greater hair cortisol during pregnancy. All analyses controlled for maternal age, education, body mass index (BMI), use of inhaled corticosteroids, race/ethnicity, and post-traumatic stress disorder (PTSD) and depressive symptoms. Following stratification by race/ethnicity, associations between stressful and traumatic life events and hair cortisol were found among Black women only. This is the first study to consider associations between lifetime stress exposures and hair cortisol in a sociodemographically diverse sample of pregnant women. Increased exposure to stressful and traumatic events, independent of PTSD and depressive symptoms, was associated with higher cortisol production, particularly in Black women. Future research should investigate the influence of such increased cortisol exposure on developmental outcomes among offspring.
Introduction
Despite growing evidence linking prenatal maternal stress to adverse developmental outcomes in children, the underlying mechanisms remain poorly understood. The HPA axis coordinates many basic physiological functions and the body’s stress response (Bailey et al., Citation2013). Functioning of the maternal HPA axis during pregnancy plays an important role in early child development, including cognitive, behavorial and physical development (O'Donnell et al., Citation2009; Wadhwa, Citation2005; Weinstock, Citation2005; Wright et al., Citation2013), and pregnancy is marked by important changes in HPA axis functioning (D'Anna-Hernandez et al., Citation2011; Kirschbaum et al., Citation2009; McLean et al., Citation1995).
Hair cortisol is emerging as an integrative measure of HPA axis activity (Staufenbiel et al., Citation2013), reflecting cortisol production over weeks to months. Recent data support the use of hair cortisol as a retrospective calendar of cortisol production over the course of pregnancy (D'Anna-Hernandez et al., Citation2011; Kirschbaum et al., Citation2009), prompting a call for the integration of hair sampling into epidemiological studies of pregnant women as well as ethnically, racially and socioeconomically diverse samples to fill identified research gaps (Wosu et al., Citation2013). Importantly, stressful life experiences are not evenly distributed, with individuals from lower socioeconomic status (SES) environments and members of racial/ethnic minority groups exposed to higher rates (Hatch & Dohrenwend, Citation2007; Roberts et al., Citation2011). Nonetheless, studies examining how women’s lifetime exposure to stressful life experiences influence cortisol production, especially during pregnancy and among ethnic minorities, are sparse (Shea et al., Citation2007). Notably, a number of studies in pregnant and non-pregnant samples have reported links between hair cortisol and stress or trauma exposures, though other studies have failed to find such associations (Kalmakis et al., Citation2015; Kalra et al., Citation2007; Russell et al., Citation2012; Staufenbiel et al., Citation2013; Wosu et al., Citation2013).
Related research links lifetime psychopathology, including PTSD symptomatology, to exposure to stressful and traumatic events and altered HPA axis functioning (Meewisse et al., Citation2007), although the majority of exposed individuals do not develop PTSD (Breslau, Citation2001; Breslau et al., Citation1998; Bronner et al., Citation2009). Similarly, depressive symptoms are associated with childhood trauma and HPA axis functioning (Hinkelmann et al., Citation2013). These findings have spurred interest in examining associations between exposure to traumatic events and HPA axis disruption independent of PTSD and depressive symptoms to determine whether traumatic exposures may impact HPA axis functioning in the absence of psychopathology (de Kloet et al., Citation2007; Klaassens et al., Citation2010; Meewisse et al., Citation2007). At the same time, experiencing stressful events that do not meet official trauma criteria can also have serious consequences for well-being (Cohen et al., Citation2012; Tosevski & Milovancevic, Citation2006). Hence, effects of traumatic and non-traumatic stressful life events on HPA axis functioning need to be considered. In the current study, we assessed associations between lifetime exposure to non-traumatic and traumatic stressful life events and cortisol production measured from scalp hair, independent of PTSD and depressive symptoms, in a multi-racial/ethnic sample of pregnant women.
Materials and methods
Participants
Participants were part of the Programing of Intergenerational Stress Mechanisms (PRISM) study, a prospective cohort originally funded to recruit N = 275 pregnant women and their children to examine the role of prenatal stress on respiratory health in children. Women were recruited at 26.9 (SD = 8.1) weeks’ gestation from the Beth Israel Deaconess Medical Center and the East Boston Neighborhood Health Center from March 2011 to August 2012. Women had to be at least 18 years of age, free of chronic illness, fluent in English or Spanish, and not have endorsed drinking more than seven alcoholic drinks per week prior to pregnancy recognition or any alcohol after pregnancy recognition. Subsequent funding allowed for the collection of hair for cortisol assessment starting a short time into the recruitment phase. Two hundred twenty-five women were approached to participate in hair collection; women were excluded from participation due to shift work (n = 17), exogenous steroid use (n = 5) in the past six months, or multigestational pregnancy (n = 6), as these factors may influence cortisol production (Granger et al., Citation2009). Those identifying as multi-racial/ethnic (n = 17) were excluded from analysis. Women not included in these analyses did not differ significantly from those included based on mean age, BMI, smoking or education level. See for participant characteristics.
Table 1. Sample descriptives.
Procedure
Participants provided written informed consent; the study was approved by the relevant institutions’ human studies ethics committees. Participant demographics were assessed shortly following recruitment. Within 2 weeks of enrollment, trained research assistants administered questionnaires to assess women’s lifetime exposure to stressful (non-traumatic and traumatic) life events, and PTSD and depressive symptoms. Around the time of delivery, women provided hair samples as part of a follow-up study visit at home or in the woman’s health clinic.
Assessment of lifetime exposure to stressful and traumatic events
Within 2 weeks of enrollment, trained research assistants assessed women’s lifetime exposure to stressful and potentially traumatic events using the 30-item Life Stressor Checklist-Revised (LSC-R) (Wolfe & Kimerling, Citation1997). The LSC-R includes items of particular relevance to women (e.g. rape, abortion, interpersonal violence) and questions to determine whether each endorsed event met the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) PTSD Criterion A (e.g. during the event, the respondent believed that she or someone else could be killed or seriously harmed; American Psychiatric Association, Citation2000).
Two scores were calculated from the LSC-R. First, a weighted score of all endorsed stressful life events (traumatic and non-traumatic) that considered the self-reported negative impact of each event was computed. Specifically, each endorsed event was multiplied by a score ranging from 1 (not at all) to 5 (extremely) reflecting the participant’s assessment of the severity of the negative impact this event had had on her during the past 12 months. Scores could range from 0 to 150 (range in present sample = 0–96), with higher scores indicating greater exposure to and impact of exposure to stressful and traumatic events. Second, a score reflecting the number of endorsed lifetime traumatic events (i.e. events that met the DSM-IV PTSD Criterion A was calculated; this score did not consider the participant’s assessment of the perceived negative impact of the event). Higher scores indicate exposure to more traumatic events (range in present sample = 0–11). Internal reliability was good at Cronbach’s α = 0.86 for the weighted score, and Cronbach’s α = 0.93 for the traumatic event score, respectively, similar to previous reports (Wolfe & Kimerling, Citation1997).
Hair cortisol assessment
Hair cortisol was assessed in women’s scalp hair, collected shortly following delivery. A hair sample (approximately 3 mm in diameter) was cut as close as possible to the scalp from a posterior vertex position. Hair samples were cut into three 3 cm segments, length permitting, with each 3 cm segment corresponding to one pregnancy trimester based on a hair growth rate of approximately 1 cm/month (Wennig, Citation2000), as previously described (Kirschbaum et al., Citation2009). Due to individual differences in hair length, 100 (55.6%) women provided hair samples long enough for the assessment of hair cortisol during all three trimesters, 65 (36.1%) women for the second and third trimesters only, and 15 (8.3%) women for the third trimester only.
Hair samples were shipped to Dresden, Germany for analysis in the Kirschbaum Laboratory. Washing and steroid extraction followed a previously described protocol (Stalder et al., Citation2013). Hair was washed in isopropanol, and cortisol was extracted from 7.5 mg of whole non-pulverized hair using methanol in the presence of internal standards. Samples were centrifuged at 15,200g, and the supernatant was collected; alcohol was evaporated under a stream of nitrogen and reconstituted with double-distilled water and then injected into a Shimadzu HPLC-tandem mass spectrometry system (Shimadzu, Canby, OR, USA) coupled to an AB Sciex API 5000 Turbo-ion-spray triple quadrupole tandem mass spectrometer (AB Sciex, Foster City, CA) with purification by on-line solid-phase extraction (Gao et al., Citation2013). Lower limits of quantification were 0.1 pg/mg; inter- and intra-assay variabilities were 3.7–8.8%.
Covariates
Mothers self-reported their age, highest level of education and race/ethnicity. Race/ethnicity was coded to compare Black and Hispanic women to White women. Prenatal BMI was computed as kg/m2 based on mother’s self-reported height and pre-pregnancy weight. Internal validation data comparing self-reported height and weight with measured height and weight among a subsample of participants recruited into a sociodemographically similar Boston birth cohort during early pregnancy (<10 weeks gestation) suggest good agreement between self-reported and measured data across all levels of height and weight (Wright et al., Citation2013).
To investigate effects of exposure to stressful and traumatic life events independent of PTSD and depressive symptoms, PTSD symptomatology was assessed two weeks after enrollment using the Posttraumatic Stress Disorder Checklist – Civilian Version (PCL-C). The PCL-C consists of 17 items assessing DSM-IV symptom criteria for PTSD, including re-experiencing, avoidance and numbing, and hyperarousal symptoms (Weathers et al., Citation1991), and has established reliability and validity, including correspondence with clinical diagnostic interviews for PTSD (Weathers et al., Citation2001). Mothers indicated how much they had been bothered by each of these symptoms since the occurrence of the most stressful event they experienced on a 5-point scale; higher scores indicate greater symptoms. Internal reliability in the present sample was high at Cronbach’s α = 0.99, but comparable to previous reports of internal reliability (Wilkins et al., Citation2011). At the same time, depressive symptoms were assessed using the Edinburgh Postnatal Depression Scale (EPDS). The EPDS consists of 10 items assessing common depressive symptoms experienced over the past seven days and has been shown to be both reliable and valid among pregnant and postpartum women and to correspond to clinical ratings of depression (Cox et al., Citation1987). Responses were made on a 4-point scale; higher scores indicate greater depressive symptoms. Cronbach’s alpha in the present sample was good at α = 0.80, similar to previous reports (Cox et al., Citation1987).
Finally, mothers completed a questionnaire to provide information about their hair and hair care routines and indicated whether or not they had used inhaled corticosteroids (ICS) during the previous 12 months, as ICS use has the potential to alter cortisol production (Dahl, Citation2006). See for correlations between the main study variables.
Statistical analyses
Levels of hair cortisol were log-transformed to reduce skewness. Mixed-effects models allowing for within-subject correlated observations and assuming independence across participants were used to test the effects of maternal lifetime exposure to stressful and traumatic events on women’s hair cortisol levels throughout pregnancy. Analyses were performed using the entire sample and subsequently stratified by race/ethnicity. All analyses controlled for maternal age, education, ICS use, pre-pregnancy BMI, PTSD and depressive symptoms and, in non-stratified analyses, race/ethnicity. A first-order autoregressive correlation pattern was assumed for the within-subject observations, such that observations from adjacent trimesters were assumed to be more highly correlated than those between the first and third trimesters. Residual analyses were used to verify the assumptions of the model. The 1 degree of freedom (df) tests of associations between stressful and traumatic events and hair cortisol levels during pregnancy were the primary tests. Racial/ethnic group differences with respect to hair cortisol and stressful and traumatic life events were analyzed using one-way ANOVAs with three levels (White, Black, Hispanic), followed, if significant, by Hochberg’s GT2 for post-hoc comparison of the group means. Analyses were performed using SAS software, Version 9.3, and SPSS Version 20 (IBM, New York, NY). For all analyses, p < 0.05 was considered statistically significant.
Results
Cohort description
provides detailed information regarding participant characteristics. In this racially/ethnically mixed sample, 64 (35.6%) women self-identified as Caucasian, 34 (18.9%) as Black, and 82 (45.6%) as Hispanic.
Lifetime exposure to stressful and traumatic events and hair cortisol
Correlations of hair cortisol across pregnancy trimesters were high (0.93 for adjacent trimesters and 0.86 for observations between the 1st and 3rd trimesters), suggesting that women with higher cortisol levels during any trimester tended to have higher values during the other two trimesters. When considering the entire sample, maternal lifetime exposure to more traumatic events (i.e. without consideration for exposure to stressful, non-traumatic events) was significantly associated with greater maternal hair cortisol during pregnancy, F(1, 161) = 5.49, p = 0.020. Greater impact of lifetime exposure to stressful life events (traumatic and non-traumatic) over the prior 12 months was also significantly associated with higher hair cortisol during pregnancy, F(1, 162) = 5.51, p = 0.020.
Table 2. Correlation matrix for main study variables.
Race/ethnicity, exposure to stressful and traumatic events, and hair cortisol
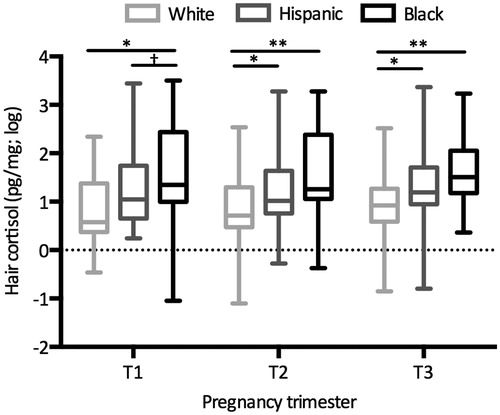
There was a significant effect of race/ethnicity on maternal lifetime exposure to traumatic events [F(2, 176) = 3.67, p = 0.027] and on recent impact of maternal lifetime exposure to stressful (non-traumatic and traumatic) events [F(2, 177) = 6.91, p = 0.001]. Specifically, Black women reported significantly higher levels of lifetime exposure to traumatic events than White, though not Hispanic, women and significantly higher levels of recent impact of lifetime exposure to stressful (non-traumatic and traumatic) events than White and Hispanic women (, ). There was also a significant effect of race/ethnicity on hair cortisol during the first [F(2, 97) = 4.74, p = 0.011], second [F(2, 162) = 7.97, p = 0.001], and third [F(2, 177) = 10.43, p < 0.001] trimester. Specifically, Black women had significantly higher hair cortisol levels than White, though not Hispanic, women during all three trimesters. Hispanic women had marginally higher hair cortisol levels than White women during the first trimester and significantly higher hair cortisol levels during the second and third trimesters ().
Figure 1. Maternal lifetime exposure to and recent impact from stressful and traumatic events by race/ethnicity. Maternal lifetime exposure to and recent impact from stressful and traumatic events varied as a function of race/ethnicity. Boxplots display full range of scores. Panel (a) Black women reported higher levels of recent impact of lifetime exposure to stressful (non-traumatic and traumatic) events than White and Hispanic women.
Panel (b) Black women reported greater lifetime exposure to traumatic events than White but not Hispanic women. Panel (c) Maternal PTSD symptoms since the most stressful event varied marginally by race/ethnicity; post-hoc tests revealed no significant differences among groups. Hair cortisol by race/ethnicity across pregnancy trimesters. *p < 0.05, **p < 0.01.
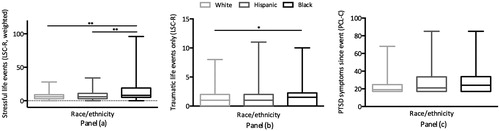
Figure 2. Maternal hair cortisol by pregnancy trimester and race/ethnicity. Hair cortisol varied significantly as a function of race/ethnicity during all pregnancy trimesters. Boxplots display full range of scores. Black women had significantly higher hair cortisol levels than White but not Hispanic women during all trimesters. Hispanic women had marginally higher hair cortisol levels than White women during the first trimester and significantly higher hair cortisol levels during the second and third trimesters. †p < 0.10, *p < 0.05, **p < 0.01.
Given the observed effects of race/ethnicity on lifetime exposure to stressful and traumatic events as well as hair cortisol levels, analyses were repeated stratified by race/ethnicity. These analyses revealed that greater lifetime exposure to traumatic events was associated with greater hair cortisol among Black women [F(1, 25) = 4.84, p = 0.037], but not among White [F(1, 53) = 0.55, p = 0.462] or Hispanic [F(1, 70) = 0.74, p = 0.392] women. Similarly, there was a significant and positive association between recent impact of lifetime exposure to stressful and traumatic events and hair cortisol during pregnancy among Black women [F(1, 25) = 5.61, p = 0.026], but not among White [F(1, 54) = 0.02, p = 0.888] or Hispanic [F(1, 70) = 0.06, p = 0.800] women.
Sensitivity analyses
Analyses were repeated on only the 100 women for whom hair cortisol levels could be measured during all trimesters; all findings reported above remained significant.
In addition, some women reported very high levels of lifetime exposure to traumatic life events, recent impact of lifetime exposure to stressful life events and PTSD symptoms (). To take a more conservative approach, the analyses were repeated after reducing all scores (five scores of lifetime exposure to traumatic life events, three scores of recent impact of lifetime exposure to stressful life events, four PTSD symptom scores) exceeding three standard deviations from the mean to the next highest score. The above reported results remained significant and our conclusions did not change.
Discussion
To our knowledge, this is the first study to test associations between maternal lifetime exposure to stressful and traumatic life events and an integrated measure of cortisol assessed in scalp hair in pregnant women. Importantly, these associations were investigated in a racially/ethnically diverse sample that included White, Black and Hispanic women and adjusted for a number of covariates, including maternal education, BMI, steroid use, and PTSD and depressive symptoms. The results indicated that greater lifetime exposure to traumatic life events and increased impact in the past 12 months from lifetime exposure to stressful and traumatic events were each associated with greater hair cortisol during pregnancy. When stratifying by race/ethnicity, this effect was only seen among Black women.
Notably, two indices of maternal lifetime exposure to stressful life events were considered, one reflecting lifetime exposure to stressful life events weighted by participants’ recent experience of the negative impact of the event, regardless of whether or not the event met the DSM-IV PTSD Criterion A, and a second index reflecting the number of lifetime traumatic events experienced, i.e. only events that met DSM-IV PTSD Criterion A. Significant associations for both measures with maternal hair cortisol emerged, suggesting that considering events that women perceive to have negatively impacted them, as well as their personal evaluation of the magnitude of this negative impact, may be as strongly associated with HPA axis functioning as the number of experienced events meeting DSM trauma criteria.
Interestingly, both Black and Hispanic pregnant women had higher hair cortisol levels than White women, but in analyses stratified by race/ethnicity, there was an association between increased exposure to lifetime stressful and traumatic life events and elevated hair cortisol only among Black women, suggesting that they may be uniquely vulnerable to persistent pathophysiological consequences of cumulative stress exposures. As Black women also reported significantly greater stress impact scores compared to White and Hispanic women, Black women may have been more negatively affected by exposures to stressful and traumatic life events, e.g. due to lower levels of social support (Small, Citation2007), or there may be differences in the reporting of stressful and traumatic life events among Black compared to Hispanic women. These findings also converge with those from previous studies that have found greater cumulative stress exposure to be associated with increases in corticotropin-releasing hormone only among Black women (Tse et al., Citation2012) and altered diurnal salivary cortisol rhythms (lower morning cortisol and flatter cortisol slopes over the course of the day) among pregnant Black, but not Hispanic, women (Suglia et al., Citation2010). Existing data further indicate that both Black and Hispanic adults’ diurnal salivary cortisol rhythms differ not only from those of Whites but also from each other (Hajat et al., Citation2010). Specifically, a previous study reported that both Blacks and Hispanics had flatter declines in morning cortisol relative to Whites; however, whereas Blacks had flatter cortisol declines in the evening, Hispanics had steeper evening cortisol declines. Hence, these data also suggest differences in HPA axis functioning among Blacks and Hispanics that warrant further investigation.
Similar to other research, Black women in this sample were disproportionally exposed to more traumatic events over their lifecourse (Hatch & Dohrenwend, Citation2007; Roberts et al., Citation2011). Thus, an alternative explanation for the finding that exposure effects were evident only among Black participants could be that a certain exposure threshold must be reached to impact cortisol levels and that the Black women in this sample were the only subgroup to experience sufficiently high rates of stressful and traumatic life events to reach such a threshold.
Also of note, associations between increased lifetime exposure to stressful and traumatic events and elevated hair cortisol were found after controlling for PTSD and depressive symptoms. These findings suggest that exposure to stressful and traumatic events, regardless of the development of PTSD or depression, may be sufficient to alter functioning of the HPA axis. Previous studies have also reported altered hair cortisol levels among individuals exposed to a potentially traumatic event, irrespective of whether or not they developed PTSD (Steudte et al., Citation2013).
The present study has a number of strengths, including its focus on pregnant women, the racially/ethnically diverse sample, and the use of an integrated measure of long-term cortisol output. Nonetheless, some limitations should be noted. As this was not a prospective study, reports of stressful and traumatic events and PTSD symptoms were based on participant recall. However, the LSC-R has previously successfully been used in community samples (Wolfe & Kimerling, Citation1997). Also, research suggests that hair segments dating back more than 6 months may contain lower cortisol levels due to washout effects and that best practices may include collecting multiple hair samples over the course of pregnancy to minimize any washout effects. Finally, very little is known about differential hair growth rates among individuals from different racial/ethnic backgrounds (Baque et al., Citation2012; Loussouarn et al., Citation2005), but reported differences are small (Loussouarn, Citation2001; Loussouarn et al., Citation2005).
Conclusions
Black and Hispanic women reported greater lifetime exposure to traumatic events than White women, but only among Black women was greater exposure associated with increased hair cortisol during pregnancy. Future research should examine the extent to which stress-induced differences in maternal prenatal HPA axis functioning are associated with poorer developmental outcomes among offspring and how these effects may be moderated by race/ethnicity. Observed racial/ethnic differences may provide insight into understanding existing health disparities.
Declaration of interest
The authors report no conflicts of interest. The PRISM cohort is funded by R01 HL095606 (RJW, MBE); hair analyses were supported by the Mindich Child Health & Development Institute (RJW). During preparation of this manuscript, MBE was supported by the Program for Behavioral Science, Department of Psychiatry, Boston Children’s Hospital. Funding sources had no involvement in study design, data collection, data analysis and interpretation, the writing of the report, or the decision to submit the article for publication.
| Abbreviations | ||
| BMI | = | body mass index |
| DSM-IV | = | Diagnostic and Statistical Manual of Mental Disorders, 4th Edition |
| HPA | = | hypothalamic-pituitary-adrenal |
| ICS | = | inhaled corticosteroids |
| PTSD | = | post-traumatic stress disorder |
| SES | = | socioeconomic status. |
References
- American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders, Test Revision (DSSM-IV-TR). Washington, DC: APA
- Bailey CR, Cordell E, Sobin SM, Neumeister A. (2013). Recent progress in understanding the pathophysiology of post-traumatic stress disorder: implications for targeted pharmacological treatment. CNS Drugs 27:221–32
- Baque CS, Zhou J, Gu W, Collaudin C, Kravtchenko S, Kempf JY, Saint-Leger D. (2012). Relationships between hair growth rate and morphological parameters of human straight hair: a same law above ethnical origins? Int J Cosmet Sci 34:111–16
- Breslau N. (2001). The epidemiology of posttraumatic stress disorder: what is the extent of the problem? J Clin Psychiatry 62(Suppl 17):16–22
- Breslau N, Kessler RC, Chilcoat HD, Schultz LR, Davis GC, Andreski P. (1998). Trauma and posttraumatic stress disorder in the community: the 1996 Detroit Area Survey of Trauma. Arch Gen Psychiatry 55:626–32
- Bronner MB, Peek N, Vries M, Bronner AE, Last BF, Grootenhuis MA. (2009). A community-based survey of posttraumatic stress disorder in the Netherlands. J Trauma Stress 22:74–8
- Cohen S, Janicki-Deverts D, Doyle WJ, Miller GE, Frank E, Rabin BS, Turner RB. (2012). Chronic stress, glucocorticoid receptor resistance, inflammation, and disease risk. Proc Natl Acad Sci USA 109:5995–9
- Cox JL, Holden JM, Sagovsky R. (1987). Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. Br J Psychiatry 150:782–6
- D'Anna-Hernandez KL, Ross RG, Natvig CL, Laudenslager ML. (2011). Hair cortisol levels as a retrospective marker of hypothalamic-pituitary axis activity throughout pregnancy: comparison to salivary cortisol. Physiol Behav 104:348–53
- Dahl R. (2006). Systemic side effects of inhaled corticosteroids in patients with asthma. Resp Med 100:1307–17
- de Kloet CS, Vermetten E, Heijnen CJ, Geuze E, Lentjes EG, Westenberg HG. (2007). Enhanced cortisol suppression in response to dexamethasone administration in traumatized veterans with and without posttraumatic stress disorder. Psychoneuroendocrinology 32:215–26
- Gao W, Stalder T, Foley P, Rauh M, Deng H, Kirschbaum C. (2013). Quantitative analysis of steroid hormones in human hair using a column-switching LC-APCI-MS/MS assay. J Chromatogr B Analyt Technol Biomed Life Sci 928:1–8
- Granger DA, Hibel LC, Fortunato CK, Kapelewski CH. (2009). Medication effects on salivary cortisol: tactics and strategy to minimize impact in behavioral and developmental science. Psychoneuroendocrinology 34:1437–48
- Hajat A, Diez Roux A, Franklin TG, Seeman T, Shrager S, Ranjit N, Castro C, et al. (2010). Socioeconomic and race/ethnic differences in daily salivary cortisol profiles: the multi-ethnic study of atherosclerosis. Psychoneuroendocrinology 35:932–43
- Hatch SL, Dohrenwend BP. (2007). Distribution of traumatic and other stressful life events by race/ethnicity, gender, SES and age: a review of the research. Am J Community Psychol 40:313–32
- Hinkelmann K, Muhtz C, Dettenborn L, Agorastos A, Wingenfeld K, Spitzer C, Gao W, et al. (2013). Association between childhood trauma and low hair cortisol in depressed patients and healthy control subjects. Biol Psychiatry 74:e15–17
- Kalmakis KA, Meyer JS, Chiodo L, Leung K. (2015). Adverse childhood experiences and chronic hypothalamic-pituitary-adrenal activity. Stress 18:446–50
- Kalra S, Einarson A, Karaskov T, Van Uum S, Koren G. (2007). The relationship between stress and hair cortisol in healthy pregnant women. Clin Invest Med 30:103–7
- Kirschbaum C, Tietze A, Skoluda N, Dettenborn L. (2009). Hair as a retrospective calendar of cortisol production-Increased cortisol incorporation into hair in the third trimester of pregnancy. Psychoneuroendocrinology 34:32–7
- Klaassens ER, Giltay EJ, van Veen T, Veen G, Zitman FG. (2010). Trauma exposure in relation to basal salivary cortisol and the hormone response to the dexamethasone/CRH test in male railway employees without lifetime psychopathology. Psychoneuroendocrinology 35:878–86
- Loussouarn G. (2001). African hair growth parameters. Br J Dermatol 145:294–7
- Loussouarn G, El Rawadi C, Genain G. (2005). Diversity of hair growth profiles. Int J Dermatol 44(Suppl1):6–9
- McLean M, Bisits A, Davies J, Woods R, Lowry P, Smith R. (1995). A placental clock controlling the length of human pregnancy. Nat Med 1:460–3
- Meewisse ML, Reitsma JB, de Vries GJ, Gersons BP, Olff M. (2007). Cortisol and post-traumatic stress disorder in adults: systematic review and meta-analysis. Br J Psychiatry 191:387–92
- O'Donnell K, O'Connor TG, Glover V. (2009). Prenatal stress and neurodevelopment of the child: focus on the HPA axis and role of the placenta. Dev Neurosci 31:285–92
- Roberts AL, Gilman SE, Breslau J, Breslau N, Koenen KC. (2011). Race/ethnic differences in exposure to traumatic events, development of post-traumatic stress disorder, and treatment-seeking for post-traumatic stress disorder in the United States. Psychol Med 41:71–83
- Russell E, Koren G, Rieder M, Van Uum S. (2012). Hair cortisol as a biological marker of chronic stress: current status, future directions and unanswered questions. Psychoneuroendocrinology 37:589–601
- Shea AK, Streiner DL, Fleming A, Kamath MV, Broad K, Steiner M. (2007). The effect of depression, anxiety and early life trauma on the cortisol awakening response during pregnancy: preliminary results. Psychoneuroendocrinology 32:1013–20
- Small ML. (2007). Racial differences in networks: do neighborhood conditions matter? Social Sci Quart 88:320–43
- Stalder T, Kirschbaum C, Alexander N, Bornstein SR, Gao W, Miller R, Stark S, et al. (2013). Cortisol in hair and the metabolic syndrome. J Clin Endocrinol Metab 98:2573–80
- Staufenbiel SM, Penninx BW, Spijker AT, Elzinga BM, van Rossum EF. (2013). Hair cortisol, stress exposure, and mental health in humans: a systematic review. Psychoneuroendocrinology 38:1220–35
- Steudte S, Kirschbaum C, Gao W, Alexander N, Schonfeld S, Hoyer J, Stalder T. (2013). Hair cortisol as a biomarker of traumatization in healthy individuals and posttraumatic stress disorder patients. Biol Psychiatry 74:639–46
- Suglia SF, Staudenmayer J, Cohen S, Enlow MB, Rich-Edwards JW, Wright RJ. (2010). Cumulative stress and cortisol disruption among Black and Hispanic pregnant women in an urban cohort. Psychol Trauma 2:326–34
- Tosevski DL, Milovancevic MP. (2006). Stressful life events and physical health. Curr Opin Psychiatry 19:184–9
- Tse AC, Rich-Edwards JW, Koenen K, Wright RJ. (2012). Cumulative stress and maternal prenatal corticotropin-releasing hormone in an urban U.S. cohort. Psychoneuroendocrinology 37:970–9
- Wadhwa PD. (2005). Psychoneuroendocrine processes in human pregnancy influence fetal development and health. Psychoneuroendocrinology 30:724–43
- Weathers FW, Huska JA, Keane TM. (1991). PCL-C for DSM-IV. Boston: National Center for PTSD-Behavioral Science Division
- Weathers FW, Keane TM, Davidson JR. (2001). Clinician-administered PTSD scale: a review of the first ten years of research. Depress Anxiety 13:132–56
- Weinstock M. (2005). The potential influence of maternal stress hormones on development and mental health of the offspring. Brain Behav Immun 19:296–308
- Wennig R. (2000). Potential problems with the interpretation of hair analysis results. Forensic Sci Int 107:5–12
- Wilkins KC, Lang AJ, Norman SB. (2011). Synthesis of the psychometric properties of the PTSD checklist (PCL) military, civilian, and specific versions. Depress Anxiety 28:596–606
- Wolfe J, Kimerling R. (1997). Gender issues in the assessment of posttraumatic stress disorder. In: Wilson JP, Keane TM, editors. Assessing psychological trauma and PTSD. New York: Guildford. p 192–238
- Wosu AC, Valdimarsdottir U, Shields AE, Williams DR, Williams MA. (2013). Correlates of cortisol in human hair: implications for epidemiologic studies on health effects of chronic stress. Ann Epidemiol 23:797–811.e2
- Wright RJ, Fisher K, Chiu YH, Wright RO, Fein R, Cohen S, Coull BA. (2013). Disrupted prenatal maternal cortisol, maternal obesity, and childhood wheeze. Insights into prenatal programming. Am J Respir Crit Care Med 187:1186–93