Abstract
Percutaneous sacroiliac screw fixation is technically demanding and can result in complications mainly related to imaging problems. Furthermore, the conventional technique performed using fluoroscopic control is associated with a long radiation exposure. The purpose of this study was to evaluate the accuracy of two navigation technologies used in traumatology; fluoroscopy and Iso-C3D navigation. A total of 40 screws were placed (20 with Iso-C3D, 20 with 2D fluoroscopy) at levels S1 and S2. With both technologies, all S1 screws could be placed correctly, but four (10%) incorrect placements were seen at S2 with fluoroscopy navigation. With all Iso-C3D navigated drillings, no perforation was seen. Iso-C3D navigation therefore proved superior to 2D fluoroscopy navigation for sacroiliac screw fixation in an experimental set-up designed to assess accuracy.
Introduction
In the treatment of unstable C-type pelvic injuries Citation[1], osteosynthesis with iliosacral screws is a minimally invasive option for stabilizing the posterior pelvic ring Citation[2–5]. Using the conventional fluoroscopy-based technique, the drilling can only be controlled in one projection at once; the position of the screws must be followed and adjusted under fluoroscopy in anterior-posterior (a.p.), inlet, outlet and lateral projections. This leads to increased radiation exposure for the surgeon and patient, and injuries to nerve roots and the gluteal vessels have been reported in 3–15% of cases using this method Citation[6], Citation[7].
More recently, navigation systems have been introduced for traumatological indications, especially in the field of spine and pelvic surgery Citation[8–12]. Particularly in spine surgery, with CT-based navigation, the accuracy of pedicle screw placement could be improved Citation[13], Citation[14]. In unstable pelvic ring injuries, however, CT-based navigation is not applicable, as the fragment positions in the CT dataset may not reflect the intraoperative situation. For these applications, fluoroscopy- and Iso-C3D-based navigation are indicated. The technology of these navigation modalities has been explained elsewhere Citation[15], Citation[16]. For both modalities, the images are acquired intraoperatively and represent the actual situation, e.g., after reduction of a fracture. However, each navigation technology has its advantages and pitfalls () Citation[17].
Table I. Comparison of fluoroscopy and Iso-C3D navigation.
The purpose of this study was to evaluate the accuracy of fluoroscopy and Iso-C3D navigation when used for navigated sacroiliac screw fixation.
Methods
The navigation system SurgiGATE® (Praxim-Medivision, Grenoble, France) was used, including an Ultra 10 Workstation (Sun Microsystems, Palo Alto, CA) and an Optotrak 3020 optoelectronic localizer (Northern Digital Inc., Waterloo, Ontario, Canada) with an accuracy of 0.1 mm in translation and 0.1° in rotation, according to the manufacturer.
All drillings were performed by one examiner, an experienced surgeon, after extensive training in conventional and navigated sacroiliac screw drilling. Drilling was performed with a navigated drilling machine (Powerdrive, Synthes, Bochum, Germany) and new drill bits of 4.5 mm diameter. A navigated drill sleeve was used. After drilling, a k-wire (2.8 mm, Synthes) was inserted into the drill hole and a canulated titanium screw (7.3 mm, Synthes) was placed.
A total of 40 drillings were performed using 10 foam pelvises (Synbone, Malans, Switzerland), Twenty drillings (10 S1, 10 S2) were performed with fluoroscopy-based navigation, and 20 (10 S1, 10 S2) with Iso-C3D navigation. For the drilling, the pelvis was fixed in a special holding device in the supine position, the pelvis itself being covered such that the examiner was blinded.
Postoperative evaluation was done by direct inspection and evaluation of CT images ( and ). The evaluation scored the outcome as follows: 0 = no perforation; 1 = minimal perforation without clinical relevance; 2 = obvious perforation (see ). The postoperative data set was analysed in the DICOM viewer eFilm Workstation™ (Merge eFilm, Milwaukee, WI).
Figure 1. Postoperative scoring of sacroiliac screw placement. A scoring system was developed to evaluate screw placement by direct visualization and by CT. a) Score = 0: no perforation. b) Score = 1: minimal perforation. c) Score = 2: obvious perforation.
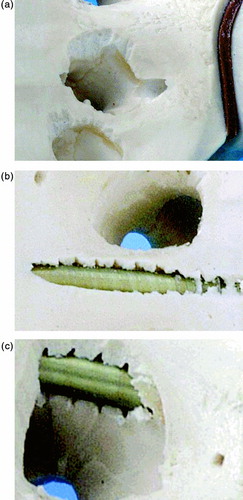
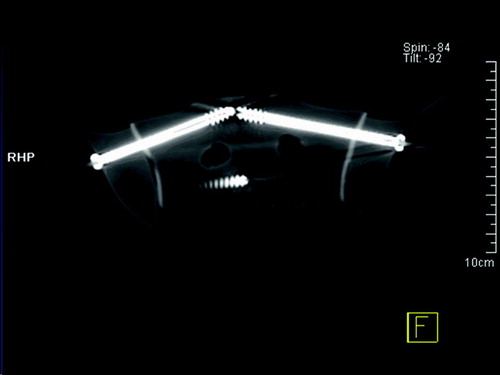
Figure 2. Postoperative evaluation with CT. All screws were analysed with direct visualization as outlined in and by CT with axial, coronal and sagittal reformation. The screws shown in this CT image were placed under Iso-C3D navigation.
Set-up for fluoroscopy-based navigated drilling
The specific “C-arm” module, available as one of the SurgiGATE® modules during the period of our study, was used (). Four projections (a.p., lateral, inlet and outlet) were acquired with the navigated C-arm (Exposcope 8000®, Ziehm, Nuremberg, Germany). The images were imported into the system and the trajectories defined according to the relative course of the S1 and S2 screws.
Figure 3. Fluoroscopy-based navigation. For 2D navigation, fluoroscopy images were acquired for simultaneous a.p., inlet, outlet and lateral projection.
Set-up for Iso-C3D-based navigated drilling
The Iso-C3D Siremobil® (Siemens, Erlangen, Germany) was used (). For the scanning the pelvis was placed on a purpose-built carbon table in the supine position. To plan the drillings it is necessary to determine exactly the volume of interest – in our series the center of S1 and S2. With a rotation of 190° around the isocenter, 100 single images were generated and converted simultaneously to 3D cut views. This data set was transferred via an interface (Navi-Link®, Siemens) to the navigation system in the mode of Iso-C3D navigation. After planning the trajectories within the multiplanar planes, the navigated drilling commenced.
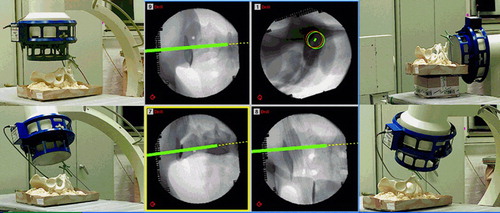
Figure 4. Set-up for Iso-C3D navigation. a) After placing the reference base on the iliac crest, an Iso-C3D scan was performed (100 images). b) The trajectories were planned in the 3D mode and drilling was performed. [Color versions available online.]
![Figure 4. Set-up for Iso-C3D navigation. a) After placing the reference base on the iliac crest, an Iso-C3D scan was performed (100 images). b) The trajectories were planned in the 3D mode and drilling was performed. [Color versions available online.]](/cms/asset/f649a332-8459-4527-921e-43b8924e4fd0/icsu_a_188924_f0004_b.jpg)
Results
With regard to the distribution of S1 and S2, it was found that all S1 screws could be placed correctly with a score of 0, and all incorrect placements were seen at S2. Sixteen (80%) of the fluoroscopy-based drillings were correct. Minimal perforation of the cortex (score = 1) was seen with 3 (15%) screws (S1 = 1, S2 = 2), and a more severe perforation (score = 2) with 1 (5%) screw (at S2). No perforation was seen with the Iso-C3D-navigated drillings.
Discussion
Percutaneous sacroiliac screw fixation is a frequently used minimally invasive surgical technique. For safe positioning of the screw, the drill bit must be controlled in four views Citation[18]. As this surgical technique is associated with radiation exposure for the surgeon, screw malpositioning can cause nerve injuries.
Navigation systems were introduced to increase the accuracy of surgical procedures and to decrease radiation exposure during operations. It was previously shown that use of navigation systems could reduce radiation exposure in other procedures Citation[19], and an experimental study involving implantation of a dynamic hip screw found that the radiation dose could be reduced by 93% Citation[20] with navigation.
Our results show that a higher proportion of sacroiliac screws could be placed accurately with Iso-C3D navigation than with conventional C-arm-based navigation. Of course, the 100% perfect placement of screws with Iso-C3D navigation cannot be transferred from a laboratory set-up into the clinical situation, but the difference when compared to fluoroscopy-based navigation is clear.
As the experimental set-up and surgical devices were identical for both series, the most likely reason for the difference in accuracy is one image source (the C-arm) having lower basic accuracy. It is suggested that the four views specified by Matta Citation[5] may even increase the error of fluoroscopy-based navigation. However, 2D navigation has been successfully used for percutaneous screw placement in the pelvis Citation[21]. Another clear advantage of Iso-C3D navigation is the availability of a 3D tool for precise, postoperative 3D analysis. However, the additional costs of a 3D C-arm and associated equipment such as a radiolucent table must be mentioned.
It should be emphasized that the results from this experimental set-up cannot be transferred directly into the clinical situation. Initial clinical applications reveal that the image quality with both techniques is impaired by obesity and bowel gases.
A clear limitation of Iso-C navigation is the limited data volume (119 mm3) and the problem of metallic artefacts if other implants are already present. In comparison to a CT of the pelvis, orientation is difficult, especially when trajectories are to be planned. When drilling, the images may flip according to the drill-bit axis. However, CT-based navigation is not a practical alternative due to the unknown actuality of the image data set when the fracture is manipulated. An elegant CT modality-based and registration-free navigation system has been described by Jacob et al. Citation[22]. However, this set-up is cost-intensive and can only be realized interdisciplinarily.
Conclusion
Iso-C3D navigation demonstrates superiority to fluoroscopy navigation for sacroiliac screw fixation in an experimental set-up designed to assess accuracy.
References
- Orthopedic Trauma Association Committee for Coding and Classification Fracture and dislocation compendium. J Orthop Trauma 1996; 10: V–IX
- Pohlemann T. Pelvic ring injuries: assessment and concepts of surgical management. AO Principles of Fracture Management, T P Rüedi, W M Murray. Thieme, Stuttgart 2001; 391–413
- Routt M L, Jr, Simonian P T, Swiontkowski M F. Stabilization of pelvic ring disruptions. Orthop Clin North Am 1997; 28: 369–388
- Tile M. The management of unstable injuries of the pelvic ring [editorial; comment]. J Bone Joint Surg Br 1999; 81: 941–943
- Matta J, Saucedo T. Internal fixation of pelvic ring fractures. Clin Orthop 1989, 242: 83–97
- Gorczyca J, Conner J. A beginner's experience with percutaneous iliosacral screws. Surgery of the Pelvis and Acetabulum: The 3rd International Consensus. Pittsburgh, PA 1996, October
- Routt M L, Jr, Simonian P T, Mills W J. Iliosacral screw fixation: early complications of the percutaneous technique. J Orthop Trauma 1997; 11: 584–589
- Culemann U, Pohlemann T, Hüfner T, Gänsslen A. Dreidimensionale Bewegungsanalyse nach interner Stabilisierung von Beckenringfrakturen ‐ eine Computersimulation. Unfallchirurg 2000; 103: 965–971
- Hüfner T, Pohlemann T, Gänsslen A, Geerling J, Krettek C, Tscherne H. Computer assisted surgery (CAS) for correction of a malhealed pelvic ring fracture in a young female patient (abstract). Comput Aided Surg 1999; 4: 154
- Hüfner T, Geerling J, Kfuri M, Jr, Gänsslen A, Citak M, Kirchhoff T, Sott A H, Krettek C. Computer assisted pelvic surgery: registration based on a modified external fixator. Comput Aided Surg 2003; 8: 192–197
- Kahler D M, Zura R D, Mallik K. Computer guided placement of iliosacral screws compared to standard fluoroscopic technique. Proceedings of the 5th Symposium on CAOS Computer Assisted Orthopaedic Surgery, DavosSwitzerland, February, 2000
- Stockle U, Konig B, Dahne M, Raschke M, Haas N P. [Computer assisted pelvic and acetabular surgery. Clinical experiences and indications]. Unfallchirurg 2002; 105: 886–892
- Amiot L P, Poulin F. Computed tomography-based navigation for hip, knee, and spine surgery. Clin Orthop Rel Res 2004, 421: 77–86
- Laine T, Mäkitalo K, Schlenzka D, Tallroth K, Poussa M, Alho A. Accuracy of pedicle screw insertion: a prospective CT study in 30 low back patients. Eur Spine J 1997; 6: 402–405
- Hofstetter R, Slomczykowski M, Krettek C, Köppen G, Sati M, Nolte L-P. Computer-assisted fluoroscopy-based reduction of femoral fractures and antetorsion correction. Comput Aided Surg 2000; 5: 311–325
- Euler E, Heining S, Riquarts C, Mutschler W. C-arm-based three-dimensional navigation: a preliminary feasibility study. Comput Aided Surg 2003; 8: 35–41
- Hufner T, Gebhard F, Grutzner P A, Messmer P, Stockle U, Krettek C. Which navigation when? Injury 2004; 35(Suppl 1)S-A30–34
- Matta J M. Regarding safe and effective placement of iliosacral screws. J Orthop Trauma 1996; 10: 514
- Suhm N, Jacob A L, Nolte L-P, Regazzoni P, Messmer P (2001) Surgical navigation reduces radiation doses during closed intramedullary nailing. Computer Assisted Radiology and Surgery. Proceedings of the 14th International Congress and Exhibition (CARS 2000), San Francisco, CA, 28 June-1 July, 2000, H U Lemke, M W Vannier, K Inamura, A G Farman, K Doi. Elsevier, Amsterdam, 262–266
- Hufner T, Kfuri M, Jr, Galanski M, Bastian L, Loss M, Pohlemann T, Krettek C. New indications for computer-assisted surgery: tumor resection in the pelvis. Clin Orthop 2004, 426: 219–225
- Mosheiff R, Khoury A, Weil Y, Liebergall M. First generation computerized fluoroscopic navigation in percutaneous pelvic surgery. J Orthop Trauma 2004; 18: 106–111
- Jacob A L, Regazzoni P, Steinbrich W, Messmer P. The multifunctional therapy room of the future: image guidance, interdisciplinarity, integration and impact on patient pathways. Eur Radiol 2000; 10: 1763–1769