Abstract
Objective. To evaluate the effectiveness of sildenafil versus continuous positive airway pressure (CPAP) for patients with erectile dysfunction (ED) and obstructive sleep apnea (OSA).
Methods. This is a meta-analysis of a randomized controlled trial. The main outcome measures for effectiveness were the percentage of successful intercourse attempts, International Index of Erectile Function (IIEF) domain scores (erectile function, EF) and the satisfaction levels of the patients and their partners with the treatment for ED.
Results. Two randomized controlled trials totaling 70 patients were included. Meta-analysis results are as follows: after 12 weeks of treatment, patients under sildenafil demonstrated a significant advantage over under CPAP in terms of the percentage of successful intercourse attempts [OR = 3.24, 95% CI (2.37–4.43)], EF scores [WMD = 3.57, 95%CI (1.68–5.45)], and the satisfaction levels of the patients and their partners with the treatment for ED [OR = 3.56, 95% CI (1.27–9.98)].
Conclusion. Current clinical studies might confirm that both therapeutic methods were safe and effective, but sildenafil was superior to CPAP in the treatment of ED in men with OSA. We conclude that new therapeutic agents or a combination of the two methods should be studied further.
Introduction
Erectile dysfunction (ED) is defined as the inability of a man to attain or maintain an erection long enough to complete the sexual act [Citation1], and it affects over half of all men between 50 and 70 years of age [Citation2]. From a biological point of view, this high prevalence underscores the fact that ED is in reality a part of the aging process. The determinants of whether and at what age man becomes dysfunctional are probably related to a number of genetic and environmental factors. For example, many disease states [e.g. obstructive sleep apnea (OSA), diabetes, hypertension, depression, and vascular disease] are associated with ED, and the development of ED in these men is extremely variable, occurring at times many years before the onset of these disorders.
OSA was clearly documented for the first time in 1966 [Citation3] and is characterised by upper airway narrowing or collapse resulting in repetitive episodes of hypoxaemia, swings in intrathoracic pressure and sleep fragmentation from arousals. Anatomical causes of upper airway collapse are the most frequent cause of OSA [Citation4]. It is highly prevalent in the middle age active population [Citation5,Citation6]. The consequences of obstructive breathing disturbances on sleep structure and continuity, tissue oxygenation, hemodynamic variables and on the release of systemic inflammatory mediators can account for vigilance and quality of life impairments [Citation7] as well as for the increase in morbidity and mortality [Citation8–11].
OSA is recognized as a risk or even an etiological factor for ED. On the other hand, sleep-disordered breathing has been reported by many patients with ED. Sildenafil prolongs the action of cyclic guanosine monophosphate and nitric oxide (NO) by inhibiting cyclic guanosine monophosphate-specific phosphodiesterase 5. In March 1998, the US Food and Drug Administration (FDA) approved sildenafil citrate (Viagra®, Pfizer, New York, NY) for the treatment of ED [Citation12]. As of December 2005, more than 27 million men worldwide had received sildenafil for treatment of ED, including an estimated 17 million men in the US (Data on file, Pfizer, New York, NY). It is largely used for ED, a highly prevalent condition in OSA. CPAP represents a very effective treatment for OSA as demonstrated by the results of different randomized controlled [Citation13–16] and non-randomized trials [Citation17]. A positive airway pressure device is basically an air pump (fan-driven or turbine system) that draws in external, filtered air and delivers pressurized airflow, which is adjustable by varying the pressure valve diameter or fan/turbine speed.
A dearth of NO has been implicated for the development of the OSA consequences [Citation18]. ED, as a result of endothelial dysfunction, is often related with diabetes mellitus, atherosclerosis, hypertension and coronary artery disease; almost all are long-term complications of OSA. Thus, the impairment of NO vasoprotective function may explain the association between OSA and ED and may also indicate optimal therapeutic management. Perimenis et al. study 70 demonstrated that both sildenafil 100 mg and CPAP, used separately, had positive therapeutic impact but sildenafil was superior [Citation19,Citation20]. Therefore, we carried out a meta-analysis to determine the effectiveness of sildenafil versus CPAP for patients with ED and OSA.
Methods
Search strategy
We searched Pubmed (1966–2008), Embase (1974–2008), the Cochrane Library (2008 issue 3), Chinese biomedicine literature database (1978–2008), Chinese technological periodical full-text database (1989–2008.10), and Chinese periodical full-text database (1994–2008.10) for randomized controlled trials comparing sildenafil with CPAP. We searched key Chinese magazines of related fields manually, used search engines such as Google™ to search related references on the internet, and searched the references of included studies. Hand searching of the reference lists of included studies and reviews was undertaken and contact was made with experts in the field, unpublished studies were not sought. No limits based on language were imposed.
The search strategy described was used to obtain titles and abstracts of randomized controlled trials that were relevant to this review. The titles and abstracts will be screened independently by two reviewers (ZhiLong Dong) and (YiXin Wan), who will discard studies that are not applicable, and two reviewers will independently assess retrieved the titles and abstracts of all identified trials to confirm fulfillment of inclusion criteria. Disagreements will be resolved in consultation with ZhiPing Wang. Data extraction will be carried out independently by the same authors using standard data extraction forms. The quality items assessed were randomization, allocation concealment, blinding (participants, investigators, outcome assessors, and data analysis), and completeness of follow-up.
Inclusion criteria
All patients were monitored two consecutive nights for diagnosis and one additional night for therapeutic titration by a polygraph data recording system for the following parameters: electroencephalogram, electro-oculogram, chin, intercostal and bilateral anterior tibialis electromyography, electrocardiogram, nasal and buccal thermistors to assess air exchange, tachograph for beat-to-beat heart rate and ear oxymetry for blood oxygen saturation. Sleep stages and events were scored manually according to standard criteria [Citation21]. Patients were asked to answer Questions 3 and 4 of the International Index of Erectile Function (IIEF) questionnaire. When the score was 4 or less for both questions they were referred for andrologic evaluation if they agreed.
Types of outcome measures
The percentage of successful intercourse attempts, IIEF domain scores (EF) and the satisfaction levels of the patients and their partners with the treatment for ED were included.
Types of intervention
Types of intervention were sildenafil versus CPAP.
Statistical analysis
We analyzed the data using Review Manager (version 5.0) and extracted and pooled data for summary estimates. We expressed results for dichotomous outcomes as relative risk with 95% confidence intervals (CI) and continuous outcomes as weighted mean difference or standard mean difference. We used the χ2 statistic to assess heterogeneity between trials and the I2 statistic to assess the extent of inconsistency. We used a fixed effect model for calculations of summary estimates and their 95% CI unless there was significant heterogeneity, in which case results were confirmed using a random effects statistical model. Subgroup analyses were intended to explore important clinical differences among that might be expected to alter the magnitude of treatment effect.
Results
Search results
We identified 22 potentially eligible trials and subsequently excluded 20 trials for the following reasons: 10 were not randomized; seven were missing test group or control group; three were abstracts referring exclusively to limited disease or treatments other than sildenafil or continuous positive airway pressure (CPAP) regimen; Two randomized controlled trials totaling 70 patients were included [Citation19,Citation20]. The two trials all reported three types of outcome including the percentage of successful intercourse attempts, EF scores, and the satisfaction levels of the patients with the treatment for ED. In both groups, patients were matched for age, severity of OSA and ED duration. Comorbidities such as diabetes mellitus, atherosclerosis, hyperlipidemia, coronary artery disease and hypertension were evenly distributed in both groups.
The quality and characteristics of included studies
The quality and characteristics of included studies are shown in .
Table I. The quality and characteristics of included studies.
Meta-analysis results
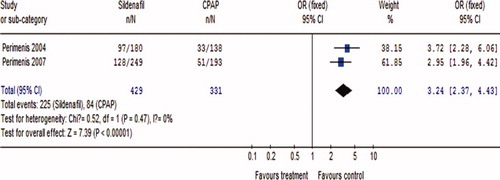
Treatment efficacy: After 12 weeks of treatment, patients under sildenafil demonstrated a significant advantage over under CPAP in terms of the percentage of successful intercourse attempts [OR = 3.24 95% CI (2.37–4.43)]. The result of the attempts for intercourse in two groups is depicted in .
Figure 1. The percentage of successful intercourse attempts for sildenafil versus CPAP.
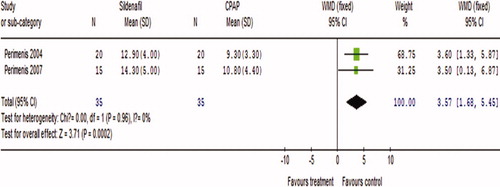
IIEF domain scores (EF scores) were increased in both groups compared to baseline (). In patients under sildenafil and CPAP, the EF scores after treatment were higher than before. However, post-treatment, EF scores () were significantly higher in men treated with sildenafil than in men treated with CPAP [WMD = 3.57, 95% CI (1.68–5.45)].
Figure 2. EF scores before treatment for sildenafil versus CPAP.
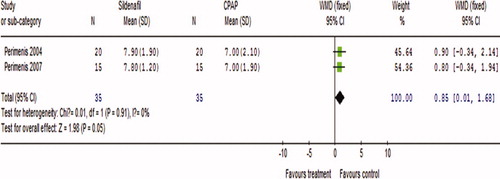
Figure 3. EF scores after treatment for sildenafil versus CPAP.
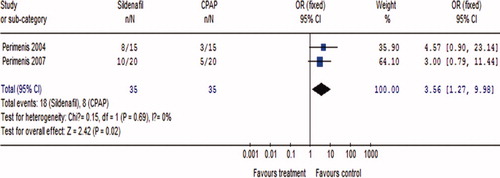
At the end of study, patients receiving sildenafil demonstrated a significant advantage in terms of the satisfaction levels of the patients and their partners with the treatment for ED, compared with patients receiving CPAP [OR = 3.56 95% CI (1.27–9.98)], and the result is shown in .
Figure 4. Satisfaction with treatment for sildenafil versus CPAP.
Discussion
The number of the included studies is relatively small. The small number of participants and included studies, as well as the low quality of most studies in this study, might not allow for a reliable conclusion. Of the two included studies, none of the studies mentioned blinding and intention-to-treat analysis, which may produce high performance bias, measuring bias, and selective bias. Future research should clearly spell out how to implement blinding and allocation conceal. Publication bias might exist. Pharmacogenomic difference could exist between European and Asian patient populations. Future study should pay attention to the impact of geographical difference. We still need more high-quality multicenter randomized controlled trials from other countries and regions to compare the dose levels of sildenafil.
The association between OSA and ED might be explained by the impairment of NO vasoprotective function due to the respiratory disturbances during nighttime sleep. Several studies reported that oxygen therapy for 1 month resulted in the reversal of ED in men with obstructive pulmonary disease [Citation22]. CPAP provided either in the short term or for 12 weeks improved erectile function in men with OSA and ED [Citation23,Citation24]. Aasebo et al. reported a 42% reversal of ED in men with chronic obstructive pulmonary disease receiving a 1-month oxygen therapy [Citation25]. Short-term nasal CPAP also improved the impaired nocturnal penile tumescence in one-third of patients in a study of men with OSAS and ED [Citation26]. The effectiveness of CPAP may be due to the increase of NO circulating levels and the consequent improvement of endothelial cell function [Citation27].
In the present study, when the mean severity of OSA was mild, sildenafil proved to be more effective than CPAP as it resulted in a significantly higher rate of successful attempts for intercourse and increased EF scores compared to CPAP. Although sildenafil was more effective than CPAP in treating ED, approximately half of the patients were not satisfied with this treatment. Thus, it seems that none of the studied therapeutic methods met the needs and expectations of all patients. It must be noted that satisfaction was not affected by adverse events, as both therapeutic methods proved to be safe and well tolerated. It should be noted, however, that satisfaction issues should be best assessed in a blinded fashion, to exclude psychological bias on different treatment arms. This could not apply in this study due to the obviously different nature of the two treatment modalities.
Conclusion
Current clinical studies might confirm that both therapeutic methods were safe and effective, but sildenafil was superior to CPAP in the treatment of ED in men with OSA. Although there is convincing evidence to confirm the results mentioned previously, the results still need to be confirmed by large sample multicenter randomized controlled trials. We conclude that different therapeutic methods, including combinations of CPAP with sildenafil, or newer oral agents, should be studied further.
Acknowledgments
The authors thank Professor BaoLiang Ma, the Second Hospital of Lanzhou University, for his statistical consultation, and all those who willingly participated in this study.
References
- NIH Consensus Development Panel on Impotence. Impotence. JAMA 1993;270:83–90.
- Feldman HA, Goldstein I, Hatzichristou DG, et al Impotence and its medical and psychosocial correlates: results of the Massachusetts male aging study. J Urol 1994;151:54–61.
- Gastaut H, Tassinari CA, Duron B. Polygraphic study of the episodic diurnal and nocturnal (hypnic and respiratory) manifestations of the Pickwick syndrome. Brain Res 1966;1:167–186.
- Caples SM, Kara T, Somers VK. Cardiopulmonary consequences of obstructive sleep apnea. Semin Respir Crit Care Med 2005;26:25–32.
- Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med 1993;328:1230–1235.
- Hiestand DM, Britz P, Goldman M, Phillips B. Prevalence of symptoms and risk of sleep apnea in the US population: results from the national sleep foundation sleep in America 2005 poll. Chest 2006;130:780–786.
- Vgontzas AN, Papanicolaou DA, Bixler EO, et al Sleep apnea and daytime sleepiness and fatigue: relation to visceral obesity, insulin resistance, and hypercytokinemia. J Clin Endocrinol Metab 2000;85:1151–1158.
- Grote L, Ploch T, Heitmann J. Sleep-related breathing disorder is an independent risk factor for systemic hypertension. Am J Respir Crit Care Med 1999;160:1875–1882.
- Shahar E, Whitney CW, Redline S, et al Sleep-disordered breathing and cardiovascular disease: cross-sectional results of the sleep heart health study. Am J Respir Crit Care Med 2001;163:19–25.
- Peppard P, Young T, Palta M, Skatrud J. Prospective study of the association between sleep-disordered breathing and hypertension. N Engl J Med 2000;342:1378–1384.
- He J, Kryger MH, Zorick FJ, Conway W, Roth T. Mortality and apnea index in obstructive sleep apnea. Experience in 385 male patients. Chest 1988;94:9–14.
- FDA. 1998. FDA approves impotence pill, VIAGRA. Available from: http://www.fda.gov/bbs/topics/ANSWERS/ANS00857.html [Accessed 27 February 2004].
- Senn O, Brack T, Matthews F, Russi EW, Bloch KE. Randomized short-term trial of two auto-CPAP devices versus fixed continuous positive airway pressure for the treatment of sleep apnea. Am J Respir Crit Care Med 2003;168:1506–1511.
- Engleman HM, Kingshott RN, Wraith PK, Mackay TW, Deary IJ, Douglas NJ. Randomized placebo-controlled crossover trial of continuous positive airway pressure for mild sleep apnea/hypopnea syndrome. Am J Respir Crit Care Med 1999;159:461–467.
- Jenkinson C, Davies DO, Mulins R, Stradling JR. Comparison of therapeutic and subtherapeutic nasal continuous positive airway pressure for obstructive sleep apnoea: a randomized prospective parallel trial. Lancet 1999;353:2100–2105.
- Masa JF, Jimenez A, Duran J, et al Alternative methods of titrating continuous positive airway pressure: a large multicenter study. Am J Respir Crit Care Med 2004;170:1218–1224.
- Marin JM, Carrizo SJ, Vicente E, Agusti AG. Long-term cardiovascular outcomes in men with obstructive sleep apnoeahypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet 2005;365:1046–1053.
- Lavie P, Herer P, Hoffstein V. Obstructive sleep apnea syndrome as risk factor for hypertension: population study. Br Med J 2000;320:479–482.
- Perimenis P, Karkoulias K, Konstantinopoulos A, et al Sildenafil versus continuous positive airway pressure for erectile dysfunction in men with obstructive sleep apnea: a comparative study of their efficacy and safety and the patient's satisfaction with treatment. Asian J Androl 2007;9:259–264.
- Perimenis P, Karkoulias K, Markou S, et al Erectile dysfunction in men with obstructive sleep apnea syndrome: a randomized study of the efficacy of sildenafil and continuous positive airway pressure. Int J Impot Res 2004;16:256–260.
- Rechtschaffen A, Kales A. A manual of standardized terminology, techniques and scoring systemfor sleep stages in human adults. Washington: US Government Printing Office; 1968.
- Kato M, et al Impairment of endothelium dependent vasodilation of resistance vessels in patients with obstructive sleep apnea. Circulation 2000;102:2607–2610.
- Haight JSJ, Djupesland PG. Nitric oxide (NO) and obstructive sleep apnea (OSA). Sleep Breath 2003;7:53–61.
- Malhotra A, White DP. Obstructive sleep apnoea. Lancet 2002;360:237–245.
- Aasebo U, Gyltnes A, Bremnes RM, et al Reversal of sexual impotence in male patients with chronic obstructive pulmonary disease and hypoxemia with long-term oxygen therapy. J Steroid Biochem Mol Biol 1993;46:799–803.
- Low WY, Ng CJ, Tan NC, Choo WY, Tan HM. Management of erectile dysfunction: barriers faced by general practitioners. Asian J Androl 2004;6:99–104.
- Shepard JW Jr, et al Relationship of ventricular ectopy to nocturnal oxygen desaturation in patients with chronic obstructive pulmonary disease. Am J Med 1995;78:28–34.