
Abstract
Background: Meares Irlen Syndrome (MIS), otherwise known as “visual stress”, is one condition that can cause difficulties with reading. Aim: This study aimed to compare the effect of two coloured-filter systems on the symptoms of visual stress in children with reading delay. Methods: The study design was a pre-test, post-test, randomized head-to-head comparison of two filter systems on the symptoms of visual stress in school children. A total of 68 UK mainstream schoolchildren with significant impairment in reading ability completed the study. Results: The filter systems appeared to have a large effect on the reported symptoms between pre and post three-month time points (d = 2.5, r = 0.78). Both filter types appeared to have large effects (Harris d = 1.79, r = 0.69 and DRT d = 3.22, r = 0.85). Importantly, 35% of participants’ reported that their symptoms had resolved completely; 72% of the 68 children appeared to gain improvements in three or more visual stress symptoms. Conclusion and significance: The reduction in symptoms, which appeared to be brought about by the use of coloured filters, eased the visual discomfort experienced by these children when reading. This type of intervention therefore has the potential to facilitate occupational engagement.
Introduction
Meares-Irlen Syndrome (MIS), otherwise known as “visual stress”, occurs in 5–20% of the population (Citation1); it is thought to be one of the key visual causes of reading difficulties. Symptoms include letters appearing to blur, move around or go double, glare, and headaches (Citation2). The aetiology of these is a contested topic and has been extensively discussed elsewhere (Citation3). Some people find coloured filters help to reduce or stop the symptoms, either when used as overlays on text or when used in spectacles; this type of intervention has been found to ease the discomfort experienced and to improve reading accuracy (Citation4,5).
Health conditions that limit occupational engagement can lead to occupational deprivation (Citation6); such deprivation reduces the learning opportunities essential for child development and quality of life. As such, facilitating engagement in reading is within the domain of occupational therapy; interventions and assistive technologies that support reading need to be tested to examine their efficacy for inclusion in occupational therapy practice.
The Occupational Therapy Practice Framework (Citation7) highlights how essential reading is to participation in a range of daily living activities: preparing and reading shopping lists and selecting appropriate items when shopping, reading religious texts to undertake religious observance, accessing public transport through written timetables to allow for community mobility, all rely on reading performance. For children, participating in play, reading school books, and reading prior to bedtime (sleep preparation), are also heavily dependent on the ability to read (Citation7).
Reading is needed in work activities, managing finances, and managing medication (Citation7). It is therefore important that professionals intervene to remediate reading difficulties in order to prevent occupational performance problems in adulthood.
Failure to master basic literacy skills in the primary school years has been estimated to cost the UK taxpayer between £5000 and £43,000 per individual to the age of 37 (Citation8). If the filters allow a substantial number of children to read without the symptoms of visual stress, there would be clinical, educational, and cost benefits.
Coloured filters can be used in spectacles. These have been developed by educationists and researchers such as Irlen, Wilkins, Fowler, Harris, and Stein. In this form they have more far-reaching applications; they can filter light during both reading and writing tasks, on paper, computer screens, or white boards. There has been one preliminary occupational therapy research study investigating the effects of coloured filters on occupational performance; however, this was specific to children with a dual disorder of developmental coordination disorder (DCD) and visual stress. It was found that the coloured filters improved occupational performance in five out of the six participants, suggesting the potential value of this type of assistive equipment in supporting occupational engagement (Citation9). Randomized controlled trials, examining the efficacy of coloured filtered lenses, commenced in the early 1990s. Beneficial effects were demonstrated through a range of outcomes: reductions in visual stress symptoms including eyestrain and headache (Citation10); improved reading accuracy and comprehension (Citation4); improved reading speed (Citation11) and improved reading ability, motion sensitivity, convergence, and accommodation control (Citation12). Sustained voluntary use of coloured filter lenses was found to be almost at the 80% level, demonstrating that the individuals experienced continued benefits (Citation13,14).
Some studies have not found beneficial effects: for example, Menacker et al. (Citation15) failed to show any effect of coloured glasses on reading, but it appears that they did not use the full range of colours that the manufacturers require; thus their study protocol may have limited any potential benefits of that particular lens system. In addition, Menacker et al. (Citation15) used inappropriate selection criteria as they chose to study people with dyslexia, not people with visual stress. Since not all people with dyslexia have a significant degree of visual stress (Citation16), it is likely that only some of Menacker and colleagues’ participants had visual stress; it is not surprising therefore that they did not find a significant effect.
The UK College of Optometrists, which aims to provide a balanced view of the evidence on the topic, supports the use of individually prescribed coloured filters to ameliorate the symptoms of visual stress (Citation17). Visual stress can be part of a dyslexic profile or stand-alone as a condition in its own right (Citation16). Interestingly, for people with dyslexia, the American Pediatrics Association does not advocate the use of colour; they state conclusively that reading difficulties are not caused by visual perceptual deficits and have recommended that coloured filters are not offered in practice (Citation18). Provision of coloured filters to reduce symptoms of visual stress thus clearly remains a contentious issue.
As the use of coloured filters for treating the symptoms of visual stress is disputed, further research is needed to test the efficacy of this intervention. Here we present a trial to examine the effect of two coloured-filter systems on the symptoms of visual stress in children with reading delay.
Material and methods
The study design was a pre-test, post-test, randomized head-to-head comparison of the effects of two coloured-filter systems (Harris Foundation (Citation19) and Dyslexia Research Trust (Citation20) (DRT) systems) on the symptoms of visual stress in primary school children. These two systems were selected as the Local Education Authority requested that two filter systems with relatively simple screening procedures were tested. It was felt ethically unjustified to use a control group in the design as no benefit had been achieved with placebo filters during independent trials of these types of filters (Citation21,22). Ethics approval was gained from Oxford Research Ethics Committee (01.02) by JS. The full study design has been reported elsewhere as the data were collected as part of a trial which examined the effect of the filter systems on reading and spelling ability (Citation22). The effect of the two colour-filter systems on the symptoms of visual stress is reported here.
Participants
Mainstream schoolchildren with a significant impairment in reading capacity, defined as at least 18 months behind that expected for their age, were included in the study. The 18-month reading lag was selected by the research team as it represented a sufficiently large delay to indicate reading difficulties but still remained within the realms of a child’s normal academic ability. Children were required to be between the ages of seven and 10; they needed to be old enough to manage to wear spectacles but young enough to be learning to read. The Head of Special Educational Needs of one Local Education Authority in England identified 87 children fulfilling the inclusion criteria using records held on their own database.
Recruitment
The Local Education Authority gave permission for primary schools to recruit the identified sample. Following the head teacher’s permission, the parents of these children were invited to give written informed consent for their child to join the study. All 87 initially consented, but one parent later withdrew consent leaving a total of 86 participants for the study.
Procedure
Baseline testing
Baseline testing of both visual and psychometric measures was conducted by one of the research team (RH). He had been trained by an orthoptist and a psychologist to undertake these respective tests. The children’s visual capacity was tested, e.g. convergence, accommodation, and visual acuity, and where there were any concerns they were referred to an optometrist to remedy any defects before being included in the trial. The British Abilities Scales (BAS II) subtests of similarities, matrices, recall of digits, reading, and spelling were used to test general academic ability and literacy. Age was the final baseline variable collected. The general academic capacity of the children was found to be within normal limits, but as expected their reading and spelling were much worse, being 1.3 SD behind the population mean (10th percentile).
Dependent variables
The dependent variables measured were the number and type of visual stress symptoms experienced by the children; the symptoms were measured for each child before and after wearing the filters for at least 30 minutes a day over a three-month period. A list of common symptoms, which had been agreed by a group of education and health experts with extensive research experience of visual stress, were used to measure the symptoms experienced; a slightly condensed free version of this questionnaire has recently been published online (Citation23). The nature of the questions was similar to those included in other published validated questionnaires (Citation24,25), but they differed in that they provided a shortened, simplified version, which was felt to be more suitable for use with young children. Pre-intervention and post-intervention the questionnaire was used with participants; they were individually asked if they experienced any of the symptoms when reading (see ). They were asked to answer “yes” or “no” to each question. Words like “halo”, “aura”, and “glare” were discussed to ensure the child understood the questions. The rationale for asking the child about the presence of MIS symptoms is to identify whether they experience these symptoms; these symptoms would interfere with their ability to see the letters clearly and to be able to track their eyes along the line of letters. Children with reading difficulties are likely to develop delays in their reading ability.
Table I. Survey questions.
The scores were used to determine whether there had been a statistically significant effect of intervention on type and number of symptoms across time points and across type of filter.
Intervention procedure
Random allocation of filter systems to schools
An independent researcher, using a table of random numbers, assigned the Harris filters to one of two groups of schools, selected to be of equivalent socio-economic status. DRT filters were assigned to the other group. Allocation to group produced 42 participants for the Dyslexia Research Trust filters and 44 participants for the Harris filters; the allocations were held in sealed envelopes, which were not opened until after baseline testing had occurred. Once baseline tests had been carried out, children were offered the filter system assigned to that school. At baseline there were no statistical differences between groups according to filter type allocated.
Selection of filter colour for individual children
The children went through either the Harris Foundation or Dyslexia Research Trust procedure for selecting the appropriate individualized colours. The methods used to select the filters followed the protocols prescribed by the filter designers: the researcher (RH) had been trained by the two filter companies to determine optimal selection of the coloured filter for the child and undertook the selection process with the children. With regard to choice of colours, DRT offers two sets of spectacles: one with two blue lenses; the other with two yellow lenses. The Harris Foundation offers a larger number of colours and tests a different tint for each eye. The Harris Foundation company keeps confidential the number of colours and range of colours it uses. DRT filters took less than five minutes to select per child and Harris filters took approximately 15–30 minutes.
Pre-intervention procedure
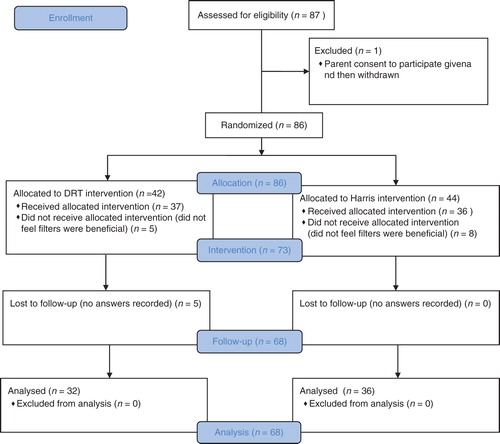
A total of 86 participants were surveyed for type and number of symptoms of visual stress at the pre-intervention stage. At baseline, of the 11 surveyed symptoms of visual stress, 86 of children interviewed experienced a mean of 5.3 symptoms (SD 2.5), with a range of between 0 and 10 symptoms. Participants were then offered the filter to look through. Five of the DRT group and eight of the Harris group did not find the filters beneficial. Those 13 who did not feel the filters were helpful had a lower level of symptoms (m = 3.46, SD = 1.94) than those 73 who found the filters helpful (m = 5.60, SD = 2.50). This was a statistically significant difference (t = 3.03, p = 0.003). The 73 (85%) children who said that the filters did make the letters look clearer, or stopped the letters moving, were asked to use the colour in spectacles for the next three months, for reading and writing work; 37 used DRT filters and 36 used Harris filters; in total 73 children received the intervention.
Children were asked, by the teacher, to wear the filters for at least 30 minutes per day at school for reading activity, whether for book or whiteboard tasks. Compliance was ascertained through individual teacher report. Parents were not actively involved in the intervention. After three months the children were asked again about their symptoms using the questions in : this was undertaken by another researcher (NR). The children were told not to bring their filters with them or to share what type of filters they had used. NR was not given any of the baseline data or made aware of which filters the child had used.
Five participants were lost at the follow-up stage; of the five, four participants were not available for retesting and one participant’s data could not be recorded as they gave unclear answers: all five were in the Dyslexia Research Trust group. Those who dropped out at follow-up did not have a different number of symptoms from those who were followed up (t = 0.56, p = 0.58). Sixty eight participant data sets were included in analysis (DRT n = 32, Harris n = 36). Analysis was undertaken by PH (see ).
Figure 1. CONSORT flow diagram.
Results
Type of symptoms experienced pre- and post-intervention
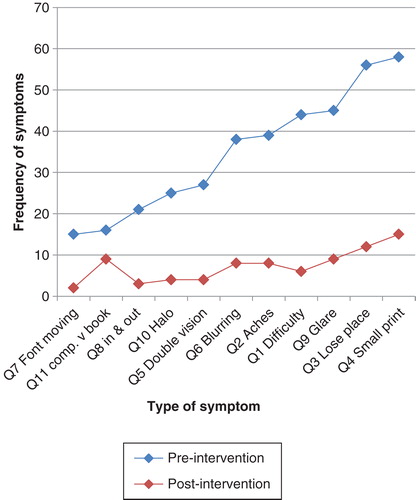
Pre-intervention the frequency with which the different types of symptoms were experienced was high (mean 35, SD 15.1, range 15 to 58, n = 68) (see ). For example: difficulty reading small print was experienced by 58 of the 68 participants. The letters moving was the least experienced symptom, but it was still experienced by 15 of the participants.
Table II. Frequency of symptom type experienced (n = 68).
Post-intervention, frequency of symptoms had reduced across all types experienced (by mean 7.27, SD 3.97, range 2–15; see ). There was a significant reduction in symptoms (mean 27.23) but the reduction was quite wide-ranging (SD 12.2) with some symptoms reduced much more than others. Those that had reduced the most were the ones that had been most frequent pre-intervention. The intervention had a large effect on the symptoms of the group between pre and post time points (d = 2.5, r = 0.78).
Figure 2. Type of symptoms experienced pre- and post-intervention (n = 68).
Number of symptoms experienced pre- and post-intervention
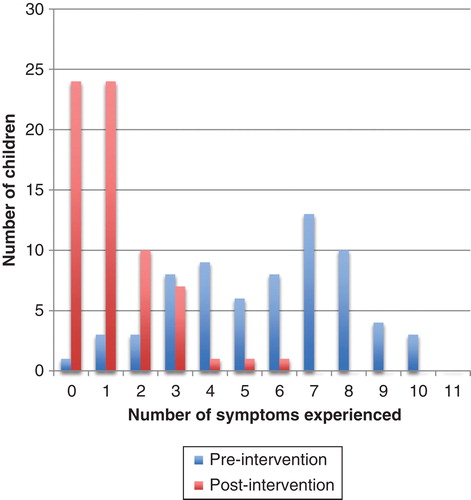
On average, the pre-intervention symptoms of visual stress per child were significantly reduced; pre-intervention the individual mean number of symptoms per child was 5.65 (SD = 2.5), post intervention the mean per child was 1.18 (SD = 1.28). Overall, it was found that there was a statistically significant reduction in the symptoms (t = 13.34, p < 0.001) with the intervention having been found to produce a large effect (d = 2.29, r = 0.75).
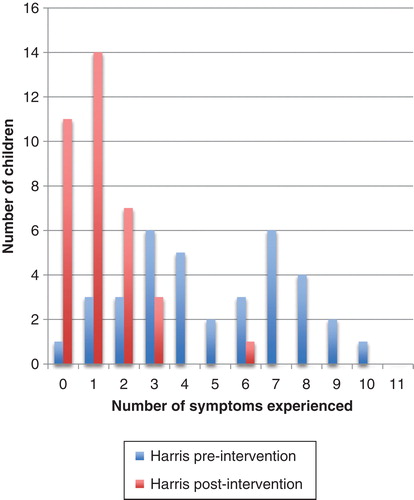
The most common number of symptoms experienced was seven and the maximum number of symptoms experienced by an individual participant was 10 (see ). Post-intervention the total number of symptoms experienced had dropped to 80, a drop of 80%. Importantly 24 (35%) participants’ symptoms had resolved completely and in 24 participants their symptoms had reduced to only one type. In all, 72% of the 68 children gained improvements in three or more of the visual stress symptoms.
Figure 3. Number of children experiencing symptoms pre- and post-intervention (n = 68).
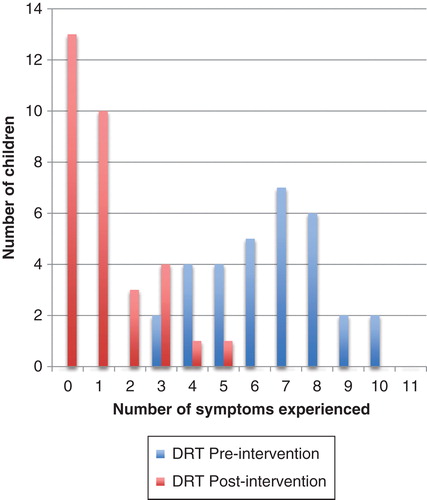
Both groups reported a large reduction in symptoms (Harris d = 1.79, r = 0.69 and DRT d = 3.22, r = 0.85) and this effect was significantly greater in the group with DRT filters (m = 5.28, SD = 2.10) than the group with Harris filters.
Of those who received the DRT filters, 13 (40%) participants’ symptoms had resolved completely and 10 (31%) reduced to experiencing only one symptom. The maximum number of symptoms dropped from 10 to five symptoms (see ).
Figure 4. Number of symptoms experienced by participants using DRT filters pre- and post-intervention (n = 32).
Of those who received the Harris filters, 11 (30%) participants’ symptoms had resolved completely and 14 (39%) reduced to experiencing only one symptom. The maximum number of symptoms dropped from 10 to six symptoms with all but one experiencing three symptoms or less (see ).
Figure 5. Number of symptoms experienced by participants using Harris filters pre- and post-intervention (n = 36).
For those using the Harris filters, on average, the symptoms of visual stress were reduced (n = 36); pre-intervention the mean number of symptoms was 4.49 (SD = 2.67) and post-intervention their mean number of symptoms was 1.19 (SD = 1.24).
Discussion
The children experienced high rates of the symptoms characteristic of visual stress. Symptoms that were experienced included font moving, blurring, glare, double vision, and headaches as identified by Stein and Fowler (Citation2) as well as eyestrain and headache as identified by Wilkins (Citation10). For children experiencing headaches, who also have a reading delay, visual stress needs to be considered by clinicians as a possible cause of their symptoms. For intelligent children the reading delay may be less apparent and so headaches are more indicative of possible visual stress.
Of children who chose not to try filters, or said they did not help, half had five or six symptoms and half had two symptoms or less. Interestingly, none of the 10 said the font moved; it maybe this is a particularly disabling symptom and unless it is present the child does not wish to wear the filters. Some children may not have wished to wear the filters due to perceived social stigma.
There is no cut-off score for visual stress symptoms at present. A cut-off score is not sought as it is recognized that the symptoms are not equally weighted and the symptoms may affect children in different ways – indeed the effect of one symptom could be very disabling to an individual child. By avoiding a cut-off score, it is possible to ensure no symptomatic child is excluded from being offered a potentially beneficial intervention.
The presence of visual stress symptoms appears high in children with reading delay. It may be that some of these children have dyslexia but others may have different conditions (Citation13). A large prevalence study of both selected and unselected samples would be useful to establish prevalence rates in the UK. Refinement of robust measures for the symptoms of visual stress and further development of standardized protocols for the administration of such tests could be published to assist parents, teachers, and other professionals to screen children for this condition and provide outcome measures for testing interventions.
It is apparent that the filters reduced the number and range of the children’s visual stress symptoms, suggesting that coloured filters are helpful in treating this type of condition. However, when trying the filters, at the point of entry into the trial, 13 children did not feel they were beneficial and chose not to wear them. Thus coloured filters may not be beneficial for all children experiencing visual stress symptoms. Perhaps these were the children who were more highly represented in the studies of Menaker et al. (Citation15), who did not report a positive effect of filter use.
We took a population of children with reading delay sufficient to recruit to a trial; of those a large number experienced MIS symptoms. We have not undertaken a prevalence study and so cannot make generalizations about symptom level in those with reading delay or those in the general population. Our trial did not include a control group; the rationale for this decision was presented in the methods section. However, we recognize this is a limitation of the study as, had a control group been included, concern related to any placebo effect could have been alleviated. We can discuss the relative effect of the filters on children with reading delay, by comparing the effect of two systems across pre- and post intervention-time points but not the absolute effect as compared with a control group.
It is interesting to note that the beneficial effects of the coloured filters on visual stress symptoms were mirrored by reading improvements, as measured by increases in BAS s scores, in a parallel study in the same children (Citation22); after wearing either kind of filter for three months both the DRT and the Harris Foundation groups had improved their BAS s scores: for DRT by 1.8 and Harris by 1.7: equivalent to an average of 4.5 months over the three months, i.e. 1.5 months more than you would expect for an average child’s progress. The BAS scoring system accounts for maturation as it is based on normalized data; this is recognized as a robust measure of reading ability. In addition the DRT filters, which had a more beneficial effect on visual stress symptoms, were also found to have had more effect on spelling ability and certain types of reading speed than those of participants using the Harris system (Citation22).
Children in the trial had been receiving support from a Special Educational Needs Co-ordinator due to their reading delay and yet they were still more than 18 months behind with their reading. For 35% of the children in the trial, their symptoms were completely resolved by wearing the filters. For these children it is apparent that filter use was very beneficial.
The process needed to support such children with reading delay can depend on a number of factors. Some governments have stopped automatic eye checks for children starting school. This could be usefully reintroduced as visual problems may be a common cause of illiteracy. We recommend that any child who is struggling to learn to read should visit an optometrist as there maybe an underlying medical condition which need addressing. If the eye itself is healthy then coloured filters could be trialled to identify whether this aids reading ability.
The different manufacturers have different processes for referral and provision. There are a range of filter manufacturers who offer this type of service and their details can be found on the World Wide Web (Citation23). Some, such as Cerium’s Intuitive Colorimeter lenses, have to be prescribed by an optometrist. Health and educational professionals can refer children to optometrists who advertise this type of service. The Irlen Institute and Harris Foundation train their own assessors; training can be undertaken by health or education professionals or referrals made to the trained assessors. Screening tools and protocols for DRT lenses are freely available for use by professionals and parents at a dedicated website http://www.colouredlensesandvisualstress (Citation23); alternatively assessment can be arranged by booking through the DRT website services. The spectacles containing the DRT filters have been distributed through primary schools by form teachers, occupational therapists, Special Educational Needs Coordinators, and head teachers.
Screening for the symptoms of visual stress and facilitation of the provision of filters for those who find them beneficial could be a valuable collaborative opportunity for teachers and occupational therapists to support children with reading difficulties. If children are enabled to read text they can improve their reading performance. Reading performance is essential for academic achievement in a range of subjects and can therefore influence potential for academic achievement and future career choice. Reading is also essential for a range of activities of daily living. In these ways enabling children to read can support occupational engagement in all three domains of self-care, work, and leisure. Provision of coloured filters for these children could be a clinically and educationally effective intervention.
Declaration of interest: One of the authors developed one of the filter systems tested in this research study; however, the author makes no financial profit from the sale of these filters as they are distributed through a non-profit organization. Every measure has been taken in the study design and execution to ensure that the study has been conducted without risk of bias. The authors alone are responsible for the content and writing of the paper.
References
- British Dyslexia Association. Eyes and dyslexia. Available from http://www.bdadyslexia.org.uk/about-dyslexia/further-information/eyes-and-dyslexia.html. accessed 2 February 2012.
- Stein JF, Fowler MS. Effect of monocular occlusion on visuomotor perception and reading in dyslexic children. Lancet 1985;326:69–73.
- Kruk R, Sumbler K, Willows D. Visual processing characteristics of children with Meares-Irlen syndrome. Ophthalmic Physiol Opt 2008;28:35–46.
- Robinson GL, Foreman PJ. Scotopic sensitivity/Irlen syndrome and the use of coloured filters: a long-term placebo-controlled and masked study of reading achievement and perception of ability. Percept Mot Skills 1999;88:83–113.
- Wilkins AJ, Evans BJW, Brown J, Busby A, Wingfield AE, Jeanes R, et al. Double-masked placebo-controlled trial of precision spectral filters in children who use coloured overlays. Ophthalmic Physiol Opt 1994;14:365–70.
- Whiteford G. Occupational deprivation: global challenge in the new millennium. Br J Occup Ther 2000;63:200–4.
- American Occupational Therapy Association. Occupational therapy practice framework: domain & process. Am J Occup Ther 2008;62:625–83.
- Every Child a Chance Trust. The long term costs of literacy difficulties. 2nd ed. London: KPMG/Every Child a Chance Trust; 2009.
- Konarski M, Taylor MC. A preliminary qualitative investigation of the effect of prescribed coloured lenses on occupational performance. Optom Today 2010;42–7.
- Wilkins AJ. Reading through colour: how coloured filters can reduce reading difficulty, eye strain, and headaches. Chichester: Wiley; 2003.
- Bouldoukian J, Wilkins A, Evans B. Randomised controlled trial of the effect of coloured overlays on the rate of reading of people with specific learning difficulties. Ophthalmic Physiol Opt 2002;22:55–60.
- Ray NJ, Fowler S, Stein JF. Magnocellular function: motion sensitivity, convergence, accommodation, and reading. In Ramat S, Straumann D, editors. Clinical and basic oculomotor research: in honor of David S. Zee. New York: New York Academy of Sciences; 2005. p 283–93.
- Evans B, Patel R, Wilkins A, Lightstone A, Eperjesi F, Speedwell L, et al. A review of the management of 323 consecutive patients seen in a specific learning difficulties clinic. Ophthalmic Physiol Opt 1999;19:454–66.
- Maclachlan A, Yale S, Wilkins A. Open trial of subjective precision tinting: a follow-up of 55 patients. Ophthalmic Physiol Opt 1993;13:175–8.
- Menacker S, Breton M, Breton M, Radcliffe J, Gole G. Do tinted lenses improve the reading performance of dyslexic children? A cohort atudy. Arch Ophthalmol 1993;111:213–18.
- Kriss I, Evans B. The relationship between dyslexia and Meares-Irlen syndrome. J Res Read 2005;28:350–64.
- Allen PM, Evans BJW, Wilkins AJ. The uses of colour in optometric practice to ameliorate symptoms of visual stress. Optom Pract 2012;13:1–8.
- Handler SM, Fierson WM; Section on Ophthalmology; Council on Children with Disabilities; American Academy of Ophthalmology; American Association for Pediatric Ophthalmology and Strabismus; American Association of Certified Orthoptists. Learning disabilities, dyslexia, and vision. Pediatrics 2011;127:e818–56.
- Harris Foundation. Available from http://www.harrisdyslexia.com. accessed 22 February 2012.
- Dyslexia Research Trust. About us. Available from http://www.dyslexic.org.uk. accessed 22 February 2012.
- Harris D, MacRow-Hill SJ. Application of ChromaGen haploscopic lenses to patients with dyslexia: a double-masked, placebo-controlled trial. J Am Optom Assoc 1999;70:629–40.
- Hall R, Ray N, Harries P, Stein J. A comparison of two-coloured filter systems for treating visual reading difficulties. Disabil Rehabil. 2013. 35:2221–6. Available from http://www.ncbi.nlm.nih.gov/pubmed/23627538.
- Harries PA, Fowler L, Parker C, Perkins L, Wignall S, Manalpara E. A resource for parents and professionals to support them through the process of helping children with visual stress [computer software]. 2012. Retrieved from http://www.colouredlensesandvisualstress.com/.
- Borsting EJ, Rouse MW, Mitchell GL, Scheiman M, Cotter SA, Cooper J, et al. Validity and reliability of the revised convergence insufficiency symptom survey in children aged 9 to 18 years. The CITT Study Group. Optom Vis Sci 2003;80:832–8.
- Conlon E, Lovegrove W, Chekaluk E, Pattison P. Measuring visual discomfort. Vis Cogn 1999;6:637–66.