Abstract
Objective: This paper describes the current level of development of robots for surgery.
Material and Methods: This paper is based on a literature search in Pubmed, IEEExplore, CiteSeer and the abstract volumes of the MICCAI 2002, 2003 and 2004, CARS 2003 and 2004, CAOS 2003 and 2004, CURAC 2003 and 2004 and MRNV 2004 meetings.
Results: Divided into different disciplines (imaging, abdominal and thoracic surgery, ENT, OMS, neurosurgery, orthopaedic surgery, radiosurgery, trauma surgery, urology), 159 robot systems are introduced. Their functionality, deployment, origin and mechanical set-up are described. Additional contacts and internet links are listed.
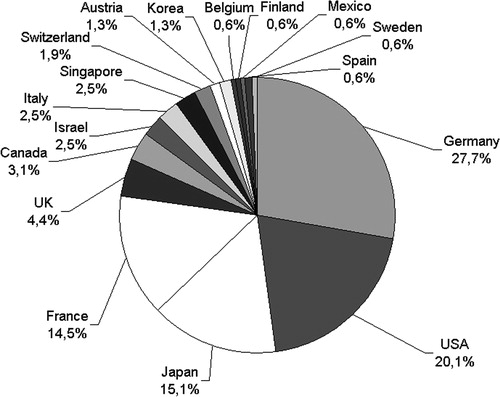
Conclusions: The systems perform diverse tasks such as milling cavities in bone, harvesting skin, screwing pedicles or irradiating tumors. From a technical perspective the strong specialization of the systems stands out. Most of the systems are being developed in Germany, the United States, Japan or France.
Introduction
Computer-aided surgery is in a state of continuous development Citation[1–5]. Research is being done at university research facilities as well as on the part of commercial entities. Recent developments enable single procedures in trauma surgery and urology besides the established applications in neurosurgery, orthopaedics, cardiac and abdominal surgery. Some can be used in MRI, while others are small enough to be hand-held. Industrial robots are being adopted or special robot kinematics with specific mechanical structures are being developed.
The current state of the development of robot-aided surgery, especially of mechanical components, is summarized here, and the individual systems are introduced. They are assigned to specific medical disciplines: imaging, abdominal and thoracic surgery, ENT, OMS, neurosurgery, orthopaedics, radiosurgery, trauma surgery, or urology, according to their field of deployment.
A descriptive statistical evaluation of features, such as clinical readiness for use, kinematics employed, origin (nationality) and degrees of freedom (DOF), is presented.
This work focuses on technicians conducting research and development in the field of computer- and robot-aided surgery, as well as on the interested physician who will find himself in closer contact with this technology in the future. The technician will be able to position his projects within an international context, where the physician will get an overview of existing systems and their clinical readiness for use.
Material and methods
A search of the literature databases Pubmed, IEEExplore and CiteSeer has been carried out; the link lists of institutes working in the field of robot-aided surgery have been sifted through; and finally, a general internet search has been carried out. Additionally, the abstract volumes of the conferences MICCAI 2002, 2003 and 2004, CARS 2003 and 2004, CAOS 2003 and 2004, CURAC 2003 and 2004 and MRNV 2004 have been sifted through. In this context, special emphasis has been placed on developments in the past 4 years.
All systems providing an automated or remote movement of a tool have been included in this inquiry. Motorized platforms for surgical microscopes are excluded as, for example, they do not manipulate tissue.
The evaluation of the gathered data was carried out using Microsoft Excel 2000®.
The citing of systems and projects is sorted according to the earlier mentioned disciplines, and within these in alphabetical order. Citations of unknown project names are placed at the end of sections. Unknown project names are replaced by a code composed of letters corresponding to the country of origin and consecutive numbers.
Results
The results are compiled in .
Table I. Overview of the robotic systems.
Imaging
The CLEM systemFootnote1 (Compact Laparoscopic Endoscope Manipulator) is used to guide an endoscopic camera in three DOF. Pneumatic muscles are used as actuators. The system is controlled by a keypad or via voice control and a foot switch Citation[10]. Pre-clinical results have been reported Citation[9].
The project COPRINFootnote2 deals with the control of a miniature endoscopic camera. Parallel kinematics with three DOF are used. The construction measures ∼8 mm in diameter, is 25 mm long and can carry 500 g of axial weight. Information on clinical use is not available.
The robot CROBOTFootnote3 (ENDOCRAWLER) uses special serpentine kinematics to move an endoscope through the patient's intestines. To do this, specific elements of the construction change their diameter and distance. No clinical experience has been obtained so far.
The EDR systemFootnote4 is used for telesonography purposes and uses three-DOF hybrid kinematics (‘Pantograph’) Citation[11]. The sonode is moved by remote control over the abdomen of the patient. Additionally, the system provides a real-time video-conference system. Experimental results are available Citation[12].
The robot EMILFootnote5 (Endoscopic Microcapsule Locomotion) is used for examination of the gastrointestinal tract. Its purpose is to transport an endoscopic microcapsule.Footnote6 The device moves in a snake-like manner by alternately changing the diameter of its segments and the distance between these segments. In vivo tests on pigs have been reported Citation[13].
ENDOASSIST®Footnote7 is a commercially available system for automatically controlling the camera during endoscopic operations. The system is based on a five-axis SCARA arm and can be used clinically. The company also introduced the system ENDOSISTA, which cannot yet be purchased.
The FIPSFootnote8 system provides remote-controlled imaging for endoscopic operations. A three-axis kinematics device is attached to the OR table and moves an endoscope around the entry point. It is controlled with a joystick by the surgeon. The system is licensed by the Storz Company, Tuttlingen, Germany. Information on clinical use is not available.
The system GABIEFootnote9 (Guidage Actif Basé sur l'Imagerie Echographique) is used for endoscopic telesonography. A sonode is attached to a surgical tool. No information on kinematics or use is available, and clinical experience is not yet reported.
The system HIPPOCRATEFootnote10 provides automated user-independent ultrasonic imaging and can also be used for telesurgery Citation[16]. The sonode is moved over pre-defined parts of the patient with constant velocity. The kinematics of HIPPOCRATE are based on special serial kinematics with six DOF. The development, which is not commercially available, is being driven by several European institutions and companiesFootnote11.
HYPER-ENDOSCOPEFootnote12 is a prototype of an active-serpentine endoscope. It can be used as a remote-controlled surgical system and moves through the intestines by changing the diameter and distance of the single segments. Other projects concern microsurgical instruments and force feedback for virtual endoscopy.
The LAPARO-NAVIGATORFootnote13 (or NAVIOT) system uses two-DOF parallel kinematics to automatically control an endoscope. The drive is positioned beside the patient and a lever gear moves the endoscope. Clinical experiences have been reported Citation[17].
The LERFootnote14 provides automatic imaging for endoscopic surgery. To do this, a ring is positioned on the abdominal wall using straps, an articulated arm or suturing. A camera unit can be rotated and tilted via a cross arm. Additionally, the objective can be moved back and forth in the trocar so that three DOF can be gained. The velocity of the moving parts is limited to 20°/s and 20 mm/s. It takes ∼30 s to remove the system from the patient Citation[18]. Control is performed via a keypad or voice control. Experiments on pigs have been performed.
The system MINOP2Footnote15 has been developed by a consortium of several institutes and enterprises. Within the scope of this project, an exoscope for neurological applications has been set up. This system comprises a five-DOF articulated arm, which carries a stereo camera and a set of lenses, and 3D-vision goggles to be worn by the surgeon. Thus, the usual disadvantages of a surgical microscope should be avoided Citation[19]. No information on clinical experience is available.
The MUSYCFootnote16 project deals with the development of a robot for coloscopy Citation[20]. The device travels in a snake-like manner through the intestines by segmentally ingesting the abdominal wall. It is propelled by pneumatic actuators in an inchworm-like way. The robot can be used for imaging and biopsy. Results are available from in vitro trials Citation[21].
The system OTELOFootnote17 provides automated user- independent ultrasonic imaging and can also be used for telesurgery Citation[16]. The sonode is moved over pre-defined parts of the patient with constant velocity. The kinematics of OTELO comprise a set-up that is directly placed on the patient. The system is not commercially available. Development has been undertaken by several European institutions and companies.Footnote18
The system PAROMISFootnote19 is used for robotic endoscopic camera guidance. It is based on hexapod kinematics and can be attached to the OR table. The system weighs ∼4 kg. It is controlled by speech or a touch screen. Force–torque sensing is implemented Citation[22]. Information on clinical experiences is not available.
The TERFootnote20 system is used for telesonography Citation[23]. A frame is attached to the patient using straps. On this frame, a sonode can be remotely rotated and tilted. Information on clinical experiences is not available.
ULTRASOUND ROBOT, a robot for telesonography, is under development in Stockholm.Footnote21 This six-DOF articulated arm robot is mounted on a trolley and remotely controlled by the surgeon using a joystick. It carries a US-sonode and can also be controlled over long distances. Information on clinical experiences and disposability is not available.
A robot for remote-controlled ultrasonic imaging was introduced by Abolmaesumi and SalcudeanFootnote22 (project ‘CAN1’). This robot is based on parallelogram kinematics and guides an ultrasonic probe over the patient's skin in six DOF around an invariant point. The patient can move the robot aside by hand when necessary. The robot is controlled via a force-feedback joystick or a space mouse. There is information on clinical experiences available Citation[24], Citation[25].
A C-arm with robotic functions is under development in LübeckFootnote23 (project ‘DEU10’). This system features a C-arm with five DOF to provide isocentric movement in virtually any axis around a point. In addition, acquiring larger pictures by building a mosaic becomes possible. The system uses a smaller C-arm when compared with known isocentric C-arms Citation[26]. Information on clinical use is not available.
At the University of Malaga,Footnote24 a robot for endoscopic surgery is under development (project ‘SPA1’). This system comprises a self-made SCARA-type robotic arm mounted on a vertical rail to move an endoscopic camera within four DOF. Experiments on a patient simulator and animals have been reported Citation[27].
An active endoscopic system has been introduced by the group of BrudickFootnote25 (project ‘USA2’). This robot winds through the intestines Citation[28] and consists of a number of flexible combined segments which alternately enlarge their diameter and push on each other. There is room inside for an optical fibre to inspect the intestinal walls. Information on clinical experiences is not available.
Three robotic camera holders have been introduced by RentschlerFootnote26 et al. (project ‘USA5’). These robots are used to provide imaging during laparoscopic surgery. The first system is a small (15 mm diameter and ∼75 mm long) battery-powered camera fixed to the inner abdominal wall by a clamp. It uses LED lights to illuminate the region of interest. Camera data are submitted via a wireless connection. The second system uses the same camera, but provides pan and tilt movements (360°, ± 45°). Here, a cable is used to provide power to the motors and the camera. The third system uses two wheels to propel itself to the region of interest. Here also a cable is used. In vivo experiments have been performed on pigs Citation[29].
Abdominal and thoracic surgery
At the Department of Mechano-Informatics at the University of Tokyo,Footnote27 the ‘Active Trocar’ project is pushed ahead. This manipulator for endoscopic interventions is able to move the forceps in six DOF and is mounted on the OR table with a small passive arm. This master–slave system has been tested on a pig Citation[30].
The system AKTORMEDFootnote28 is a robot for master–slave applications in minimally invasive surgery Citation[31]. It uses a three-DOF articulated arm with an hydraulic actuator.Footnote29 The system is set up next to the OR table. Information on clinical experience is not available.
The telesurgical experimental set-up ARTEMISFootnote30 consists of a cockpit unit and several manipulator arms for endoscopic surgical steps and for imaging. Serial kinematics and specially developed joysticks for control by the surgeon are used Citation[32]. Clinical information is not available.
Surry et al. introduce BBAFootnote31 (Breast Biopsy Apparatus), a system for breast biopsy under ultrasonic control. A fusion of stereotactic mammography, freehand ultrasound and 3D-ultrasound is performed to define the region of interest. The system provides three DOF on a Cartesian stage. Experiences from animal trials have been reported Citation[33].
BLACK FALCON is a surgical robot for remote-controlled procedures.Footnote32 This self-made articulated arm provides four DOF to move a surgical tool Citation[34]. Information on clinical experiences is not available.
Within the BLUE DRAGONFootnote33 project, a system for the guidance of endoscopic instruments has been developed. It is based on parallelogram kinematics and provides four DOF. Owing to this set-up, movements around a pivot point are possible. One of the project aims is to measure forces and torques, which appear during surgery Citation[35]. Pre-clinical results are available Citation[36].
The B-ROB 1Footnote34 robot is used for radiologically controlled biopsy extraction Citation[37]. It is built around special seven-axis kinematics with a serial configuration. The slender set-up enables operations to be performed inside a CT scanner. Information on clinical experiences is not available.
Its predecessor, B-ROB2, is based on a modular approach using several two-DOF stages Citation[38]. In a first prototype, two of these stages were mounted in a parallel fashion, allowing control of entry point and direction of a biopsy needle. The stages were mounted on a passive arm and could be used in a CT scanner environment. An MRI-compatible set-up is under development. Information on clinical experience is not available.
CT-BOT is a robot for percutaneous interventions inside a CT scanner and was introduced by a group from Strasbourg.Footnote35 The system uses parallelogram kinematics and provides five DOF. It is built from radiolucent material, uses ultrasonic actuators, and carries a needle driver unit which provides two additional DOF Citation[39]. The system is mounted on the patient's abdomen with straps. It is remotely controlled via a six-DOF joystick which provides force feedback. There is no information on clinical experiences available.
The system D2M2 (Direct Drive Modular Manipulator) is under development for endoscopic surgery in Montpellier.Footnote36 It comprises a self-made SCARA-arm attached to a vertical guide. The arm itself carries an endoscopic tool which moves in six DOF for minimally invasive interventions. The robot is controlled by a master input device. Clinical experience has not been reported.
The systems DAVINCI® Footnote37 and ZEUS® or AESOP® Footnote38 from the recently merged companies Computer Motion and Intuitive Surgical, both from USA, may be purchased. These telesurgical workstations consist of a cockpit unit with joysticks, imaging elements and a manipulator unit whose three arms control the instruments and endoscopic camera Citation[6]. SCARA kinematics with six DOF (DAVINCI) and four DOF (ZEUS, AESOP) are used. These systems are used for laparoscopic surgery (visceral surgery, gynaecology and urology Citation[7]) and in the field of minimally invasive cardiac surgery Citation[8].
The system ENDOPARFootnote39 is a telemanipulator for laparoscopic interventions. This system uses three industrial PUMA robots to move the instruments (known from DaVinci) and to guide the endoscopic camera Citation[40]. The intention of the project is to automate several tasks such as suturing Citation[41]. The system has not yet been tested in a surgical environment.
The ENDOXIROBFootnote40 system has been developed for endoscopic operations. It features two arms to control the instruments and to align the endoscopic camera. This development has been driven by several French institutes and companies.Footnote41 For the first experiment, a six-axis industrial-articulated robot is used. Another prototype with parallelogram kinematics has been introduced Citation[42]. This set-up allows movements in three DOF around an invariant point. There is no information on clinical experiences available.
The Green Telepresence Surgery System (GTSS) was developed at the Stanford Research Institute.Footnote42 This telemanipulation system consists of a workstation with two joysticks and a stereo visualizing device and a robot with two articulated arms at the surgery site Citation[43]. In addition, acoustic information and force feedback are provided. This system was the predecessor of the DaVinci surgical system.Footnote43
The HYPERFINGERFootnote44 is a manipulator for microsurgical interventions. This master–slave system maneuvers the forceps in seven DOF using a small linkage system. The slave subsystem is set up on a tripod next to the OR table and is 10 mm in diameter. The system has been tested on a pig Citation[44].
The system IRASIS (Insertion Robotisée d'Aiguille sous Imagerie) is developed by the LSIIT within the ROBEA program.Footnote45 This robot is intended to insert a needle into a tumor in the liver under CT control. A self-made six-DOF articulated arm robot is used Citation[39]. The system is a successor to the project CT-BOT. Information on clinical experience is not available.
KIMRO is a robotic system for interventions in the MR scanner and has been introduced by Virtanen et al.Footnote46 This system uses a long arm made from plastics and titanium to move a needle or other surgical tools within the field of an MR scanner Citation[45] in five DOF. No information on surgical experiences is known.
The system LAPROTEKFootnote47 is used for remote-controlled laparoscopic surgery. It is commercially available (but not FDA approved). The system comprises a workstation with joysticks and visualization and a robotic device attached to the OR table Citation[46]. The instruments have a diameter of 7.5 mm and are disposable. Information on clinical experience has been reported Citation[47].
The LARSFootnote48 system was used experimentally for percutaneous renal access Citation[48] and for minimally invasive neurosurgical Citation[49] and laparoscopic Citation[50] interventions. In these procedures, the system was used to guide an endoscopic camera. Mechanically, the system is based on a serial articulated arm. No information on DOF is available. On the basis of LARS, several other robotic systems have been developed (see PAKY, ACUBOT and Steady-Hand Robot).
The LPRFootnote49 (Light Puncture Robot) is a system for use inside the MR scanner. The device provides five DOF and is set directly onto the patient's abdomen. The systems LER and TER use straps for fixation; here, these straps are actuated by pneumatic motors to move the device. The robot weighs 1 kg and is made from plastic material Citation[51]. Information on clinical experience is not available.
The project MARGEFootnote50 deals with robotics for microsurgical applications Citation[52], Citation[53]. The robot is programmed to automatically restrict its movements according to the area of the body in which it moves. In addition, common tasks like suturing are pre-programmed. A Mitsubishi PA10 articulated arm robot is used. Information on clinical experience is not available.
The system MCFootnote2E (Manipulateur Compact de Chirurgie Endoscopique) is a joint projectFootnote51 for endoscopic surgery Citation[54], Citation[55]. The project is connected to the MARGE project and the ROBEA program. The system's base is mounted on the patient's stomach by belts or straps. The endoscopic tool is moved by a small robotic arm attached to the base. In vivo trials on pigs have been reported.
Within the MICRONFootnote52 project, a hand-held three-DOF manipulator to compensate for tremor during intra-ocular microsurgery has been developed Citation[56], Citation[57]. It consists of three-legged parallel kinematics with piezo drives and inertial or optic measuring systems Citation[172]. The range of movement is 0.5 mm and the maximum force is 0.05 N. There is no information on clinical experiences available.
The MICROSURGICAL ASSISTANTFootnote53 project (‘Steady-Hand Robot’) deals with robot technologies in microsurgical applications. The instrument is attached to a manipulator arm (serial, six DOF), which damps or stops certain undesirable movements such as hand tremor or departure from pre-defined trajectories Citation[58]. The system is based on the PAKY Citation[166], the LARS project. No information on clinical experiences is available. DewanFootnote54 et al. Citation[173] present an ophthalmologic application.
The MIRA manipulator systemFootnote55 can be used inside the MR scanner for minimally invasive interventions, e.g., on the spine. Thus, it is possible to remotely puncture vertebral bodies under near real-time imaging. The mechatronic components for the special four-axis serial kinematics are made from MR-compatible material. No clinical experiences are known to have been reported.
The system PADEMISFootnote56 (Peristaltically Actuated Device for Minimal Invasive Surgery) is under development for minimally invasive surgery. This worm-like structure has a diameter of 4 mm and comprises three groups of six segments which change diameter and length periodically to create peristaltic movement. Each segment consists of six chambers in a radial assembly. The direction of movement can be controlled by actuating each chamber differently. A flexible tube provides pressure to the silicone rubber segments and access to the tip of the device for endoscopic procedures Citation[59]. Clinical experience has not been reported.
The robot PADYCFootnote57 has been developed for applications in the field of pericardiac punctures. Via the robot arm, the movements of the surgeon are checked and, if needed, restricted if pre-defined trajectories or perimeters are exceeded Citation[60]. The system uses a three-axis SCARA robot with additional rotational and linear axis and contains six DOF altogether. Spatial orientation is provided by an optical tracking system. There is no information on clinical experiences available.
The RAMS (or AMES) surgical robot project is a miniaturized six-DOF telemanipulator with master and slave subsystems, programmable tools, force feedback and tactile feedback. This project is driven by NASAFootnote58 and an industrial partner Citation[61].Footnote59 Master and slave arms are ∼2.5 cm thick and 25 cm long and have six DOF each. The system has been deployed for testing purposes.
The ROBITOMFootnote60 manipulator system can be used in MR as well as in CT scanners for biopsy of breast tumors. The mechatronic components for the special three-axis kinematics are built from MR-compatible materials Citation[54]. There are no clinical experiences known so far.
A ROBOTIC LASER COAGULATOR was presented by SuzukiFootnote61 et al. Citation[63]. This device combines a video endoscope, a light source, a visible laser pointer and a coagulating laser diode in the forceps. This two-DOF system is 11 mm in diameter and 26.5 mm long and can be integrated into a telerobotics system. Clinical experiences have been carried out on a porcine liver.
The system TEC (Tethered Epicardial Crawler, project HEARTLANDER) is currently being developedFootnote62 for minimally invasive heart surgery Citation[64]. The device is inserted through a small incision and moves on the heart's surface. To do so, the device consists of two suction pads (13 mm in diameter, 13 mm high) connected to each other by 3 nitinol alloy wires Citation[65]. The length of these wires can be controlled by the surgeon via a joystick and a digitized fiberscope. In vivo trials on pigs have been reported.
The group of SastryFootnote63 is dealing with the development of telesurgical manipulators and interfaces. The objective is to realize force feedback as well as exact haptic feedback on endoscopic interventions Citation[66]. There are no clinical experiences known so far.
Within the TONATIUH project,Footnote64 a robot for telesurgical procedures is being developed. The group first collected experiences in robot-aided laparoscopic surgery using a PUMA 6000 robot. The TONATIUH-robot has four DOF and a maximum reach of 40 mm, a payload of 300 g and a weight of 18 kg. The system is remotely controlled by a joystick Citation[67]. Surgical experience has been reported on pigs and dogs Citation[68].
To place a needle in a tumor under ultrasonic control, the ATRE-LabFootnote65 has developed a manipulator called UMI Citation[174]. This special set-up, which consists of a sonode and a needle driver, is adducted to the skin by a PUMA robot Citation[69]. There are no clinical experiences known so far.
The system VECTORBOT is under development for positioningFootnote66 instrument such as needles, electrodes or drill guides. The system seems to be based on an articulated arm (DLR ‘Hand III’ 67). Further information is not available.
A robotic system for minimally invasive coronary artery bypass (CABG) surgery has been introduced by the group around Salcudean Citation[70] (project ‘CAN2’).Footnote68 The system is based on parallel kinematics and provides six DOF. It is supposed to move the instrument in synchrony with the heart's movements when performing surgery in such a way that the instrument virtually stands still. It is controlled by the surgeon via force-feedback joysticks. There is no information on clinical experiences available.
Research in the field of telesurgery and automated robotic camera-guidance systems for endoscopic surgery is being done at the German Aerospace Center.Footnote69 For example, one of the developed systems is intended to automatically keep the view of the camera on the instrument or virtually ‘freeze’ the heart's movements by synchronizing the movement of the instrument with the heartbeat Citation[71]. Special articulated kinematics (project ‘DEU1’) are used.
The project NAVIPED deals with robotic aid for pedicle screwing Citation[138]. There are no clinical experiences known so far.
A robot system for needle placement under CT control is under development in ErlangenFootnote70 (project ‘DEU8’). This six-DOF industrial PUMA robot is implemented in a CT environment. Information on clinical experiences is not available.
A robot for the puncture of retinal vessels is under development in LübeckFootnote71 (project ‘DEU9’). This system comprises a six-DOF hexapod known from the EVOLUTION1 system. It is planned to use the system to insert a 22-gauge needle into the vessels of the retina. Heartbeat and other motions of the patient are to be compensated for Citation[73]. Information on clinical experience is not available.
A robot system for CT-guided interventions has been presented in StrasbourgFootnote72 (project ‘FRA3’). The system is composed of self-made five-DOF parallel kinematics for the positioning of a three-DOF needle driver Citation[39]. The parallel structure is made of two six-bar lever mechanisms. Force sensors for force feedback are implemented and a commercial force-feedback input device is used. All actuators are installed in such a way that they do not disturb the CT scanner. Information on clinical experience is not available.
At the Technion in Israel,Footnote73 a robot for the registration of bone surfaces is under development (project ‘ISR3’) (see RSPR3).
The Surgical Assist Technology GroupFootnote74 has developed a system to control instruments for surgery. It uses hexapod kinematics (six DOF) which can be deployed in an open MRI (project ‘JAP1’). Together with the Surgical Planning Laboratory,Footnote75 a system has been developed which serves to place radioactive seeds under MRI control and uses special serial kinematics with five DOF Citation[75], Citation[76] (see project ‘JAP7’). Clinical experiences are not known.
A robot for use in an open MRI has been developed in Tokyo.Footnote76 It enables minimally invasive liver biopsy, works via electro-hydraulic-driven kinematics and can be sterilized Citation[77] (project ‘JAP3’). There are no clinical experiences known so far.
A forceps manipulator for a couple of endoscopic procedures has been introduced by Suzuki Citation[175] (project ‘JAP16’).Footnote77 The system provides two microforceps (with four DOF each), a light source and an endoscopic camera in a single tube. For image overlay, a magnetic tracking sensor is also attached to the tube Citation[78]. The system is controlled by force-feedback joysticks to provide haptic control. The endoscopic tube is attached to a five-DOF robotic arm Citation[79]. In vivo tests on pigs have been reported Citation[78].
A robot for telemanipulation and laparoscopic surgery has been presented by ShimachiFootnote78 et al. (project ‘JAP17’). The system is in an experimental state and provides movements for a forceps in four DOF. To achieve accurate force feedback for the operator, a special force-sensing trocar is used Citation[80]. Information on clinical experiences is not available.
DohiFootnote79 et al. presented a robot for MR-guided thermotherapy for liver tumors (project ‘JAP21’). The system uses a five-bar linkage mechanism to orient the needle in two DOF. A third DOF is provided by moving the set-up vertically. The device is made from aluminum and stainless steel and actuated by ultrasonic motors. It has a maximum height of 240 mm in the MR gantry Citation[81]. Information on clinical experiences is not available.
A robot system for breast biopsy under ultrasonic control is being developed at the CIMIL LaboratoryFootnote80 (project ‘SING1’). A SCARA-robot with a second forearm is used. The first forearm carries a needle driver and provides seven DOF. The second arm carries the ultrasonic probe and allows movements in four DOF. Using this set-up, the needle can always be held within the range of the ultrasonic probe. For navigation, internal encoders and an external optical tracking system are used Citation[82]. There is no information on clinical experiences available.
A study group at Philips Medical SystemsFootnote81 has developed a robot to be deployed in a CT scanner (project ‘USA3’). The system directs a needle and is controlled by CT data, whereas the needle is aligned automatically. Details of pre-clinical experiences are available Citation[83].
A system for telesurgery is under industrial developmentFootnote82 (project ‘USA7’). The device moves a surgical tool in six DOF and uses special hybrid kinematics: two compound rests are mounted in parallel fashion and guide a tool. This assembly rotates on a ring which is mounted on the OR table. The tool itself can rotate around its axis Citation[84]. Information on clinical experience is not available. The company is also involved in the RAMS surgical robot project.
A robot for CABG is under development at the Columbia UniversityFootnote83 (project ‘USA8’). This system is set up using parallel kinematics and moves the surgical tool in six DOF. The heart's surface is tracked optically and the robot is controlled in such a way that the beating heart virtually stands still when watched through the visualization device also attached to the robot. Information on clinical experiences has not been reported.
Oral- and maxillofacial surgery, ear, nose and throat surgery
The A73 systemFootnote84 has been developed for automated telesurgical interventions in the sphenoid sinus. It uses a common articulated robot with six DOF and can either work automatically or be remotely controlled using a six-axis joystick Citation[85]. It has been developed in collaboration with industrial partners.Footnote85 Details of pre-clinical experiences are available.
The Surgical Robotics LabFootnote86 has introduced several projects. ROBOPOINT is a small, sterilizable robot with special hybrid kinematics (four DOF) Citation[87]. Possible applications are the control of instruments, punctures or the milling of bones. The OTTO system (which is based on the SurgiScope® Footnote87 system) is attached to the ceiling over the OR table and is deployed in head surgery to implant aesthetic prostheses Citation[88]. It uses parallel kinematics with seven DOF. OTTO2 provides a seven-DOF articulated robot (adapted industrial robot) for instrument guidance. ROBODENT® has been developed for dentistry but is actually not a robotic device. Another system (project ‘DEU5’) is used for maxillofacial interventions in a CT scanner. This comprises a three-axis robotic milling device that is attached to the scanner. Some of the systems have been tested clinically. Another system for maxillofacial surgery is under development: NAVIGATED CONTROL is used for bone milling Citation[86]. A shaver is hand-held and guided by a navigation system. The software switches the shaver off when a pre-defined spatial area is left. By doing so, a cavity can be resected. Details of clinical experiences are not available.
Within the Collaborative Research Center 414, ‘Computer and Sensor Based Surgery’, 88 of the German Research Foundation (DFG), the Universities of Heidelberg and Karlsruhe, Germany, are working on several concepts for robot-aided cranio-maxillofacial surgery Citation[89]. The ROBACKA project Citation[90], Citation[91] is used for milling the skullcap. It uses a six-axis articulated robot which is able to autonomously follow certain trajectories and which can also be used for passive navigation.
The robot ROBIN for milling of the lateral skull base and implantation of hearing aids is being developed in TübingenFootnote89 and Stuttgart.Footnote90 It is based on hexapod kinematics and is also described as a combination of surgical robotics and navigation Citation[92]. To expand the workspace, the robot is attached to a bracket. Information on clinical experiences is not available.
The RONAFFootnote91 project deals with the milling of the lateral skull base. To do this, an industrial robot with six DOF has been programmed to mill a cavity for an implanted hearing aid without perforating the skullcap, either under ultrasonic control or via force-based local navigation Citation[93]. Information on clinical experiences is not available.
The SURGICOBOTFootnote92 is a system designed to supervise and restrict movements of the surgical tool. The tool is mounted freely on a small six-DOF robotic arm and is restricted to certain pre-programmed areas. If such a boundary is reached, the movement of the tool is stopped. Experiments on resin jaws have been performed Citation[94].
The system X1 is available for dental implant navigation.Footnote93 This passive hexapod is used to precisely manufacture drill guides. Strut lengths are provided by the control software and realized manually. An integrated mill is then used to cut the drill guide. The system is commercially available.
A system for robot-aided laryngoscopy is under development in LeipzigFootnote94 (project ‘DEU 11’). The purpose of this system is to register forces during surgery and to move to different view positions Citation[95]. Information on clinical experiences is not available.
A robot for surgery of the upper airway and the throat has been presented by Taylor et al.Footnote95 (project ‘USA9’). This system consists of three manipulator arms (4.2 mm diameter). These devices implement Distal Dexterity Units (DDU) which are composed of snake-like units and detachable parallel manipulation units. The units provide bending of up to 70° with a radius between 18 and 29 mm in every direction and forces up to 1 N Citation[96]. Therefore, movements of the forceps attached to the distal end of the set-up is possible in six DOF.
Neurosurgery
The system ALPHA has been introduced by a commercial entity.Footnote96 It is based on a parallel lever mechanism and provides five-DOF movements around a remote center of rotation for microsurgical procedures Citation[97]. It is remotely controlled by the surgeon using a joystick. The company has published pictures of surgical procedures performed with this system.
The system CRANIOFootnote97 has been developed for milling of the skull cup Citation[98]. Pre-operatively planned bone resections are performed. Within this project, individual implants are manufactured to fit exactly to the resection. The system uses a small hexapod set-up to move the milling device in six DOF (CRIGOS). Information on clinical experience is not available.
The EVOLUTION1® 98 system guides tools or endoscopes on hexapod kinematics and an additional linear axis, which provides further workspace. It is used for neurosurgical applications. The hexapod is attached to a boom. The system has been clinically deployed but is no longer in production.
The system IGORFootnote99 (Image Guided Operating Robot) Citation[99] serves for image date fusion, for surgical planning and for performing neurosurgical interventions. A six-DOF articulated arm is used. Information on clinical experiences is not available.
The MINERVAFootnote100 robot for neurosurgical applications works inside a CT scanner. The surgeon is oriented by the images provided by the scanner and controls the robot step by step. Simultaneously, the system checks the surgeon's actions to determine whether the momentarily desired trajectory might destroy vital structures Citation[100]. The robot consists of special serial kinematics with five DOF. The system has been clinically deployed for testing purposes.
The NEUROARMFootnote101 project deals with the development of an MR-compatible manipulator for remote surgery. The system uses three specially developed articulated arms with seven DOF and piezo-electric motors for manipulation and imaging Citation[101–103] and works in an MRI scanner. Information on clinical experiences is not available.
The NEUROBOTFootnote102 project of the ATRE Laboratory in Tokyo is a manipulator for microsurgery. Within a pipe of 10 mm diameter, two surgical forceps and a 3D endoscope, as well as tubes for irrigation and suction are contained. The forceps are remote-controlled by a joystick. Clinical experiences have been reported Citation[104], Citation[105].
The NEUROBOTFootnote103 of the CIMIL Laboratory in Singapore is used for the milling of bones in the skull base area. Mechanically, it consists of two units: a base (three DOF) which is positioned before the actual robot (hexapod, six DOF). The hexapod executes the milling process. Information on clinical experiences is not available.
The NEUROMATE® Footnote104 system of the US company ISS was originally developed by the French University of Grenoble and was sold by the IMMI company before this company was taken over by ISS. An articulated robot of six DOF is used to place and guide a tool in the skull area Citation[106]. The actual surgical task is performed by the surgeon. The robot is commercially available.
The PATHFINDER® 105 system moves tools according to a pre-operatively defined trajectory. On the basis of serial articulated kinematics, it works without a stereotactic frame and registers the patient autonomously. The system is commercially available. This company also introduced the NEUROSISTA system which is not available and no clinical experiences have been reported. It consists of two SCARA robots with five DOF each.
The robotic system WAMFootnote106 was developed for spinal interventions. It is based on a seven-DOF articulated arm developed for industrial applications.Footnote107 The system for surgical applications is restricted to four DOF. The instrument is attached to the robot which allows movements only under pre-defined constraints Citation[107]. Experiences from phantom trials have been reported.
Navab and LoserFootnote108 introduced a robotic system for percutaneous interventions (project ‘DEU4’). This systems provides a two-DOF needle driver on a passive articulated arm and can be used in CT scanners Citation[108]. Results of animal trials have been reported.
At the German Cancer Research Center,Footnote109 a robot for stereotactic interventions has been developed (project ‘DEU6’). The system consists of an adapted measuring arm intended for industrial application which has been motorized and is controlled by the surgeon via a joystick and a conventional stereotactic frame Citation[109]. Special software to compute the ideal position of the robot base and for visualization of the robot's movements for collision avoidance is also included Citation[110]. There is no information on clinical experiences available.
A system for robot-aided laser ablation in neurosurgery has been introduced by a commercial entityFootnote110 (project ‘DEU7’). The device is mounted on a standard stereotactic frame and guides a laser-beam in two DOF (in/out and rotation). Brain-tissue fragments are removed from the cavity by continuous irrigation and suction through the laser probe. Blood vessels are detected by a confocal laser-scanning microscope, which is integrated into the probe. An additional coagulating laser is included in the probe to close vessels. The tube used has a diameter of ∼5.5 mm Citation[111]. Clinical trials have been reported.
From the ATRE labFootnote111 of the University of Tokyo comes an MRI compatible robot (project ‘JAP7’). It uses special serial kinematics made from synthetic material with five DOF for needle insertion in stereotactic neurosurgery. It works in an open MRI Citation[112]. The group is collaborating with the CISST-group at Johns Hopkins University, Baltimore, MD, USA. The system is also used for urological applications Citation[113]. Information on clinical experiences is not available.
A telesurgical workstation with MR-compatible arms to move tools and for imaging purposes has been introduced by TajimaFootnote112 (project ‘JAP8’). The experimental set-up is radially placed around a vertical-field MRI and is remotely controlled by a six-DOF joystick. Two arms with serial kinematics of MR-compatible material are used Citation[114]. Information on clinical experiences is not available.
An MR-compatible brain retracter manipulator (project ‘JAP10’) has been introduced by Okamoto et al.Footnote113 Two-segmented tongues, each with 10 individually controllable pieces, push aside the brain tissue in order to create space for further manipulators. Each segment of the hydraulically controlled tongues monitors and regulates the pressure put on the brain tissue Citation[115]. Experiences on animal experiments have been reported.
A manipulator for use in open MRI has been introduced by Masamune et al.Footnote114 (project ‘JAP12’). The system is for use in stereotactic neurosurgery. The robot has five DOF and is able to move a needle towards the injection point. To do this, a pivotable bow is seated on a Cartesian x–y–z guide along which the needle-driver can be moved Citation[116]. Information on clinical experiences is not available.
At the AIST Institute,Footnote115 a manipulator for transnasal neurosurgery is being developed (project ‘JAP13’). This three-axis robot is based on serial parallelogram kinematics and is able to move a surgical tool in an open vertical field MRI scanner Citation[117]. There is no information available on clinical experiences.
A micromanipulator for neurosurgical applications was presented at the Nagoya UniversityFootnote116 (project ‘JAP14’). This device is composed of a master–slave system with seven DOF which can be used in small cavities. To obtain a good maneuverability, a guided tube is used. The set-up has a diameter of 3 mm. There is information available on experiences from an experiment on chicken Citation[118].
A master–slave system for microneurosurgery was presented by Asai et al.Footnote117 (project ‘JAP19’). This system consists of a master-console, providing three-DOF joysticks, visualization (microscope and endoscopic stereo camera) and some foot switches and a manipulator set-up with two arms (four DOF: three rotational, one translational). Forceps are attached to the arms. In vivo experiments on rats have been carried out Citation[119].
ShadmerFootnote118 et al. have presented a robot for functional MRI experiments (project ‘USA10’). This two-DOF system is able to apply forces on the hand of a test person. The device is pneumatically driven and made from plastic components.
Orthopaedics
The ACROBOT® 119 robot mills the implant bed for a unicondylary knee prosthesis Citation[120], Citation[121]. It is mechanically based on an articulated robot arm designed for industrial purposes (six DOF). The end effector is controlled by the surgeon and allows only certain, pre-defined trajectories. The system is commercially available.
The ACUBOTFootnote120 system (see also PAKYFootnote121) is used for the robot-aided insertion of a needle for percutaneous vertebroplasty Citation[122].Footnote122 It is based on special active serial kinematics (‘RCM’, three DOF) on passive carrier arm (three DOF). This arm is attached to a Cartesian stage with three DOF and places a needle under CT or fluoroscopic control according to a pre-defined plan. This robot is also used for urological procedures (discussed later). Information on clinical experiences is not available.
The ARTHROBOTFootnote123 robot is used for the implantation of hip endoprostheses Citation[123]. It is based on parallel kinematics with four DOF and is attached directly to the bone. A mechanical registration procedure is used. There are no reports of clinical experiences. The same groupFootnote124 is working on several other medical robotics projects. These are remote-controlled manipulators and the appropriate interfaces.Footnote125 Information on clinical experiences is not available.
A system for orthopaedic use (knee arthroplasty) has been presented by Dombre et al.Footnote126 The system BRIGIT (Bone Resection Instrument Guidance by Interactive Telemanipulator) is under development in collaboration with an industrial partner.Footnote127 An industrial six-DOF articulated arm robot was adapted Citation[124] and mounted on a trolley together with the control cabinet. For surgery, the trolley is attached to the OR table. Information on clinical experience is not available.
The CASPARFootnote128 system uses an articulated industrial robot with six DOF for hip and knee endoprostheses, as well as for cruciate ligament replacement. The system was commercially available and has been used clinically, but the production has now stopped.
The Helmholtz Institute for Biomedical Technologies in Aix-la-ChapelleFootnote129 is working on the robotic system for bone treatment called CRIGOS.Footnote130 The system is technically based on parallel kinematics with six DOF. For applications, see CRANIO, MINARO and MINOP2.
The PI GALILEO NAVFootnote131 system uses two perpendicular linear axis to navigate and to automatically move the saw block to prepare the implant bed for knee replacement Citation[125]. For navigation purposes, the system uses an optical tracking system. The device is commercially available.
The GP-System is a motorized saw-blade guide for knee arthroplasty.Footnote132 The system automatically moves the saw block in two DOF and can be used with any prosthesis system. No pre-operative CT scan is necessary for planning. There is no information available on clinical use.
The BMGOFootnote133 work group is dealing with the milling of implant beds for knee replacement. The project IMAGE REGISTRATION uses a six-DOF industrial robot which carries a mill and a camera to track the bone surface. The bone is not clamped, but its movements are tracked by a special imaging system.Footnote134 Details of clinical experiences are not available.
The ITD system (Intelligent Tool Drive)Footnote135 is a hand-held six-DOF manipulator for the machining of bones Citation[126], Citation[127]. This device compensates for unintentional movements of the surgeon (e.g., tremor) and a tool is stabilized with respect ro the bone. The spatial alignment of the device and the bone is tracked by a special optical tracking system Citation[128].Footnote136 The first prototype is based on parallel kinematics (hexapod) with electrical linear motors; another set-up, which may become possible in the future, is based on epicyclic hybrid kinematics Citation[129]. The system has not been deployed clinically so far.
The robot LUKE is under industrialFootnote137 development for pedicle screw placement. This articulated arm robot provides six DOF to move the surgical tools. Information on clinical experiences is not available.
The MARSFootnote138 system is a carrier system for the positioning of a drill for spinal surgery. The miniaturized hexapod kinematics with six DOF carry a drill sleeve and are attached to the vertebral body via a clamp. After an automated powered alignment of the tool platform via fluoroscopic images, the drilling process can be carried out by the surgeon Citation[130], Citation[131]. Information on experiences from animal experiments is available. This procedure can also be used for long bone intra-medullary distal locking Citation[132] and has been developed in collaboration with an industrial partnerFootnote139 for commercialization under the name SpineAssist.
The system MIASFootnote140 is under development for minimally invasive arthroscopy Citation[133–135]. This hand-held system features a remote-controlled tip with one DOF (bending) for moving a small endoscopic tool. The arthroscope is a cylinder with an outer diameter of 4 mm and 350 mm total length. The 25 mm distal section of the arthroscope is dirigible (bending range 0–110°). The system also comprises a special navigation system. Information on clinical experiences is not available.
Within the MINAROFootnote141 project, robotic devices for bone-cement removal during revision hip surgery Citation[136] are under development. One system (MINARO1) is based on a hexapod known from the CRIGOS project. The robot is mounted next to the OR table. Another set-up (MINARO2) is based on small bone-mounted four-DOF kinematics Citation[176]. Details of clinical experiences are not available.
The system MODICASFootnote142 orients an implantation tool for hip prostheses towards the patient with a small six-DOF articulated robot. An optical tracking system is used Citation[137]. A pre-operative planning based on CT data is performed. The steps of the work on the bone are carried out by the surgeon. The system has been tested clinically.
The project NAVIPEDFootnote143 deals with robotic aid for pedicle screwing Citation[138]. An articulated arm robot is used. Information on kinematics and clinical experiences is not available.
The ORTHOSISTA® Footnote144 system serves as a carrier for a drill sleeve for orthopaedic applications. On the basis of two orthogonal intra-operatively acquired radiographs, the trajectory of, e.g., a screw, can be determined. The robot aligns the sleeve accordingly. The system is based on special hybrid kinematics with four DOF. The producer has reported clinical experiences.
The MRCASFootnote145 group is working on a system for precision freehand sculpting of bone, PFS. A hand-held nibbling-device is held against the bone and is switched on automatically when located in a pre-defined area so that only the planned bone surface remains Citation[139]. Clinical experiences with the system have not been reported so far.
The system PRAXITELESFootnote146 is under development for knee surgery. This bone-mounted robot is able to orient a cutting block for image-free knee arthroplasty Citation[140]. The system consists of a subsystem to manually adjust the position of the implant according to the planning performed with a navigation system, and a two-DOF robotic device which automatically adjusts the alignment of the implant to the anatomical axis. Experiences with cadaver trials have been reported.
The system RAO ASSISTANT MANIPULATOR has been designed by Yanagihara et al.Footnote147 to assist the surgeon during rotational acetabular osteotomy on the hip. This system uses a three-segmented tongue to retract the muscle tissue from the bone to allow minimally invasive procedures Citation[141]. The tongue is force-controlled and moved to the operation site by a six-DOF articulated manipulator. Details of clinical experience are not known but tests on pigs have been performed.
The ROBODOC®Footnote148 system is the best-known system for robot-aided surgery and is used for the milling of cavities in the femur for hip prosthesis purposes Citation[142], Citation[143]. It uses an industrial SCARA-robot with five DOF. The system is commercially available and has been applied over 10,000 times. Several work groups Citation[144], Citation[145] are dealing with related problems and use ROBODOC. In the meantime, the pins formerly required to perform the procedure have been replaced by a surface-matching procedure. The planning of the surgery is done before the operation on a proprietary planning station named ORTHODOC®.
For determination of the patient's alignment during robot-aided hip surgery, the ROBONAVFootnote149 project uses an optical tracking system along with the surgical robot ROBODOC® in such a way that the bone structure is recognized optically and undesirable movement of the patient is detected Citation[146]. Details of clinical experiences has been reported Citation[147].
The robot of the VISAROMEDFootnote150 project is used for pedicle screwing. An industrial hexapod with a horizontally and vertically adjustable carrier arm is used. The robot moves the drill with six DOF along the spinal column of the patient. There is no information available on clinical experiences with this robot. This work group also works in other fields of computer aided surgery Citation[148], Citation[149].
The robot RSPR3 has been developed in Israel.Footnote151 This parallel-kinematics-based platform is used for several medical applications. One project deals with knee arthroscopyFootnote152 (project ‘ISR1’), another Citation[150] with the insertion of needles in soft tissueFootnote153 (project ‘ISR2’), and a thirdFootnote154 with the registration of bone surfaces Citation[74] (project ‘ISR3’). This robot consists of three identical kinematic chains. Each chain contains a lever rotating around a pivot perpendicular to the base platform and offset from the center of the base. At the other end of the lever, a linear actuator is attached by a ball-and-socket joint. The upper end of the linear actuator is connected to the moving platform by a fork joint Citation[177]. This set-up leads to only a small number of singularities. Information on clinical experiences is not available.
A robot for total knee replacement has been introduced by Marcacci et al.Footnote155 (project ‘ITA1’). This system uses a custom-built five-DOF articulated robot which positions a plane guide. This guide is used by the surgeon to move the mill by hand Citation[151]. Results from trials on phantoms and biological specimens have been reported.
At the Advanced Therapeutic Engineering Laboratory,Footnote156 systems for orthopaedic surgery have been developed. One system uses z-like kinematics, manufactured from MR-compatible material (project ‘JAP6’) Citation[152]. Another system uses a simple set-up with two DOF for spinal surgery (project ‘JAP11’). Information on clinical experience is not available.
A robot for total knee arthroplasty was presented by SugitaFootnote157 et al. (project ‘JAP20’). This self-made articulated arm robot provides six-DOF motion for the milling tool. The special configuration of the axis leads to improved safety of the surgical process Citation[153]. The robot itself is 810 × 1500 × 2050 mmFootnote3 in size and weighs 900 kg. Information on clinical experience is not available.
A robot for percutaneous spine surgery has been developed at CISSFootnote158 in Korea (project ‘KOR1’). The system is ceiling-mounted and uses a self-made articulated arm to guide the tool Citation[154]. The system is remotely controlled using a workstation and joysticks. Information on clinical experience is not available.
Radiotherapy
The CYBERKNIFE® Footnote159 is an articulated arm robot maneuvering a linear accelerator. The patient is attached to the operating table via a flexible mask, and the linear accelerator is aimed at the tissue to be treated. An X-ray tracking system monitors the patient periodically for the position of the tumor throughout the treatment Citation[155]. The system is commercially available.
The system HEXAPOD is a six-DOF robotic radiation treatment couch.Footnote160 Providing six DOF, the patient can be placed in any alignment relative to the radiation source. Movements of ± 30 mm in the x- and y-axis and ± 40 mm in the z-axis, as well as rotations of ± 3° are possible. Information on clinical experience is not available.
Robotic applications for radiotherapy (the MOCOMP project) have been developed in MunichFootnote161 and Lübeck.Footnote162 Here, the spatial alignment and movement of the patient are tracked by an optical tracking system. On the basis of this data, the location of the tumor is calculated and a linear accelerator is aimed at it by a six-DOF articulated robot Citation[156]. Information on clinical experiences is not available.
At the Institute of Nuclear PhysicsFootnote163 in co-operation with the Centre Protonthérapie d'Orsay,Footnote164 a robot for tumor irradiation is developed (project ‘FRA1’). A special software called CARABEAMER is used. This robot maneuvers the patient in a proton beam around an isocenter. An articulated robot designed for industrial applications is used Citation[157]. There is no information available on clinical experiences.
Trauma surgery
The system BLOODHOUNDFootnote165 is a mobile medical robot for battlefield deployment Citation[158]. It moves on four crawlers and has an articulated arm to provide examination, drug delivery and bandages to casualties. It is supposed to move autonomously (guided by GPS) to the site and medical action is then remotely controlled by a surgeon. Information on its use by armed forces is not available.
The system DERMAROBFootnote166 (predecessor SCALPPFootnote167) actively moves a dermatome to achieve skin transplants for the treatment of burned skin Citation[159], Citation[160]. The dermatome is attached to an articulated arm robot (SCALPP) and a SCARA robot (DERMAROB) and is automatically moved with constant velocity and pressure over the skin of the patient. Information on animal experiments reported.
The system INTELLIGENT FIXATORFootnote168 comprises an external fixator which is set up with parallel kinematic structure. Each strut is actuated by a linear spindle, and strut forces are measured. The system can be used for bone repositioning as well as for deformity treatment Citation[161], Citation[162]. Clinical experience has been reported.
The REPOROBOFootnote169 project deals with the robot-aided repositioning of long bones. A six-axis industrial articulated robot is used. One bone fragment is attached to the robot and maneuvered under fluoroscopic control to fit the other fragment. Information on clinical experiences is not available.
At The Institute for Robotics and Process Control,Footnote170 a robot system for the reposition of bone fragments has been developed. A six-axis industrial articulated robot (Stäubli) is attached to the OP table and joins the bone fragments (project ‘DEU3’) Citation[164], Citation[165]. Clinical experiences have not been reported so far.
Urology
The ACUBOTFootnote171 system (PAKY, RCM robot) is used for the robot-aided insertion of a biopsy needle into the kidney. It uses special kinematics (‘RCM’, three DOF) on a passive carrier arm (three DOF) and places the needle as planned before surgery Citation[166]. The needle itself is then driven by the PAKY unit under fluoroscopic control.
The PROBOTFootnote172 is used for automated prostate resection. A boom is used to carry special circular kinematics. These in turn carry a semicircular handle on which a carriage is moved along. The tool is attached to this carriage and can move back and forth so three DOF are achieved Citation[167]. Clinical experiences have been reported.
The UROBOTFootnote173 project deals with several set-ups for urological treatments: prostate resection, implantation of radioactive seeds, and urethral surgery, among others. Special kinematics are attached to a conventional six-axis articulated arm robot. The project is based on the SARPFootnote174 project. The commercial prototype is called SABOT. Clinical experiences have been reported from the prostate resection field.
A TRUS (transrectal ultrasound) guided robotic system (project ‘CAN3’) has been developed by Fenster et al.Footnote175 It is designed to be used for brachytherapy of the prostate. The system consists of a six-DOF robot, a 3D TRUS imaging system Citation[168] and a needle rotation assembly mounted at the end of the robot arm Citation[169]. There is no information available on clinical experiments.
At the Engineering Research Center,176 a manipulator for transrectal prostate biopsy is being developed (project ‘USA4’). This system can be used in an MRI scanner. The biopsy needle is driven by special three-DOF kinematics in serial configuration which steer the needle through the rectum to a user-defined point Citation[170]. The system has been tested on a dog Citation[171]. The group is collaborating with the ATRE Laboratory in Tokyo.
Synopsis
We were able to identify 159 systems or projects (, ).
Figure 1. Summary of robots for different disciplines. ENT: ear nose throat surgery; OMS: oral- and maxillofacial surgery.
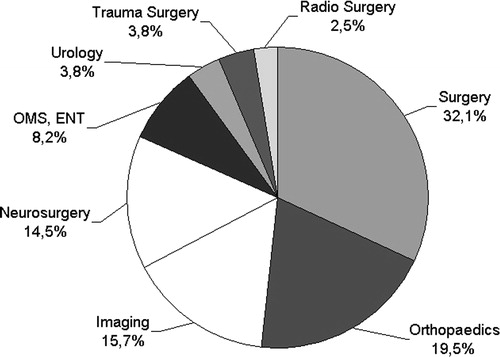
Table II. One hundred and fifty-nine robotic systems for medical applications in different disciplines.
Fifty-five percent of the systems originate from Europe, 23% from North America and ∼22% from Asia. The detailed distribution is displayed in .
Figure 2. Distribution of development sites of robot-aided systems.
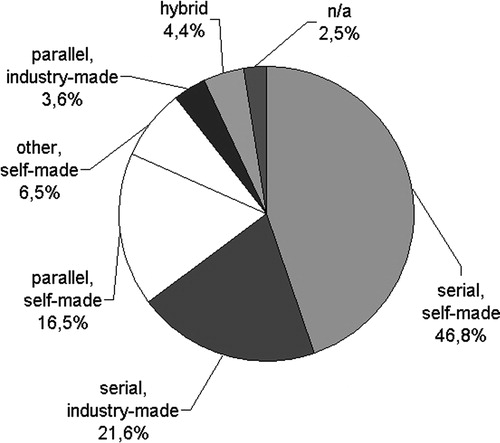
Most of the systems (68%) are based on serial kinematics with approximately one third using articulated robots (also known as PUMA or SCARA robots177) originally designed for industrial deployment. About 20% of the kinematics used are parallel kinematics from industrial production or have been specially developed for this purpose. A total of 70% of the robot systems were especially designed for medical use ().
Figure 3. Robot kinematics used.
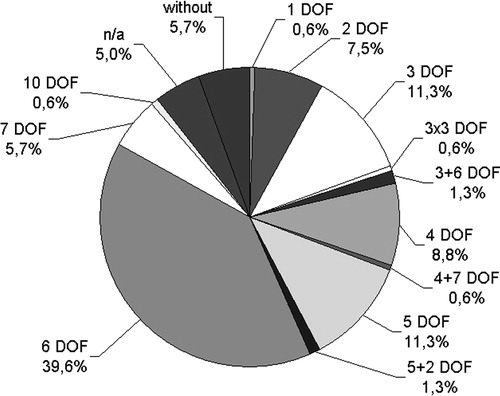
The number of DOF gives an impression of the complexity of the systems. The higher the number of DOF of a robot, the more flexible and also the more complicated it is. For complete mobility six or more DOF are required. Systems with fewer DOF are normally smaller in size and are specially adapted to their purpose. About 46% of the described systems have six or more DOF. About 42% of the systems have five or less DOF. For ∼6% of the systems giving the configuration of the DOF is not meaningful, e.g., in the serpentine set-up of an endoscope for coloscopies ().
Figure 4. DOF of the reviewed robot systems.
About 67% of the examined projects are at an experimental stage and have not yet been tested on patients. Twenty-four percent are used experimentally and 9% are commercially available in some countries.
Discussion
The present listing provides an outline of the worldwide state of the art in surgical robotics systems. The descriptions are limited to the basic facts and provide references for further study. Accurate assignment of systems, workgroups and medical fields is difficult due, in part, to the varying public relations of the institutes involved, especially in the Asian hemisphere. There are some systems which are used by two or more groups for different applications (e.g., ACUBOT/PAKY, CRIGOS/CRANIO/MINARO or project ‘JAP7’). However, the data collected in the presented study seems to allow the conclusion that most of the currently existing systems are presented.
Well-known reviews, such as those by Cleary and Nguyen Citation[1] or Taylor and Stoianovici Citation[2], provide a restricted survey of the state of the art concerning the number of systems described. Others are limited to certain fields Citation[4], Citation[5], Citation[178], Citation[179] or to particular technologies Citation[180], Citation[181].
Reflecting the presented data, the work on research and development in the field of medical robotics shows a wide extension of the technology. The systems have to fulfil several tasks, such as milling cavities in bone, harvesting skin, screwing pedicles or irradiating tumors, among others.
From the technical point of view, most systems are designed for only one dedicated application. A couple of systems are used for two or more applications, and other set-ups are used by some groups for different types of procedures. Systems which are designed for one application exclusively provide a smaller number of DOF and seem to be more compact. Alternatively, industrial robots are modified for the surgical working field (e.g., ROBODOC, CASPAR©). These robots are typically more effective and bigger than necessary for the surgical task, but their acquisition and handling are easier than using a self-made robot.
The big industrial robots of former systems were not always able to satisfy the user's expectations Citation[182]. It is assumed that, in the field of robot-aided surgery, future mechatronic devices will become smaller Citation[56], Citation[58] and easier to handle Citation[126], Citation[139]. Miniaturization can be achieved by differentiation according to applications, optimization of components and re-designing the kinematical set-ups.
In everyday life, surgeons only use a very small number of systems Citation[183]. This can be explained by the high complexity of use, the strict safety precautions, missing FDA clearances and the fact that many of the systems are developed in a university environment. In addition, all systems that were not clearly described as being in experimental use were considered to be experimental set-ups.
Basically, the objective of further research and development of medical robotics is the unification and simplification of procedures and the improvement of achieved outcomes. Whether this can be with the presented robotic systems must be evaluated by clinical trials.
Recent studies and the data presented here brought us to the conclusion that the acceptance of robotic devices has to be enhanced by the improvement of handling, e.g., by the miniaturization of the devices.
Acknowledgment
The work on project ITD is funded by the German Research Society under grants SCHA 952/1-1 and MA 1150/39-1.
Notes
1. Laboratoire TIMC, Grenoble, France; http://www-timc.imag.fr/.
2. Institut national de recherche en Informatique et en Automation, Le Chesnay, France; http://www-sop.inria.fr/coprin/index.html.
3. CIMIL Laboratory, Nanyang Technological University, Singapore; http://mrcas.mpe.ntu.edu.sg/research/crobot/index.htm.
4. Department of Medical Informatics, Ehime University Hospital, Japan; www.medinfo.m.ehime-u.ac.jp.
5. CRIM, Scuola St'Anna, Pisa, Italia; http://www-crim.sssup.it/research/projects/emil/default.htm.
6. Given Imaging, Israel; www.givenimaging.com.
7. Armstrong Healthcare Ltd., High Wycombe, UK; www.armstrong-healthcare.com.
8. Institut für Medizintechnik und Biophysik, Forschungszentrum Karlsruhe, Germany; http://hbksun17.fzk.de:8080/imb/de/home.html?med/systeme/fips.html∼top.main.
9. LIRMM (Montpellier), LRP (Paris), TIMC (Grenoble), CEA (Fontenay aux Roses), Groupe Hospitalier Pitié-Salpêtrière, CHU de Grenoble; www.lirmm.fr/∼w3rob/SiteWeb/detail_resultat.php?num_resultat = 33&num_topic = 1&num_projet = 1&num_activite = 1.
10. LIRMM, France; www.lirmm.fr/∼duchemin/Hippo.htm; Sinters SA, Toulouse, France; www.sinters.com.
11. OTELO Consortium: (1) Université d'Orleans, Laboratory of Vision & Robotics, France; www.bourges.univ-orleans.fr. (2) Sinters Group, Toulouse, France; www.sinters.fr. (3) Kell Company, Roma, Italy; www.kell.it. (4) Center for Research and Technology—Hellas (CERTH), Thessaloniki, Greece; www.eng.auth.gr. (5) Université de Tours, UMPS, Tours, France; www.med.univ-tours.fr. (6) Brunel University, Uxbridge, Great Britain; www.brunel.ac.uk. (7) Elsacom Company, Rome, Italy; www.elsacom.com. (8) Corporacio Sanitaria Clinic (CSC), Barcelona, Spain; www.clinic.eb.es. (9) Ebit Company, Geneva, Italy; www.ebit.it.
12. Biochemical Micro System Engineering Laboratory, Department of Micro System Engineering, School of Engineering, Nagoya University, Japan; www.bmse.mech.nagoya-u.ac.jp/index-e.html.
13. Bio-Medical Precision Engineering Laboratory, Institute of Environmental Studies, Graduate School of Frontier Sciences, University of Tokyo, Japan; http://bme.pe.u-tokyo.ac.jp/index_e.html.
14. Laboratoire TIMC, Grenoble, France; http://www-timc.imag.fr.
15. Aesculap AG, Tuttlingen, Germany; www.minop.de/.
16. ARTS Lab, Scuola Superiore Sant'Anna, Pisa, Italy; http://www-arts.sssup.it/research/projects.htm.
17. Laboratoire Vision and Robotique (LVR), Université d'Orléans, Bourges, France; www.bourges.univ-orleans.fr/otelo/site.html.
18. OTELO Consortium: (1) Université d'Orleans, Laboratory of Vision and Robotics, France; www.bourges.univ-orleans.fr. (2) Sinters Group, Toulouse, France; www.sinters.fr. (3) Kell Company, Roma, Italy; www.kell.it. (4) Center for Research and Technology—Hellas (CERTH), Thessaloniki, Greece; www.eng.auth.gr. (5) Université de Tours, UMPS, Tours, France; www.med.univ-tours.fr. (6) Brunel University, Uxbridge, Great Britain; www.brunel.ac.uk. (7) Elsacom Company, Rome, Italy; www.elsacom.com. (8) Corporacio Sanitaria Clinic (CSC), Barcelona, Spain; www.clinic.eb.es. (9) Ebit Company, Geneva, Italy; www.ebit.it.
19. Helmholtz-Institut für biomedizinische Technik der RWTH Aachen, Germany; www.hia.rwth-aachen.de/research/cht/paromis.html.
20. Laboratoire TIMC, Grenoble, France; http://www-timc.imag.fr.
21. Mobile Robotics SA, Stockhom, Sweden; www.mobile-robotics.com.
22. School of Computing and Department of Electrical and Computer Engineering, Queen's University, Kingston, Ontario, Canada; www.cs.queensu.ca/∼purang/projects. htmlty.
23. Institut für Robotik und Kognitive Systeme, Universita¨t Lübeck, Germany; www.rob.uni-luebeck.de.
24. Instituto de Automática y Robótica Avanzada de Andalucía, Universidad de Málaga, Severo Ochoa, 4. Parque Tecnológico de Andalucía, Málaga, Spain.
25. Department of Mechanical Engineering, California Institute of Technology, Pasadena, CA, USA; http://robotics.caltech.edu/∼jwb/medical.html.
26. Department of Surgery, University of Nebraska Medical Center, Omaha, NE, USA.
27. Department of Mechano-Informatics, The University of Tokyo, Japan; www.ynl.t.u-tokyo.ac.jp/index.html.
28. Arbeitsgruppe MITI, München, Germany; www.aktormed.com.
29. DELTA Engineering GmbH, Barbing, Germany; www.delta-engineering.info.
30. Institut für angewandte Informatik, Forschungszentrum Karlsruhe und Sektion Minimal Invasive Chirurgie, Universitätsklinik Tübingen, Germany; www.iai.fzk.de/medtech/medrob/artemis/welcome.html.
31. Robarts Research Institute, London, ON, Canada; www.imaging.robarts.ca/∼kath/.
32. Artificial Intelligence Lab, IT, Cambridge, MA, USA; www.ai.mit.edu/people/madhani.
33. Biorobotics Laboratory, University of Washington, Seattle, USA; http://brl.ee.washington.edu/Research_Active/Surgery/Device_BlueDRAGON/BlueDRAGON.html.
34. Austrian Research Centers, Seibersdorf, Austria; www.arcs.ac.at.
35. l'Equipe AVR; LSIIT, Université Louis Pasteur, Illkirch, France; http://hp2gra.u-strasbg.fr/.
36. LIRMM, Département Robotique, Montpellier, France; www.lirmm.fr/∼duchemin/D2M2.htm.
37. Intuitive Surgical, Sunnyvale, CA, USA; www.intuitivesurgical.com.
39. Lehrstuhl Informatik VI, TU München, Germany; http://atknoll1.informatik.tu-muenchen.de:8080/tum6/research/sfb453C7.
40. www.endoxirob.com.
41. Sinters SA, www.sinters.fr; CHU Toulouse, France, www.chu-toulouse.fr; LAAS, www.laas.fr; CEA-CEREM, www-dta.cea.fr/home_cerem.htm; INRIA, www.inria.fr/chir; IET, www.chu-toulouse.fr; ONERA, www.cert.ft; LIRMM, www.lirmm.fr/∼michelin/.
42. Stanford Research Institute, www.sri.com.
44. Department of Micro System Engineering, Nagoya University, Japan; www.mech.nagoya-u.ac.jp.
45. LSIIT, Illkirch, France; http://hp2gra.u-strasbg.fr/fr/research/med_rob/sauver.html.
46. Department of Mechanical Engineering, Oulu University, Oulu, Finnland; http://konekilta.oulu.fi/kimro/.
47. endoVia Medical (former Brock-Rogers Surgical), 150 Kerry Place, Norwood (MA), USA; http://endovia.millersystems.com.
48. CISST, Johns Hopkins University, Baltimore, MD, USA; www.cisst.org.
49. Laboratoire TIMC-IMAG, La Tronche, France; http://www-timc.imag.fr/.
50. LIRMM (Montpellier), LRP (Paris), CEA/SRSI (Fontenay-aux-Roses) and Pitié Salpêtrière hospital (Paris), in the framework of ROBEA (supported by the CNRS); www.lirmm.fr/∼michelin/.
51. Laboratoire Robotique de Paris (LRP), LIRMM, CEA; http://lrp6.robot.jussieu.fr/fra/personnel/morel/robotic_surgery.html.
52. The Robotics Institute, Carnegie Mellon University, Pittsburgh, PA, USA; www.ri.cmu.edu/projects/project_32.html.
53. CISST ERC, Johns Hopkins University, Baltimore, MD, USA; http://cisstweb.cs.jhu.edu/research/ microsurgicalassistant/.
54. Department of Computer Science, Johns Hopkins University, Baltimore, MD, USA.
55. Institut für Angewandte Informatik, Forschungszentrum Karlsruhe, Germany; www.iai.fzk.de.
56. Institute of Microsystems Technology, TU Ilmenau, Germany; www.maschinenbau.tu-ilmenau.de/pademis.
57. Laboratoire TIMC, Université de Grenoble, France; http://www-timc.imag.fr/olivier.schneider/perso/english/gb_rsp_main.html.
58. Jet Propulsion Laboratories, Pasadena, CA, USA; http://telerobotics.jpl.nasa.gov/tasks/rams/.
59. MicroDexterity Systems, Inc., Albuquerque, NM, USA; www.microdexsys.com.
60. Innomedic GmbH, Karlsruhe, Germany; www.innomedic.de.
61. Institute of Environmental Studies, University of Tokyo, Japan; http://bme.pe.u-tokyo.ac.jp/index_e.html.
62. The Robotics Institute, Carnegie Mellon University, Pittsburgh, PA, USA; www.ri.cmu.edu/projects/project_533.html.
63. University of California, Berkeley, CA, USA; http://robotics.eecs.berkeley.edu/medical/.
64. Dep. de Cirugía, Hosp. de Infectología, Centro Médico Nacional la Raza, IMSS.
65. Advanced Therapeutic and Rehabilitation Engineering Laboratory, University of Tokyo, Japan; www.atre.t.u-tokyo.ac.jp/projects/hong/index.html.
66. Brainlab AG, Heimstetten, Germany; www.brainlab.com.
67. German Aerospace Center, Oberpfaffenhofen; www.robotic.dlr.de.
68. School of Computing and Department of Electrical and Computer Engineering, Queen's University, Kingston, Ontario, Canada; www.ece.ubc.ca/∼tims/heart.html.
69. Deutsches Zentrum für Luft- und Raumfahrt, DLR, Wesseling; Germany; www.robotic.dlr.de.
70. Institute of Medical Physics, Erlangen, Germany; www.imp.uni-erlangen.de.
71. Institut für Robotik und Kognitive Systeme, Universita¨t Lübeck, Germany; www.rob.uni-luebeck.de.
72. LSIIT (UMR CNRS-ULP 7005), Université Louis Pasteur, Strasbourg, France; http://hp2gra.u-strasbg.fr/.
73. Technion, Haifa, Israel; http://robotics.technion.ac.il.
74. Surgical Assist Technology Group, Tsukuba, Ibaraki, Japan; http://unit.aist.go.jp/humanbiomed/surgical/.
75. Brigham and Women's Hospital, Boston, MA, USA; http://splweb.bwh.harvard.edu:8000/index.html.
76. Department of Mechano-Informatics; Institute of Environment Studies, Tokyo University; www.i.u-tokyo.ac.jp/m-i/m-i-e.htm.
77. Institute for High-Dimensional Medical Imaging, the Jikei University School of Medicine, Tokyo, Japan.
78. Department of Mechanical Engineering, Iwate University, Iwate, Japan; www.mech.iwate-u.ac.jp/.
79. Department of Mechano-Informatics, University of Tokyo, Japan; www.atre.t.u-tokyo.ac.jp.
80. CIMIL Laboratory, Nanyang Technological University, Singapore; http://mrcas.mpe.ntu.edu.sg/research/neurobot/index.htm.
81. Philips Medical Systems, Cleveland, OH, USA.
82. MicroDexterity Systems, Inc., Albuquerque, NM, USA; www.microdexsys.com.
83. Columbia University, Department of Computer Science, New York, NY, USA; http://www1.cs.columbia.edu/∼laza/stewart/.
84. Department of Otorhinolaryngology, Head and Neck Surgery, University of Erlangen-Nürnberg, Germany; www.hno.med.uni-erlangen.de.
85. CAS Innovations GmbH, Erlangen, Germany; www.cas-innovations.de; Medical Intelligence GmbH, Schwabmünchen, Germany; www.medint.de.
86. Surgical Robotics Lab, Berlin, Germany; www.srl-berlin.de.
87. ISIS S.A.S., St Martin d'Heres, France; www.isis-robotics.com.
89. Laboratorium für Medizinrobotik, Sektion sensorische Biophysik, Universitätsklinikum Tübingen, Germany; www.medizin.uni-tuebingen.de/hno/mednavrobotik/projekt/projekt.htm.
90. Fraunhofer Institut für Produktionstechnik und Automatisierung, Stuttgart, Germany; www.ipa.fhg.de/medizin.
91. Lehrstuhl für Angewandte Informatik III, Universität Bayreuth, Germany; http://ai3.inf.uni-bayreuth.de.
92. CEA-List, Service Robotique et Systèmes Interactifs, Centre de Fontenay-aux-Roses, France; CHU Amiens, Service de Chirurgie Maxillo-Faciale, Amiens, France.
93. Med3D GmbH, Heidelberg, Germany; www.med3d.de.
94. Innovation Center Computer Assisted Surgery, Leipzig, Germany; www.uni-leipzig.de/∼herz/_iccas/de/.
95. CISST, Johns Hopkins University, Baltimore, MD, USA; www.cisst.org.
96. MicroDexterity Systems, Inc., Albuquerque, NM, USA; www.microdexsys.com.
97. Helmholtz-Institut für biomedizinische Technik der RWTH Aachen, Germany; www.hia.rwth-aachen.de/research/cht/cranio.html.
98. Universal Robotic Systems GmbH, Schwerin, Germany; www.medicalrobots.com.
99. Laboratoire TIMC, Grenoble, France; http://www-timc.imag.fr/.
100. Group for Surgical Robotics and Instrumentation, Université de Lausanne, Switzerland; http://dmtwww.epfl.ch/imt/robchir/Minerva.html.
101. Department of Clinical Neurosciences, University of Calgary, Canada; www.mdrobotics.ca/neuroarm.htm.
102. Advanced Therapeutic and Rehabilitation Engineering Laboratory, University of Tokyo, Japan; www.atre.t.u-tokyo.ac.jp/index.html.
103. CIMIL Laboratory, Nanyang Technological University, Singapore; http://mrcas.mpe.ntu.edu.sg/research/neurobot/index.htm.
104. Integrated Surgical Systems, Inc., Davis, CA, USA; www.robodoc.com.
105. Armstrong Healthcare Ltd, High Wycombe, UK; www.armstrong-healthcare.com.
106. Z-Kat Inc, Hollywood, FL, USA; www.z-kat.com.
107. Barett Technology Inc., Cambridge, MA, USA; www.baretttechnology.com.
108. Chair for Computer Aided Medical Procedures (I-16), Technical University Munich, Germany; http://wwwnavab.in.tum.de/.
109. German Cancer Research Center, Heidelberg, Germany; www.dkfz.de/medphys/medeng/.
110. MRC Systems GmbH, Heidelberg, Germany; www.mrc-systems.de.
111. Advanced Therapeutic and Rehabilitation Engineering Laboratory, University of Tokyo, Japan; www.atre.t.u-tokyo.ac.jp/index.html.
112. Mechanical Engineering Research Laboratory, Hitachi Ltd., Kandatsu, Tsuchiura, Ibaraki, Japan; www.hitachi.co.jp/div/merl/index-e.html.
113. Department of Mechanical Engineering, Waseda University Tokyo, Japan; www.mech.waseda.ac.jp/.
114. Advanced Therapeutic Engineering Laboratory, Tokyo Denki University, Japan; www.atl.b.dendai.ac.jp/lab/atlab-e.htm.
115. National Insitute of Advanced Industrial Science and Technology, Tsukuba, Japan; http://unit.aist.go.jp/humanbiomed/surgical/.
116. Department of Micro System Engineering, Nagoya University, Japan; www.mech.nagoya-u.ac.jp.
117. School of Engineering, Tokyo University, Japan.
118. Laboratory for Computational Motor Control, Johns Hopkins University, Baltimore, MD, USA; www.bme.jhu.edu/∼reza/fmri_robot.htm.
119. The Acrobot Company Ltd., London, UK; www.acrobot.co.uk.
120. ISIS, Georgetown University, Washington, DC, USA, Urobotics Lab, Johns Hopkins Medical Institutions, Baltimore, MD, USA.
121. Brady Urological Institute, Johns Hopkins Medical Institutions, Baltimore, MD, USA; http://urology.jhu.edu/urobotics/projects/rcm/.
122. Imaging Service and Information System, Georgetown University, Washington, DC, USA; www.visualization.georgetown.edu/research/image_guided/image_guided.htm.
124. Telerobotics and Control Laboratory, Korea Advanced Institute of Science and Technology (KAIST); http://robot.kaist.ac.kr/.
126. LIRMM, Département Robotique, Montpellier, France; www.lirmm.fr/xml/fr/0023-28.html.
127. Medtech S.A., Cap Omega, Montpellier, France; www.medtech.fr/.
128. At first Ortomaquet GmbH, Rastatt, Germany, later from May '01 URS GmbH, Schwerin, Germany.
129. Helmholtz-Institut für Biomedizinische Technik der RWTH Aachen, Germany; www.hia.rwth-aachen.de.
131. PI precision implants AG, Aarau, Switzerland; www.pisystems.ch.
132. MEDACTA AG, Castel San Pietro, Switzerland; www.medacta.ch.
133. Department of Mechanical Engineering, Katholieke Universiteit Leuven, Belgium; www.mech.kuleuven.ac.be/bmgo/research/project_robot_en.phtml.
135. Labor für Biomechanik und experimentelle Orthopädie, Orthopädische Universitätsklinik, Mannheim, Germany; www.intelligent-tool-drive.de.
136. Lehrstuhl für Informatik V, Universität Mannheim, Germany; http://www-li5.ti.uni-mannheim.de/.
137. Brainlab AG, Heimstetten, Germany; www.brainlab.com.
138. Faculty of Mechanical Engineering, Technion, and Masor Robotics Ltd., Haifa, Israel; http://meeng.technion.ac.il.
139. Mazor Surgical Technologies, Caesarea 38900, Israel; www.mazorst.com.
140. CRIM, Scuola St'Anna, Pisa, Italia; http://www-crim.sssup.it/research/projects/mias/defaultarthro.htm.
141. Helmholtz-Institut für Biomedizinische Technik der RWTH Aachen, Germany; www.hia.rwth-aachen.de/research/cht/minaro.html.
142. Universität Siegen, Germany; www.modicas.de.
143. German Aerospace Center, Oberpfaffenhofen, Germany; www.robotic.dlr.de/tobias.ortmaier/.
144. Armstrong Healthcare Ltd, High Wycombe, UK; www.armstrong-healthcare.com.
145. Carnegie Mellon University, Pittsburgh, PA, USA; www.mrcas.ri.cmu.edu.
146. Praxim-Medivision, La Tronche, France; www.praxim.fr.
147. Waseda University, Tokyo, Japan.
148. Integrated Surgical Systems, Inc., Davis, CA, USA; www.robodoc.com.
149. Witherspoon, ISS, Davis, CA, USA; www.robodoc.com.
150. Fraunhofer Institut für Produktionstechnik und Automatisierung, Stuttgart, Germany; www.ipa.fhg.de/medizin.
151. Technion, Haifa, Israel; http://robotics.technion.ac.il.
155. Biomechanics Lab, Istituti Ortopedici Rizzoli, Bologna, Italy; www.ior.it/biomec/homeenglish.htm.
156. Advanced Therapeutic Engineering Laboratory, Tokyo Denki University, Japan; www.atl.b.dendai.ac.jp/lab/atlab-e.htm.
157. University of Tokyo, Japan.
158. CISS, Hanyang University, Seoul, Korea; http://ciss.hanyang.ac.kr.
159. Accuray, Inc., Sunnyvale, CA, USA; www.accuray.com.
160. Medical Intelligence GmbH, Schwabmünchen, Germany; www.medical-intelligence.com.
161. Lehrstuhl Informatik IX, TU München, Germany; http://wwwradig.informatik.tu-muenchen.de/research/med/index_e.html.
162. Institut für Robotik und kognitive Systeme, Universität Lübeck, Germany; www.rob.uni-luebeck.de/.
163. Institute for Nuclear Physics, Orsay, France; http://ipnweb.in2p3.fr/.
164. Centre Protonthérapie d'orsay, France; www.protontherapie-orsay.fr/.
165. iRobot, Burlington, MA, USA; www.irobot.com.
167. Laboratoire d'Informatique de Robotique et de Microélectronique de Montpellier (LIRMM), SINTERS SA, Toulouse, L'Hôpital Lapeyronie, Montpellier, France; www.lirmm.fr/∼duchemin/indexrm.htm.
168. BG Unfallklinik Hamburg, Germany; www.tu-harburg.de/mst/deutsch/forschung/weinrich.shtml.
169. Mechatronics Faculty, FH Regensburg, Germany; http://homepages.fh-regensburg.de/∼mog39099/mk.org/mru/projekt/reprobo/reprobo.htm.
170. IRP, Universität Braunschweig, Germany; www.cs.tu-bs.de/rob/femur.html.
171. Brady Urological Institute, Johns Hopkins Medical Institutions, Baltimore, MD, USA; http://urology.jhu.edu/urobotics/projects/rcm/.
172. Imperial College London, UK; www.me.ic.ac.uk/case/mim/projects/probot/.
173. CIMIL Laboratory, Nanyang Technological University, Singapore; http://mrcas.mpe.ntu.edu.sg/research/urobot/index.htm.
174. Imperial College London, UK.
175. Imaging Research Laboratories, Robarts Institute, London, ON, Canada; www.imaging.robarts.ca/∼afenster/html/researchintereststwo.html.
176. Engineering Research Center, Johns Hopkins University, Baltimore, MD, USA; http://cisstweb.cs.jhu.edu/.
177. PUMA is a common abbreviaton for articulated robots and stands for Programmable Universal Machine for Assembly (www.eng.monash.edu.au/control/labecse.html#PUMA%20560). SCARA stands for Selectively Compliant Articulated Robot Arm (www.systemdevices.co.uk/robots/scara.html).
References
- Cleary K, Nguyen C. State of the art in surgical robotics: Clinical applications and technology challenges. Comput Aided Surg 2001; 6: 312–328
- Taylor R, Stoianovici D. Medical robotics in computer-integrated surgery. IEEE Trans Robot Autom 2003; 19(5)765–781
- Nolte LP, Langlotz F. Intraoperative Navigationssysteme. Trauma Berufskrankheit 1999; 1: 108–115
- Suhm N, Messmer P, Jakob AL, Regazzoni P. Navigationssysteme in der Unfallchirurgie-ein Überblick. OP J 2000; 16: 144–149
- Pott PP, Schwarz M. Robotik, Navigation. Telechirurgie: Stand der Technik und Marktübersicht. Zeitschrift für Orthopädie 2002; 140(5)218–231
- Boehm DH, Reichenspurner H, Detter C, Arnold M, Gulbins H, Meiser B, Reichart B. Clinical use of a computer-enhanced surgical robotic system for endoscopic coronary artery bypass grafting on the beating heart. Thorac Cardiovasc Surg 2000; 48: 198–202
- Cadeddu JA, Stoianovici D, Kavoussi L. Robotics in urologic surgery. Urology 1997; 49: 501–507
- Mohr FW, Onnasch JF, Falk V. The evolution of minimally invasive valve surgery—2 year experience. Eur J Cardiothorac Surg 1999; 15: 233–238
- Berkelman P, Cinquin P, Troccaz J, Ayoubi J, Letoublon C, Bouchard F. A compact, compliant laparoscopic endoscope manipulator. IEEE International Conference on Robotics and Automation. May, 11–15, 2002; 1870–1875
- Berkelman P, Cinquin P, Boidard E, Troccaz C, Letoublon C, Ayoubi J-M. Design, control, and testing of a novel compact laparoscopic endoscope manipulator. Proc Instn Mech Engrs Part I: J Systems and Control Engineering 2003; 217(14)329–341
- Masuda K, Kimura E, Tateishi N, Ishihara K. Three dimensional motion mechanism of ultrasound probe and first application for tele-echography system. ternational Conference of the IEEE Intelligent Robots and Systems IROS. Maui, 2001; 1112–1116
- Masuda K, Tateishi N, Suzuki Y, Kimura E, Wie Y, Ishihara K. Experiment of wireless tele-echography system by controlling echographic diagnosis robot. 5th International Conference on Medical Image Computing and Computer Assisted Intervention (MICCAI 2002. Tokyo 2002; 130–137
- Menciassi A, Dario P. Bio-inspired solutions for locomotion in the gastrointestinal tract: background and perspectives. Philos Transact Ser A Math Phys Eng Sci 2003; 361(1811)2287–2298
- Aiono S, Gilbert J, Soin B, Finlay P, Gordon A. Controlled trial of the introduction of a robotic camera assistant (EndoAssist) for laparoscopic cholectystectomy. Surg Endosc 2002; 16(9)1267–1270
- Buess GF, Arezzo A, Schurr MO, Ulmer F, Fischer H, Gumb L, Testa T, Nobman C. A new remote-controlled endoscope positioning system for endoscopic solo surgery—The FIPS endoarm. Surg Endosc-Ultrasound Interven Tech 2000; 14(4)395–399
- Delgorges C, Al Bassit L, Novales C. OETLO Project: mObile Tele-Echography using an ultra-light rObot. Telemed'02. London, UK 2002
- Kobayashi E, Masamune K, Sakuma I, Dohi T, Hashimoto D. A new safe laparoscopic manipulator system with a five-bar linkage mechanism and an optical zoom. Comput Aided Surg 1999; 4(4)182–192
- Berkelmann P, Boidard E, Cinquin P, Troccaz J. From the laboratory to the operating room: usability testing of LER the light endoscope robot. Workshop on Medical Robotics, Navigation and Visualization (MRNV). RemagenGermany 2004, 11–12 March
- Lauer W, Serefoglou S, Behrend H, Hüwel N, Fischer M, Radermacher K. Entwicklung einer neuartigen, semirobotischen Handhabungsplattform für ein elektronisches OP-Mikroskop. Biomedizinische Technik 2003; 48/1: 520–521
- Carrozza M, Lencioni L, Magnani B, D'Attanasio S, Dario P. The development of a microrobot system for colonoscopy. CVRMed and MRCAS. Grenoble 1997; 779–789
- Dario P, Carrozza MC, Pietrabissa A. Development and in vitro testing of a miniature robotic system for computer-assisted colonoscopy. Comput Aided Surg 1999; 4(1)1–14
- Radermacher K, Westrich D, Heilige M, Brandt G, Jungk A, Rau G. PAROMIS—Ein Parallelrobotersystem für die sprachgesteuerte Kameraführung in der MIC. Biomedizinische Technik 2001; 46/1: 366–367
- Vilchis A, Masuda K, Troccaz J, Cinquin P. Robot-based tele-echography: the TER system. Stud Health Technol Inform 2003; 95: 212–217
- Abolmaesumi P, Salcudean S, Zhu W, Sirouspour M, DiMaio SP. Image-guided control of a robot for medical ultrasound. IEEE Conference on Robotics and Automation. February, 2002; 11–23
- Salcudean S, Zhu W, Abolmaesumi P, Bachmann S, Lawrence PD. A robot system for medical ultrasound. ISRR 1999; 195–202
- Binder N, Matthäus L, Berger A, Schweikard A. The inverse kinematics of fluoroscopic C-arms. 3 jahrestagung der CURAC. MünchenGermany 2004
- Muñoz V, Gómez de Gabriel J, Fernández-Lozano J, García-Morales I, Molina-Mesa R, Pérezdel-Pulgar C, Serón-Barba J, Azouaghe M. Design and control of a robotic assistant for laparoscopic surgery. SIRS. ToulouseFrance July, 2001; 18–21
- Slatkin A, Burdick J. The development of a robot endoscope. IEEE/RSJ Conference on Intelligent Robots and Systems (IROS. August, 5–9. Pittsburgh, PAUSA 1995
- Oleynikov D, Rentschler M, Hadzialic A, Dumpert J, Platt S, Farritor S. In vivo camera robots provide improved vision for laparoscopic surgery. CARS. Chicago 2004; 787–792
- Kobayashi Y, Chiyoda S, Watabe K, Masafumi O, Nakamura Y. Small occupancy robotic mechanisms for endoscopic surgery. 5th International Conference on Medical Image Computing And Computer Assisted Intervention (MICCAI 2002. TokyoJapan, 2002; 75–82
- Rasmus M. Ein neues Telemanipulatorsystem. 3 Jahrestagung der CURAC. München, cGermany 2004
- Voges U, Holler E, Neisius B, Schurr M, Vollmer T. Evaluation of ARTEMIS, the advanced robotics and telemanipulator system for minimally invasive surgery. IARP 2nd Workshop on Medical Robotics. Karlsruhe 1997; 137–148
- Surry K, Smith W, Mills G, Downey D, Fenster A. A mechanical, three-dimensional ultrasound-guided breast biopsy apparatus. 4th International Conference on Medical Image Computing and Computer Assisted Intervention (MICCAI 2001. UtrechtThe Netherlands, October, 14–17, 2001; 232–239
- Madhani A, Niemeyer G, Salisbury J. The Black Falcon: A teleoperated surgical instrument for minimally invasive surgery. IEEE/RSJ International Conference on Intelligent Robots and Systems (IROS. Victoria B.CCanada, October, 13–17, 1998; 936–944
- Rosen J, Brown J, Chang L, Barreca M, Sinanan M, Hannaford B. The BlueDRAGON—a system for measuring the kinematics and the dynamics of minimally invasive surgical tools in vivo. IEEE International Conference on Robotics and Automation. 2002; 1876–1881
- Brown J, Rosen J, Hannaford B, Sinanan M. A passive mechanical pantograph system for measuring tool position during minimally invasive surgery (Poster). Bioengineering 2000; 28, Supplement 1
- Kronreif G, Fürst M, Kettenbach J, Birkfellner W, Figl M, Hanel R, Hummel J. Integriertes Robotersystem für perkutane Interventionen. 1 Jahrestagung der Deutschen Gesellschaft für Computer- und Roboterassistierte Chirurgie 2002, Leipzig, D
- Kronreif G, Fürst M, Kornfeld M, Ptacek W, Vogele M. Modular programmable targeting device for percutaneous interventions. 3 Jahrestagung der CURAC. MünchenGermany 2004
- Maurin B, Piccin O, Bayle B, Gangloff J, de Mathelin M, Soler L, Gangi A. A new robotic system for CT-guided percutaneous procedures with haptic feedback. CARS. Chicago 23–26July, 2004; 515–520
- Bauernschmitt R. Robotik in der Herzchirurgie. 3 Jahrestagung der CURAC. MünchenGermany 2004
- Bauernschmitt R, Knol A, Mayer H, Nagy I, Schirmbeck E, Wildhirt S, Lange R. Towards robotic heart surgery: Introduction of autonomous procedures into an experimental surgical telemanipulator system. 3 Jahrestagung der CURAC. MünchenGermany 2004
- van Meer F, Estève D. Micromachined silicon 2-axis force sensor for teleoperated surgery. Workshop on Medical Robotics, Navigation and Visualization (MRNV). RemagenGermany 11–12 March, 2004
- Green PS, Hill JH, Satava R. Telepresence: Dextrous procedures in a virtual operating field. Surg Endosc 1991; 192: 192
- Ikuta K, Daifu S, Hasegawa T, Higashikawa H. Hyper-finger for remote minimally invasive surgery in deep area. 5th International Conference on Medical Image Computing and Computer Assisted Intervention (MICCAI 2002. Tokyo, 2002; 173–181
- Virtanen J, Malila M, Louhisalmi Y, Hyvärinen P, Nevala K. Machine vision based fiber optic joint sensor for MR- compatible robot. CARS. Chicago 2004; 555–560
- Franzino R. The Laprotek surgical system and the next generation of robotics. Surg Clin North Am 2003; 83(6)1317–1320
- Düpree H. Das Master Slave System Laprotek als digitale Weiterentwicklung für die moderne minimal-invasive Chirurgie. 2 Jahrestagung der CURAC. NürnbergGermany 2002
- Bzostek A, Schreiner S, Barnes A., et al. An automated system for precise percutaneous access of the renal collecting system. Lecture Notes in computer science. Springer-Verlag;, Heidelberg 1997; 299–308, 1205
- Goradia T, Taylor R, Auer L. Robot-assisted minimally invasive neurosurgical procedures: first experimental experience. First Joint Conference of CVRMed and MRCAS. Grenoble 1997; 319–322
- Taylor RH, Funda J, Eldridge B. A telerobotic assistant for laparoscopic surgery. IEEE Eng Med Biol 1995; 14; 279–287
- Taillant E, Avila-Vilchis JC, Allegrini C, Bricault I, Cinquin P. CT and MR compatible light puncture robot: architectural design and first experiments. 7th International Conference on Medical Image Computing and Computer Assisted Intervention (MICCAI 2004. St MaloFrance. Springer;, Heidelberg 2004; 145–152
- Dombre E, Michelin M, Poignet P, Bidaud P, Morel G, Salle D, Mederic P, Gravez P, Karouia M, Bonnet N. Projet MARGE: Modélisation, Apprentissage et Reproduction du Geste Endochirurgical. Actes des Journées du Programme Interdisciplinaire CNRS, ROBEA 2002
- Michelin M, Dombre E, Poignet P, Eckert L. Achieving motion under a penetration point constraint. IROS'02: IEEE International Conference on Intelligent Robots and Systems. Lausanne, 2002; 1475–1480
- Zemiti N, Ortmaier T, Vitrani M, Morel G. A force controlled laparoscopic surgical robot without distal force sensing. 9th International Symposium on Experimental Robotics, ISER 2004. Singapore 18–12 June, 2004
- Krupa A, de Mathelin M, Doignon C, Gangloff J, Morel G, Soler L, Leroy J, Marescaux J. Automatic 3-D positioning of surgical instruments during robotized laparoscopic surgery using automatic visual feedback. MS4CMS'02. Rocquencourt 2002; 9–16
- Ang W, Riviere C, Khosla P. An active handheld instrument for enhanced microsurgical accuracy. 3rd International Conference on Medical Image Computing and Computer Assisted Intervention (MICCAI 2000. Pittsburgh, PAUSA, October, 11–14, 2000
- Riviere C, Khosla P. Active handheld instrument for error-compensation in microsurgery. telligent Systems and Manufacturing, Technical Conference on Microrobotics and Microsystems Fabrication. Pittsburgh, October, 16–17, 1997; 86–95
- Kumar R, Berkelman P, Gupta P, Barnes A, Jensen P, Withcomb L, Taylor R. Preliminary experiments in cooperative human/robot force control for robot assisted microsurgical manipulation. IEEE International Conference on Robotics and Automation. San FranciscoUSA 2000
- Meier P, Preuß R, Oberthür S. Development of an artificial worm for minimal invasive surgery. 38 Jahrestagung der DGBMT. Ilmenau 2004; 116–117
- Schneider O, Troccaz J. A six-degree-of-freedom passive arm with dynamic constraints (PADyC) for cardiac surgery application: preliminary experiments. Comput Aided Surg 2001; 6(6)340–351
- Das H, Charles S, Ohm T, Boswell C, Rodriguez G, Steele R, Paljug E. A telerobotics workstation for microsurgery. Medicine Meets Virtual Reality, 5th Conferenc. San Diego, CAUSA, January, 1997
- Kaiser WA, Fischer H, Vagner J, Selig M. Robotic system for biopsy and therapy of breast lesions in a high-field whole-body magnetic resonance tomography unit. Invest Radiol 2000; 35(8)513–519
- Suzuki T, Nishida Y, Kobayashi E, Tsuji T, Fukuyo T, Kenada M, Konishi K, Hashizume M, Sakuma I. Development of a robotic laser surgical tool with integrated video endsocope. 7th International Conference on Medical Image Computing and Computer Assisted Intervention (MICCAI 2004. St MaloFrance. Springer;, Heidelberg 2004; 25–32
- Patronik N, Zenati M, Riviere C. Crawling on the heart: A mobile robotic device for minimally invasive cardiac interventions. 7th International Conference on Medical Image Computing and Computer Assisted Intervention (MICCAI 2004. St MaloFrance, 2004
- Patronik N, Zenati M, Riviere C. Development of a tethered epicardial crawler for minimally invasive cardiac therapies. IEEE;. IEEE 30th Annual Northeast Bioengineering Conference. 2004; 239–240
- Cavusoglu MC, Williams W, Tendick F, Sastry S. Robotics for telesurgery: second generation Berkeley/UCSF laparoscopic telesurgical workstation and looking towards the future applications. 39th Allerton Conference on Communication, Control and Computing. Monticello, IL, October, 3–5, 2001
- Mosso-Vázquez JL, Minor MA, Pérez GR, Lara VV, Mosso VA, Torres OJG, Castañeda CI, Padilla SL, García PR, González CC, Rocha MR, et al. From Puma of Unimation 6000 Robot to Tonatiuh Robot and Hand Free Navigation System. Laparoscopic assistant 1996–2003. EU-LAt Workshop e-health. Cuernavaca, México 1–4 December, 2003
- Mosso-Vázquez J. Navegación endoscópica asistida por un robot. Experiencia en un animal de experimentación. Cirugía y Cirujanos 2002; 346–349
- Hong J-S, Dohi T, Hasizume M, Konishi K, Nobuhiko H. Ultrasound guided motion adaptive instrument for percutaneous needle insertion therapy. 6th International Conference on Biomedical Engineering and Rehabilitation Engineering. GuilinChina, 2002
- Salcudean S, Ku S, Bell G. Performance measurement in scaled teleoperation for microsurgery. 1st Joint Conference CVRMed and MRCAS. Springer, Grenoble 1997; 789–798
- Guo-Qing W, Arbter K, Hirzinger G. Real-time visual servoing for laparoscopic surgery. IEEE Eng Med Biol 1997; 16(1)40–45
- Nagel N, Schmidt G, Petzold P, Kalender W. Motion detection and prevention for a robot-assisted needle positioning system. 3 Jahrestagung der CURAC. München, Germany 2004
- Hoerauf H, Wollnack J, Laqua H, Schweikard A. Development of a microsurgical technique for retinal endovascular surgery. 3 Jahrestagung der CURAC 2004
- Palombara P, Fadda M, Martelli S, Nofrini L, Marcacci M. A minimally invasive 3-D data registration protocol for computer and robot assisted total knee arthroplasty. CVRMed-MRCAS'97 1997
- Chinzei K, Hata N, Jolesz F, Kikinis R. MR compatible surgical assist robot: system integration and preliminary feasibility study. 3rd International Conference on Medical Image Computing and Computer Assisted Intervention (MICCAI 2000. Springer Verlag, Pittsburgh 2000; 921–930
- Hata N, Jinzaki M, Kacher D, Cormak R, Gering D, Nabavi A, Silverman SG, D'Amico AV, Kikinis R, Jolesz FA, Tempany C. MRI-guided prostate biopsy using surgical navigation software: device validation and feasibility. Radiology 2001; 220(1)263–268
- Daeyoung K., Etsuko K., Dohi T, Sakuma I. A new, compact MR-compatible surgical manipulator for minimally invasive liver surgery. 5th International Conference on Medical Image Computing and Computer-Assisted Intervention. TokyoJapan, 2002
- Hatori A, Suzuki N, Hayashibe M, Suzuki S, Otake Y, Sumiyama K, Tajiri H, Kobayashi S. Navigation system for a developed endoscopic surgical robot system. CARS. ChicagoUSA 2004
- Suzuki T, Aoki E, Kobayashi E, Tsuji T, Konishi K, Hashizume M, Sakuma I. Development of forceps manipulator for assisting laparoscopic surgery. CARS. Chicago 2004; 1338
- Shimachi S, Fujiwara Y, Hakozaki Y. New sensing method of force acting on instrument for laparoscopic robot surgery. CARS. Chicago 2004; 775–780
- Hata N, Ohara F, Hashimoto R, Hashizume M, Dohi T. Needle guiding robot with five-bar linkage for MR-guided thermotherapy of liver tumor. 7th International Conference on Medical Image Computing and Computer Assisted Intervention (MICCA. St MaloFrance. Heidelberg: Springer-Verlag 2004 2004; 161–168
- Wudelete R, Kassim I, Bock W, Sing W. Combined tracking system for augmented reality assisted treatment device. Workshop on Medical Robotics, Navigation and Visualization (MRNV). RemagenGermany 2004
- Yanof J, Haaga J, Klahr P, Bauer C, Nakamoto D, Chaturvedi A, Bruce R. CT integrated robot for interventional procedures: preliminary experiment and computer–human interfaces. Comp Aided Surg 2001; 6(6)352–359
- Charles S, Stuart J, Bronisz L.. Patent US2002/0133174 A1. 19.09.2002, 2002, Surgical Manipulator
- Bumm K, Steinhart H, Wurm J, Vogele M, Nimsky CH, Iro H. A novel robot system for fully automated and telemanipulation surgery of the paranasal sphenoid sinus. InterlakenSwitzerland 2003, Computer Aided Surgery around the Head
- Hein A, Kneissler M, Mätzig M, Lüth T. Navigated Control—Ein neuer Ansatz für das exakte Fräsen. 1 Jahrestagung der CURAC. Leipzig, Germany 2004
- Schauer D, Lüth T. RoboPoint—Ein sterilisierbarer interaktiver Miniatur-Roboter zur Instrumentenführung. 1 Jahrestagung der CURAC. Leipzig 4–6 November, 2002
- Lueth TC, Hein A, Albrecht J, Demirtas M, Zachow S, Heissler E, Klein M, Menneking H, Hommel G, Bier J. A surgical robot system for maxillofacial surgery. IEEE International Conference on Industrial Electronics, Control, and Instrumentation (IECON. Aachen/Germany, September, 1998; 2470–2475
- Engel D, Raczkowsky J, Wörn H. A safe robot system for craniofacial surgery. IEEE International Conference On Robotics And Automation. SeoulKorea, 2001
- Engel D, Raczkowsky J, Wörn H. RobaCKa: Ein Robotersystem für den Einsatz in der Chirurgie. Symposium des SFB 414: Rechner- und sensorgestützte Chirurgie. 2001, Köllen Verlag
- Korb W, Engel D, Boesecke R, Eggers G, Kotrikova B, Marmulla R, O'Sullivan N, Raczkowsky J, Hassfeld S. Chirurgieroboter für Kraniotomien–Risikoanalyse und erster Patientenversuch. Automatisierungstechnik 2004; 6: 288–295
- Dammann F, Bode A, Schwaderer E, Schaich M, Heuschmid M, Maassen M. Computer-aided surgical planning for implantation of hearing aids based on CT-data in a VR-environment. Radiographics 2001; 21: 184–190
- Federspil P, Geisthoff U, Henrich D, Plinkert P. Development of the first force-controlled robot for otoneurosurgery. Laryngoscope 2003; 113: 465–472
- Bonneau E, Taha F, Gravez P, Lamy S. SURGICOBOT: Surgical Gesture Assistance COBOT for maxillo-facial interventions. Workshop on Medical Robotics, Navigation and Visualization (MRNV). RemagenGermany 11–12 March, 2004
- Dressler S, Strauss G, Krabbes M, Pretschner A, Pfeiffer E, Böttcher M, Dietz A. Mechatronical systems for microlaryngoscopy. 3 Jahrestagung der CURAC. MünchenGermany 2004
- Simaan N, Taylor R, Flint P. High dexterity snake-like robotic slaves for minimally invasive telesurgery of the upper airway. 7th International Conference on Medical Image Computing and Computer Assisted Intervention (MICCA. St. MaloFrance. Springer, Heidelberg 2004; 17–24, 2004
- Stuart J.. USA patent US 6702805. 09.03.04, 2004, Manipulator
- Bast P, Engelhardt M, Popovic A, Schmieder K, Radermacher K. CRANIO—Entwicklung eines Systems zur computer- und roboterunterstützten Kraniotomie. Biomedizinische Technik 2002; 47/1(1)9–11
- Cinquin P, Troccaz J, Demongeot J, Lavallee S, Champleboux G, Brunie L, Leitner F, Sautot P, Mazier B, Perez A, Djaid M, Fortin T, Chenic M, Chapel A. IGOR: Image guided operating robot. Innovation et Technol Biol Med 1992; 13: 374–394
- Glauser D, Frankhauser H, Epitaux M, Hefti J, Jaccottet A. Neurosurgical Robot Minerva: first results and current developments. Second Annual International Symposium on Medical Robotics and Computer Assisted Surgery, MRCAS'95. BaltimoreUSA 4–7 November, 1995
- Sutherland G, McBeth PB, Louw D. NeuroArm: an MR compatible robot for microsurgery. 17th international meeting of CARS. Elesevier, London, GB 2003; 504–508
- Louw DF, Fielding T, McBeth PB, Gregoris D, Newhook P, Sutherland G. Surgical robotics: a review and neurosurgical prototype development. Neurosurgery 2004; 54: 525–537
- Rizun PR, McBeth PB, Louw DF, Sutherland G. Robot-assisted neurosurgery. Semin Laparosc Surg 2004; 11(2)99–106
- Hongo K, Goto T, Kakizawa Y, Koyama J, Kawai T, Kan K, Tanaka Y, Kobayashi S. Micromanipulator system (NeuRobot) clinical application in neurosurgery. 17th international meeting of CARS. Elsevier, London 2003; 509–513
- Hongo K, Kobayashi S, Kakizawa Y, Koyama J, Goto T, Okudera H, Kan K, Fujie MG, Iseki H, Takakura K. NeuRobot: telecontrolled micromanipulator system for minimally invasive microneurosurgery—preliminary results. Neurosurgery 2002; 51(4)985–988
- Lavallee S, Troccaz J, Gaborit L, Cinquin P, Benabid AL, Hoffmann D. Image-guided operating robot: a clinical application in stereotactic neurosurgery. Computer-integrated surgery: technology and clinical applications, RH Taylor, S Lavallee, GC Burdea, R Mösges. MIT Press;, Cambridge, MA 1996; 343–351
- Quaid A, Abovitz A. Haptic information displays for computer-assisted surgery. Robotics and Automation (ICRA '02) 2002; 2092–2097
- Loser M, Navab N. A new robotic system for visually controlled percutaneous interventions under CT fluoroscopy. 3rd International Conference on Medical Image Computing and Computer Assisted Intervention (MICCAI 2000. PittsburghUSA, 2000; 887–896
- Korb W, Barthold S, Bendl R, Echner G, Grosser K, Pastyr O, Treuer H, Sturm V, Schlegel W. Entwicklung eines Hochpräzisions-Manipulators für die stereotaktische Neurochirurgie. Rechner- und Sensorgestützte Chirurgie. Heidelberg 19–20 July, 2001; 336–343
- Korb W, Barthold S, Bendl R, Echner G, Pastyr O, Treuer H, Sturm V, Schlegel W. Modelling, simulation and control of high-precision neurosurgical robot. EMBEC2002. ViennaAustria 2002
- Goetz M, Fischer S, Velten A, Bille J, Sturm V. Computer-guided laser probe for ablation of brain tumours with ultrashort laser pulses. Phys Med Biol 1999; 44(6)119–127
- Masamune K, Stoianovici D, Sakuma I, Dohi T, Iseki H. Direct MR image guided positioning manipulator for percutaneous needle puncturing therapy. 32nd International Symposium on Robotics. Seoul 2001; 619–624
- Fichtinger G, DeWeese TL, Patriciu A, Tanacs A, Mazilu D, Anderson JH, Masamune K, Taylor RH, Stoianovici D. Robotically assisted prostate biopsy and therapy with intra-operative CT guidance. J Acad Radiol 2001; 9(1)30–74
- Tajima F, Kishi K, Kan K, Ishii H, Nishizawa K, Fujie M, Dohi T, Sudo K, Takamoto S. An MR-compatible master–slave manipulator with interchangeable surgical tools. 17th international meeting of CARS. Elsevier, London 2003; 529–537
- Okamoto J, Iida M, Nambu K, Okayasu H, Fujie M, Umezu M, Iseki H. Development of multi-DOF brain retract manipulator for minimally invasive neurosurgery. 17th international meeting of CARS. Elsevier, London 2003; 522–528
- Masamune K, Kobayashi E, Masutani Y, Suzuki M, Dohi T, Iseki H, Takakura K. Development of an MRI-compatible needle insertion manipulator for stereotactic neurosurgery. J Image Guided Sur 1995; 1: 242–248
- Koseki Y, Toshikatsu W, Chinzei K, Iseki H. Endocope manipulator for trans-nasal neurosurgery, optimized for and compatible to vertical field open MRI. 5th International Conference on Medical Image Computing and Computer Assisted Intervention (MICCA. Tokyo, 2002; 114–121
- Ikuta K, Sasaki K, Yamamoto K, Shimada T. Remote microsurgery system for deep and narrow space—development of new surgical procedure and micro-robotic tool. 5th International Conference on Medical Image Computing and Computer Assisted Intervention (MICCA. Tokyo, 2002; 163–172
- Asai D, Katopo S, Arata J, Warisawa S, Mitsuishi M, Morita A, Sora S, Kirino T, Mochizuki R. Micro-neurosurgical system in the deep surgical field. 7th International Conference on Medical Image Computing and Computer Assisted Intervention (MICCA. Springer, HeidelbergFrance 2004; 33–40
- Cobb JP, Hencke J, Harris SJ, Jakopec M, Baena FR, Gomes M, Davies B. An active constraint robot improves outcomes in total knee arthroplasty. 3rd Annual Meeting of CAOS. Marbella 18–21 June, 2003; 64–65
- Jakopec M, Harris SJ, Baena FR, Gomes P, Cobb J, Davies B. The first clinical application of a ‘hands-on’ robotic knee surgery system. Comput Aided Surg 2001; 6(6)329–339
- Cleary K, Stoianovici D, Watson V, Cody R, Hum B, Lindisch D. Robotics for percutaneous spinal procedures: Initial report. Computer Aided Radiology and Surgery. San FranciscoUSA 2002
- Kwon D-S, Lee J-J, Yoon Y-S, Ko S-Y, Kim J, Chung J-H, Won C-H, Jong-Hwa K. The mechanism and the registration method of a surgical robot for total hip arthroplasty. IEEE International Conference on Robotics & Automation. Washington DCUSA, 11–15 May, 1889–1894
- Nahum B, Blondel L, Tassel E, Dombre E, Poignet P, Maillet P, Maury P. A cutting guide positioner robot to improve bone-cutting precission in knee osteotomy. 4th annual meeting of CAOS. USA, Chicago, IL, 16–19 June
- Ritschl P, Machacek F, Fuiko R. Computer assisted ligament balancing in TKR using the Galileo system. 3rd Annual Meeting of CAOS, FDB Langlotz, A Bauer. Steinkopf, Marbella, Spain 18–21 June, 2003; 304–305
- Pott PP, Schwarz MLR, Köpfle A, Schill M, Wagner A, Badreddin E, Männer R, Weiser P, Scharf H-P. Ein Handgehaltener Operationsroboter—Grundlagen, Spezifikationen und Lösungsentwurf. 1 Jahrestagung der CURAC. Leipzig, Germany 4–5 October, 2002
- Pott PP, Schwarz MLR, Köpfle A, Schill M, Wagner A, Badreddin E. ITD—A handheld manipulator for medical applications—Concept and design. In: Langlotz F, Davies B, Bauer A, editors. 3rd annual meeting of CAOS. MarbellaSpain. Steinkopf, Darmstadf, Männer R, Weiser P, Scharf H-P, 290–291
- Koepfle A, Schill M, Schwarz MLR, Pott PP, Wagner A, Männer R, Badreddin E, Weiser P, Scharf H-P. A modular scalable approach to occlusion-robust low-latency optical tracking. 7th International Conference on Medical Image Computing and Computer Assisted Intervention (MICCA. St. MaloFrance, 26–30 September
- Pott PP, Weiser P, Scharf H-P, Schwarz M. Getriebe mit 4 Freiheitsgraden für robotische Anwendungen in der Medizin. Zeitschrift für Biomedizinische Technik 2004; 49(6)176–179
- Shoham M, Burman M, Zehavi E, Joskowicz L, Batkilin E, Kunicher Y. Bone mounted miniature robot for surgical procedures—concept and applications. In: Langlotz BD, Bauer A, editors. 3rd annual meeting of CAOS. Spain. Steinkopf, Darmstadt, 18–21 June, 330–331
- Shoham M, Burman M, Zehavi E, Kunicher Y. MARS: miniature bone-mounted robot. ISRACAS 2003. Tel Aviv, Israel 15 May, 2003
- Joskowicz L, Milgrom C, Shoham M, Yaniv Z, Simkin A. (2003) A robot-assisted system for long bone intramedullary distal locking: concept and preliminary results. 17th international meeting of CARS. 2003. Elsevier Science, London, 485–491
- Dario P, Paggetti C, Troisfontaine N, Papa E, Ciucci T, Carrozza M, Marcacci M. A miniature steerable end-effector for application in an integrated system for computer-assisted arthroscopy. ICRA'97. 1997; 1573–1579
- Dario P, Carrozza M, Marcacci M, D'Attanasio S, Magnani B, Tonet O, Megali G. A novel mechatronic tool for computer assisted arthroscopy. IEEE Trans Inform Technol Biomed 2000;; 4: 15–29
- Tonet O, Megali G, D'Attanasio S, Dario P, Carrozza M, Marcacci M, Martelli S, Palombara PL. An augmented reality navigation system for computer assisted arthroscopic surgery of the knee. 3rd International Conference on Medical Image Computing and Computer Assisted Intervention (MICCA. Pittsburgh, PA 2000; 1158–1162
- de la Fuente M, Ohnsorge J, Bast P, Wirtz DC, Radermacher K. MINARO—Neue Ansätze für die minimalinvasive röntgenbildbasierte Revisionshüftendoprothetik. Biomedizinische Technik. 2002; 47/1(1)44–46
- Wahrburg J, Kerschbaumer F. Überlegungen zum Einsatz mechatronischer Implantationshilfen bei Minimalzugängen für Hüftendoprothesen. Der Orthopäde 2000; 29(7)650–657
- Konietschke R, Ortmaier T, Weiss H, Hirzinger G, Engelke R. Manipulability and accuracy measures for a medical robot in minimally invasive surgery. 9th International Symposium on Advances in Robot Kinematics International Federation for the Promotion of Mechanism and Machine Science. Sestri Levante, Italy 2004
- Brisson G, Kanade T, DiGioia AM, Jaramaz B. Precision freehand sculping of bone. 7th International Conference on Medical Image Computing and Computer Assisted Intervention (MICCA. 3rd annual meeting of CAOS, MarbellaSpain. Springer, Heidelberg 2003; 36–37
- Plaskos C, Stindel E, Cinquin P, Hodgson AJ, Faguer B, Lavallee S. PRAXITELES: A universal bone-mounted robot for image-free knee surgery—report on first cadaver trials. CAOS. USA, Chicago, IL 2004
- Yanagihara M, Okamoto J, Fujie M, Yano H, Mitsui N. Development of RAO assisant manipulator. CARS. ChicagoUSA 2004
- Taylor RH, Mittelstadt BD, Paul HA, Hanson W, Kazanzides P, Zuhars JF, Williamson B, Musits BL, Glassman E, Bargar W. An image-directed robotic system for precise orthopaedic surgery. IEEE Trans Robotics Automat 1994; 10: 261–273
- Barger W, Bauer A, Börner M. Primary and revision total hip replacement using the robodoc system. Clin Orthop Related Res 1998; 354: 82–91
- Nogler M, Wimmer C, Lass-Flörl C, Mayr E, Trobos S, Gegenhuber C. Contamination risk of the surgical team through Robodoc's high-speed cutter. Clin Orthop Related Res 2001; 387: 225–231
- Pellengahr C, Refior H. Rotations- und translationsabweichung in der roboterunterstützten Hüftschaftimplantation. Robotic und Navigation int Symposium. Nürnberg 8–9 March, 2002
- Witherspoon L. ROBONAV®-Robotic-systems for minimally invasive surgery. Robotic und Navigation. Internationales Symposium, Dr-Erler-Klinik. NuernbergGermany 8 March, 2004
- Börner M, Wiesel U. Erste Ergebnisse der roboterassistierten Kniegelenkendoprothetik mit dem ROBODOC®-System. Trauma Berufskrankh 2001; 3: 355–359
- Wapler M, Bräucker M, Dürr M, Hiller A, Stallkamp J, Urban V. A voice-controlled robotic assistant for neuroendoscopy. Medicine Meets Virtual Reality 1999
- Plinkert PK, Plinkert B, Hiller A, Stallkamp J. Applications for a robot in the lateral skull base. Evaluation of robot-assisted mastoidectomy in an anatomic specimen. HNO 2001; 49(7)514–522
- Glozman D, Shoham M, Fischer A. Efficient registration of 3-D objects in robotic-assisted surgery. CAOS/USA. Pittsburgh, PAUSA 1999
- Fadda M, Malvisi A, Valleggi R, Bioli G, Martelli S. A new robotic system for operating theatre. J Comp Control Eng 2001; 12(3)129–136
- Masamune K, Fichtinger G, Patriciu A, Susil RC, Taylor RH, Kavoussi LR, Anderson JH, Sakuma I, Dohi T, Stoianovici D. System for robotically assisted percutaneous procedures with computed tomography guidance. Comput Aided Surg 2001; 6(6)370–383
- Sugita N, Warisawa S, Mitsuishi M, Suzuki M, Moriya H, Kuramoto K. Development of a novel robot-assisted orthopaedic system designd for total knee arthroplasty. 7th International Conference on Medical Image Computing and Computer Assisted Intervention (MICCA. St. MaloFrance. Springer, Heidelberg 2004; 153–160
- Park J, Choi K, Yi B, Kim Y. Movement of vertebra spine surgery. CARS. Chicago 2004; 1332
- Chang S, Main W, Martin D, Gibbs I, Heilbrun M. An analysis of the accuracy of the CyberKnife: a robotic frameless stereotactic radiosurgical system. Neurosurgery 2003; 52(1)146–147
- Schweikard A, Shiomi H, Dötter M, Roth M, Berlinger K, Adler J. Fiducial-less compensation of breathing motion in lung cancer radiosurgery. delete 2003, Technical Report A-02–23, Informatik, Universität Lübeck
- Noel G, Ferrand R, Feuvret L, Boisserie G, Meyroneinc S, Mazeron J. Automatization and robotization of the setup and treatment for patients treated for a brain and base skull of the skull tumor. Cancer/Radiotherapie 2003; 7(1)33–41
- Yamauchi B, Pook P, Gruber A. Bloodhound: A semi-autonomous battlefield medical robot. 23th Army Science Conferenc. Orlando, FLUSA, 2003
- Duchemin G, Dombre E, Pierrot F, Poignet P, Urbain L, Téot L. DERMAROB: robot de prélèvement cutané. 15ème Journées des Jeunes Chercheurs en Robotique (JJCR '02). StrasbourgFrance 2002
- Téot L, Duchemin G, Poignet P, Dombre E. DERMAROB: A partial thickness skin harvesting robot: technical and experimental data. 13th Annual Meeting of the European Tissue Repair Society. AmsterdamThe Netherlands 20–23 September, 2003
- Seide K, Wolter D. Entwicklung und klinischer Einsatz eines ‘intelligenten’ Fixateur externe. Trauma Berufskrankheit 2000; 2(Suppl 1)35–37
- Seide K, Weinrich N, Schürmann U, Faschingbauer M, Jürgens C. Automatic external fixator based on parallel robot kinematics for the optimized and telemedically supported outpatient fracture and deformity treatment. 38 Jahrestagung der DGBMT. Ilmenau 2004; 118–119
- Fuchtmeier B, Nerlich M, Monkman G, Egersdörfer S, Raja K. Development of a robotic navigation and fracture fixation system. 23 September 2002. European J Medical Research Abstracts. 7th International Conference on Medical Aspects of Telemedicine, 28–29
- Fuchtmeier B, Egersdoerfer S, Mai R, Hente R, Dragoi D, Monkman G, Nerlich M. Reduction of femoral shaft fractures in vitro by a new developed reduction robot system ‘RepoRobo’. Injury 2004; 35(1)113–119
- Westphal R, Faulstich J, Gösling T, Winkelbach S, Hüfner T, Krettek C, Wahl F. Fracture reduction using a telemanipulator with haptical feedback. 17th Meeting of Computer Assisted Radiology and Surgery. London, 2003; 1369
- Sudelete LM, Stoianovici D, Jarrett TW, Patriciu A, Roberts WW, Cadeddu JA, Ramakumar S, Solomon SB, Kavoussi L. Robotic percutaneous access to the kidney: comparison with standard manual access. J Endourol 2002; 16(7)471–475
- Harris SJ, Arambula-Cosio F, Mei Q, Hibberd RD, Davies BL, Wickham JEA, Nathan MS, Kundu B. The Probot—an active robot for prostate resection. Proc Inst Mech Engrs 1997; 211(4)317–325
- Wei Z. et al. Robot-assisted 3D-TRUS guided prostate brachytherapy: system integration and validation. Med Phys 2004; 31(3): 539–548)
- Wan G, Wei Z, Gardi L, Downey D, Fenster A. Needle Steering for 3D TRUS-guided robot-aided brachytherapy. CARS. Chicago 2004; 1325
- Krieger A, Susil RC, Fichtinger G, Atalar E, Whitcomb L. Design of a novel MRI-compatible manipulator for image guided prostate intervention. IEEE 2004 Conference on Robotics and Automation. New Orleans, LA, 2004; 2517–2522
- Fichtinger G, Krieger A, Susil R, Tancas A, Withcomb L, Atalar E. Transrectal prostate biopsy inside closed MRI scanner with remote actuations under real-time image guidance. 5th International Conference on Medical Image Computing and Computer Assisted Intervention (MICCA. Tokyo, 2002; 91–98
- Riviere C, Khosla P. Microscale tracking of surgical instrument motion. 2nd International Conference on Medical Image Computing and Computer Assisted Intervention (MICCA. CambridgeUK, September, 19–22, 1999
- Dewan M, Marayong P, Okamura A, Hager G. (2004) Vision-based assistance for ophthalmic micro-surgery. 7th International Conference on Medical Image Computing and Computer Assisted Intervention (MICCA. St. MaloFrance, 2004. Springer, Heidelberg, 49–57
- Hong J., et al. An ultrasound-driven needle-insertion robot for percutaneous cholecystostomy. Phys Med Biol 2004;49; 441–455
- Suzuki N. Development of an endoscopic robot system with two hands for various gastric tube surgeries. MMVR 2003; 11: 110–116
- de la Fuente M, Radermacher K, Lutz P, Wirtz D. 3D reconstruction and navigated removal of femoral bone cement in revision THR based on few fluoroscopic images. CARS. Chicago, ILUSA 2004
- Simaan N, Glozman D, Shoham M. Design considerations of new six degrees-of-freedom parallel robots. IEEE International Conference on Robotics and Automation 1998; 1327–1333
- Federspil P, Stallkamp J, Plinkert P. Robotik—eine neue Dimension in der HNO-Heilkunde. HNO 2001; 49: 501–513
- Lueth TC, Bier J. Robot assisted intervention surgery. Neuronavigation—neurosurgical and computer scientific aspects, J Gilsbach, H Stiehl. Springer-Verlag;, Heidelberg 1999
- Visarius H, Nolte LP. Computergestützte Chirurgie: Planung, Simulation, Navigation. Das Krankenhaus 1997; 335–338
- Gosse F, Brack C, Götte H, Roth M, Rühmann O, Schweikard A, Vahldiek M. Roboterunterstützung in der Knieendoprothetik. Der Orthopäde 1997; 26: 258–266
- Honl M, Schwieger K, Gauck CH, Carrero V, Dierk O, Dries S, Hille E, Morlock M. Comparison of robotic versus manual implantation of cementless primary total hip replacement—a prospective clinical study. 49th Annual Meeting of the Orthopaedic Research Society. New Orleans, LAUSA, 2–5 February
- Pott PP, Schwarz MLR, Dürr A, El-Ganadi K, Kramer S, Klandt H, Scharf H-P, Golla S. Market potential of robotic—an empirical pre study of customers, acceptance among CURAC members. Jahrestagung der CURAC. NürnbergGermany 4–7 November, 2003